Orbit Is the Anatomical Space Bounded
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
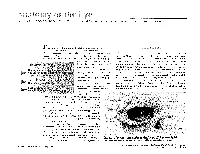
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

PE2812 Breaking Arm Bones a Second Time
Breaking Arm Bones a Second Time Children who have broken arm bones are at higher risk for breaking the same arm bones again if they do not go through the right treatment, for the right amount of time. How likely is it that There is up to a 5% chance (1 out of every 20 cases) of breaking forearm my child’s arm bones a second time, in the same place. There is a higher risk to break these bones again if the first fracture is in the middle of the forearm bones (as bones will break seen in the pictures below). There is a lower risk if the fracture is closer to again? the hand. Most repeat fractures tend to happen within six months after the first injury heals. First fracture Same fracture after healing for about 6 weeks 1 of 2 To Learn More Free Interpreter Services • Orthopedics and Sports Medicine • In the hospital, ask your nurse. 206-987-2109 • From outside the hospital, call the • Ask your child’s healthcare provider toll-free Family Interpreting Line, 1-866-583-1527. Tell the interpreter • seattlechildrens.org the name or extension you need. Breaking Arm Bones a Second Time How can I help my Wearing a cast for at least six weeks lowers the risk of breaking the same child lower the risk arm bones again. After wearing a cast, we recommend your child wear a brace for 4 weeks in order to protect the injured area and start improving of having a wrist movement. While your child wears a brace, we recommend they do repeated bone not participate in contact sports (e.g., soccer, football or dodge ball). -

Septation of the Sphenoid Sinus and Its Clinical Significance
1793 International Journal of Collaborative Research on Internal Medicine & Public Health Septation of the Sphenoid Sinus and its Clinical Significance Eldan Kapur 1* , Adnan Kapidžić 2, Amela Kulenović 1, Lana Sarajlić 2, Adis Šahinović 2, Maida Šahinović 3 1 Department of anatomy, Medical faculty, University of Sarajevo, Čekaluša 90, 71000 Sarajevo, Bosnia and Herzegovina 2 Clinic for otorhinolaryngology, Clinical centre University of Sarajevo, Bolnička 25, 71000 Sarajevo, Bosnia and Herzegovina 3 Department of histology and embriology, Medical faculty, University of Sarajevo, Čekaluša 90, 71000 Sarajevo, Bosnia and Herzegovina * Corresponding Author: Eldan Kapur, MD, PhD Department of anatomy, Medical faculty, University of Sarajevo, Bosnia and Herzegovina Email: [email protected] Phone: 033 66 55 49; 033 22 64 78 (ext. 136) Abstract Introduction: Sphenoid sinus is located in the body of sphenoid, closed with a thin plate of bone tissue that separates it from the important structures such as the optic nerve, optic chiasm, cavernous sinus, pituitary gland, and internal carotid artery. It is divided by one or more vertical septa that are often asymmetric. Because of its location and the relationships with important neurovascular and glandular structures, sphenoid sinus represents a great diagnostic and therapeutic challenge. Aim: The aim of this study was to assess the septation of the sphenoid sinus and relationship between the number and position of septa and internal carotid artery in the adult BH population. Participants and Methods: A retrospective study of the CT analysis of the paranasal sinuses in 200 patients (104 male, 96 female) were performed using Siemens Somatom Art with the following parameters: 130 mAs: 120 kV, Slice: 3 mm. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Anatomical Study of the Zygomaticotemporal Branch Inside the Orbit
Open Access Original Article DOI: 10.7759/cureus.1727 Anatomical Study of the Zygomaticotemporal Branch Inside the Orbit Joe Iwanaga 1 , Charlotte Wilson 1 , Koichi Watanabe 2 , Rod J. Oskouian 3 , R. Shane Tubbs 4 1. Seattle Science Foundation 2. Department of Anatomy, Kurume University School of Medicine 3. Neurosurgery, Complex Spine, Swedish Neuroscience Institute 4. Neurosurgery, Seattle Science Foundation Corresponding author: Charlotte Wilson, [email protected] Abstract The location of the opening of the zygomaticotemporal branch (ZTb) of the zygomatic nerve inside the orbit (ZTFIN) has significant surgical implications. This study was conducted to locate the ZTFIN and investigate the variations of the ZTb inside the orbit. A total of 20 sides from 10 fresh frozen cadaveric Caucasian heads were used in this study. The vertical distance between the inferior margin of the orbit and ZTFIN (V-ZTFIN), the horizontal distance between the lateral margin of the orbit and ZTFIN (H-ZTFIN), and the diameter of the ZTFIN (D-ZTFIN) were measured. The patterns of the ZTb inside the orbit were classified into five different groups: both ZTb and LN innervating the lacrimal gland independently (Group A), both ZTb and LN innervating the lacrimal gland with a communicating branch (Group B), ZTb joining the LN without a branch to the lacrimal gland (Group C), the ZTb going outside the orbit through ZTFIN without a branch to the lacrimal gland nor LN (Group D), and absence of the ZTb (Group E). The D-ZTFIN V-ZTFIN H-ZTFIN ranged from 0.2 to 1.1 mm, 6.6 to 21.5 mm, 2.0 to 11.3 mm, respectively. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -
The Orbit Is Composed Anteri
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Pediatric Orbital Tumors and Lacrimal Drainage System
Pediatric Orbital Tumors and Lacrimal Drainage System Peter MacIntosh, MD University of Illinois • No financial disclosures Dermoid Cyst • Congenital • Keratinized epidermis • Dermal appendage • Trapped during embryogenesis • 6% of lesions • 40-50% of orbital pediatric orbital lesion • Usually discovered in the first year of life • Painless/firm/subQ mass • Rarely presents as an acute inflammatory lesion (Rupture?) • Frontozygomatic (70%) • Maxillofrontal (20%) suture Imaging - CT • Erosion/remodeling of bone • Adjacent bony changes: “smooth fossa” (85%) • Dumbell dermoid: extraorbital and intraorbital components through bony defect Imaging - MRI • Encapsulated • Enhancement of wall but not lumen Treatment Options • Observation • Risk of anesthesia • Surgical Removal • Changes to bone • Rupture of cyst can lead to acute inflammation • Irrigation • Abx • Steroids Dermoid INFANTILE/Capillary Hemangioma • Common BENIGN orbital lesion of children • F>M • Prematurity • Appears in 1st or 2nd week of life • Soft, bluish mass deep to the eyelid • Superonasal orbit • Rapidly expands over 6-12 months • Increases with valsalva (crying) • Clinical findings • Proptosis Astigmatism • Strabismus Amblyopia INFANTILE/Capillary Hemangioma • May enlarge for 1-2 years then regress • 70-80% resolve before age 7 • HIGH flow on doppler • Kasabach-Merritt Syndrome • Multiple large visceral capillary hemangiomas • Sequestration of platelets into tumor • Consumptive thrombocytopenia • Supportive therapy and treat underlying tumor • Complications • DIC • death •Homogenous -

