Urinary Tract Infections Factsheet PDF, 0.17Mb
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Urinary Incontinence: Impact on Long Term Care
Urinary Incontinence: Impact on Long Term Care Muhammad S. Choudhury, MD, FACS Professor and Chairman Department of Urology New York Medical College Director of Urology Westchester Medical Center 1 Urinary Incontinence: Overview • Definition • Scope • Anatomy and Physiology of Micturition • Types • Diagnosis • Management • Impact on Long Term Care 2 Urinary Incontinence: Definition • Involuntary leakage of urine which is personally and socially unacceptable to an individual. • It is a multifactorial syndrome caused by a combination of: • Genito urinary pathology. • Age related changes. • Comorbid conditions that impair normal micturition. • Loss of functional ability to toilet oneself. 3 Urinary Incontinence: Scope • Prevalence of Urinary incontinence increase with age. • Affects more women than men (2:1) up to age 80. • After age 80, both women and men are equally affected. • Urinary Incontinence affect 15% to 30% of the general population > 65 years. • > 50% of 1.5 million Long Term Care residents may be incontinent. • The cost to care for this group is >5 billion per year. • The total cost of care for Urinary Incontinence in the U.S. is estimated to be over $36 billion. Ehtman et al., 2012. 4 Urinary Incontinence: Impact on Quality of Life • Loss of self esteem. • Avoidance of social activity and interaction. • Decreased ability to maintain independent life style. • Increased dependence on care givers. • One of the most common reason for long term care placement. Grindley et al. Age Aging. 1998; 22: 82-89/Harris T. Aging in the eighties. NCHS # 121 1985. Noelker L. Gerontologist 1987; 27: 194-200. 5 Health related consequences of Urinary Incontinence • Increased propensity for fall/fracture. -

CMS Manual System Human Services (DHHS) Pub
Department of Health & CMS Manual System Human Services (DHHS) Pub. 100-07 State Operations Centers for Medicare & Provider Certification Medicaid Services (CMS) Transmittal 8 Date: JUNE 28, 2005 NOTE: Transmittal 7, of the State Operations Manual, Pub. 100-07 dated June 27, 2005, has been rescinded and replaced with Transmittal 8, dated June 28, 2005. The word “wound” was misspelled in the Interpretive Guidance section. All other material in this instruction remains the same. SUBJECT: Revision of Appendix PP – Section 483.25(d) – Urinary Incontinence, Tags F315 and F316 I. SUMMARY OF CHANGES: Current Guidance to Surveyors is entirely replaced by the attached revision. The two tags are being combined as one, which will become F315. Tag F316 will be deleted. The regulatory text for both tags will be combined, followed by this revised guidance. NEW/REVISED MATERIAL - EFFECTIVE DATE*: June 28, 2005 IMPLEMENTATION DATE: June 28, 2005 Disclaimer for manual changes only: The revision date and transmittal number apply to the red italicized material only. Any other material was previously published and remains unchanged. However, if this revision contains a table of contents, you will receive the new/revised information only, and not the entire table of contents. II. CHANGES IN MANUAL INSTRUCTIONS: (N/A if manual not updated.) (R = REVISED, N = NEW, D = DELETED) – (Only One Per Row.) R/N/D CHAPTER/SECTION/SUBSECTION/TITLE R Appendix PP/Tag F315/Guidance to Surveyors – Urinary Incontinence D Appendix PP/Tag F316/Urinary Incontinence III. FUNDING: Medicare contractors shall implement these instructions within their current operating budgets. IV. ATTACHMENTS: Business Requirements x Manual Instruction Confidential Requirements One-Time