Stage Surgery on Inverted Papilloma Which Invaded Lacrimal Sac, Periorbita, Ethmoid and Frontal Sinus
臨床耳鼻:第 27 卷 第 1 號 2016 ••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••• J Clinical Otolaryngol 2016;27:143-147 증 례 Stage Surgery on Inverted Papilloma which Invaded Lacrimal Sac, Periorbita, Ethmoid and Frontal Sinus Jae-hwan Jung, MD, Minsic Kim, MD, Sue Jean Mun, MD and Hwan-Jung Roh, MD, PhD Department of Otorhinolaryngology-Head & Neck Surgery, Pusan National University Yangsan Hospital, Yangsan, Korea - ABSTRACT - Inverted papilloma of the nasal cavity and the paranasal sinuses is a benign epithelial tumor with a high rate of recurrence, local aggressiveness, and malignant transformation. For these reasons, inverted papilloma has been treated like malignant tumors with extensive surgical resection. With the help of endoscopic sinus surgery tech- nique, it is now available to treat inverted papilloma with stage surgery without severe complications which usu- ally resulted from extensive one stage resection. We report a case of stage surgery on inverted papilloma which invaded lacrimal sac, periorbita, ethmoid and frontal sinus. (J Clinical Otolaryngol 2016;27:143-147) KEY WORDS:Inverted papillomaㆍLacrimal sacㆍPeriorbitaㆍSurgery. Authors present a successful endoscopic stage sur- Introduction gery on IP which invaded lacrimal sac, periorbita, ethmoid and frontal sinus with the literature review. Inverted papilloma (IP) of the nasal cavity and the paranasal sinuses is a benign epithelial tumor with a Case Report high rate of recurrence, local aggressiveness, and ma- lignant transformation.1,2) For these reasons, IP has A 41-year-old female presented in outpatient clinic been treated like malignant tumors with extensive sur- with a complaint of tender swelling mass on the in- gical resection. ner side of her right eye for 5 years which suddenly IP of lacrimal sac and periorbita is rarely reported aggravated 2 months ago. -

GLOSSARY of MEDICAL and ANATOMICAL TERMS
GLOSSARY of MEDICAL and ANATOMICAL TERMS Abbreviations: • A. Arabic • abb. = abbreviation • c. circa = about • F. French • adj. adjective • G. Greek • Ge. German • cf. compare • L. Latin • dim. = diminutive • OF. Old French • ( ) plural form in brackets A-band abb. of anisotropic band G. anisos = unequal + tropos = turning; meaning having not equal properties in every direction; transverse bands in living skeletal muscle which rotate the plane of polarised light, cf. I-band. Abbé, Ernst. 1840-1905. German physicist; mathematical analysis of optics as a basis for constructing better microscopes; devised oil immersion lens; Abbé condenser. absorption L. absorbere = to suck up. acervulus L. = sand, gritty; brain sand (cf. psammoma body). acetylcholine an ester of choline found in many tissue, synapses & neuromuscular junctions, where it is a neural transmitter. acetylcholinesterase enzyme at motor end-plate responsible for rapid destruction of acetylcholine, a neurotransmitter. acidophilic adj. L. acidus = sour + G. philein = to love; affinity for an acidic dye, such as eosin staining cytoplasmic proteins. acinus (-i) L. = a juicy berry, a grape; applied to small, rounded terminal secretory units of compound exocrine glands that have a small lumen (adj. acinar). acrosome G. akron = extremity + soma = body; head of spermatozoon. actin polymer protein filament found in the intracellular cytoskeleton, particularly in the thin (I-) bands of striated muscle. adenohypophysis G. ade = an acorn + hypophyses = an undergrowth; anterior lobe of hypophysis (cf. pituitary). adenoid G. " + -oeides = in form of; in the form of a gland, glandular; the pharyngeal tonsil. adipocyte L. adeps = fat (of an animal) + G. kytos = a container; cells responsible for storage and metabolism of lipids, found in white fat and brown fat. -

Original Article Anatomic Study of the Lacrimal Fossa and Lacrimal Pathway
Original Article Anatomic study of the lacrimal fossa and lacrimal pathway for bypass surgery with autogenous tissue grafting Hai Tao, Zhi‑zhong Ma1, Hai‑Yang Wu, Peng Wang, Cui Han Purpose: To study the microsurgical anatomy of the lacrimal drainage system and to provide anatomical Access this article online evidence for transnasal endoscopic lacrimal drainage system bypass surgery by autogenous tissue grafting. Website: Materials and Methods: A total of 20 Chinese adult cadaveric heads in 10% formaldehyde, comprising www.ijo.in 40 lacrimal ducts were used. The middle third section of the specimens were examined for the following DOI: features: the thickness of the lacrimal fossa at the anterior lacrimal crest, vertical middle line, and posterior 10.4103/0301-4738.121137 lacrimal crest; the cross section of the upper opening, middle part, and lower opening of the nasolacrimal PMID: canal; the horizontal, 30° oblique, and 45° oblique distances from the lacrimal caruncle to the nasal cavity; ***** the distance from the lacrimal caruncle to the upper opening of the nasolacrimal duct; and the included Quick Response Code: angle between the lacrimal caruncle–nasolacrimal duct upper opening junction and Aeby’s plane. Results: The middle third of the anterior lacrimal crest was significantly thicker than the vertical middle line and the posterior lacrimal crest (P > 0.05). The horizontal distance, 30° oblique distance, and 45° oblique distance from the lacrimal caruncle to the nasal cavity exhibited no significant differences (P > 0.05). The included angle between the lacrimal caruncle and the lateral wall middle point of the superior opening line of the nasolacrimal duct and Aeby’s plane was average (49.9° ± 1.8°). -

Surgical Anatamic of Paranasal Sinuses
SURGICAL ANATAMIC OF PARANASAL SINUSES DR. SEEMA MONGA ASSOCIATE PROFESSOR DEPARTMENT OF ENT-HNS HIMSR MIDDLE TURBINATE 1. Anterior attachment : vertically oriented, sup to the lateral border of cribriform plate. 2. Second attachment :Obliquely oriented- basal lamella/ ground lamella, Attached to the lamina papyracea ( medial wall of orbit anterior, posterior air cells, sphenopala‐ tine foramen 3. Posterior attachment :medial wall of maxillary sinus, horizontally oriented. , supreme turbinate 3. Occasionally 4. fourth turbinate, 5. supreme meatus, if present 6. drains posterior ethmoid drains inferior, middle, superior turbinates and, occasionally, the supreme turbinate, the fourth turbinate. e. Lateral to these turbinates are the corresponding meatuses divided per their drainage systems ANATOMICAL VARIATIONS OF THE TURBINATES 1. Concha bullosa, 24–55%, often bilateral, 2. Interlamellar cell of grunwald: pneumatization is limited to the vertical part of middle turbinate, usually not causing narrowing of the ostiomeatal unit 3. Paradoxic middle turbinate: 26%,. Occasionally, it can affect the patency of the ostiomeatal unit 4. Pneumatized basal lamella, falsely considered, posterior ethmoid air cell Missed basal lamella – attaches to lateral maxillary sinus wall Ostiomeatal unit Anterior ostiomeatal unit, maxillary, anterior ethmoid, frontal sinuses, (1) ethmoid infundibulum, (2) middle meatus, (3) hiatus semilunaris, (4) maxillaryOstium, (5) ethmoid bulla, (6) frontal recess, (7) uncinate process. , sphenoethmoidal recess Other draining osteomeatal unit, posterior in the nasal cavity, posterior ethmoid sinus, lateral to the superior turbinate, . sphenoid Sinus medial to the superior turbinate Uncinate Process Crescent‐shaped, thin individual bone inferiorly- ethmoidal process of inferior turbinate, anterior, lacrimal bone, posteriorly- hiatus Semilunaris, medial -ethmoid infundibulum, laterally, middle meatus superior attachment- variability, direct effect on frontal sinus drainage pathway.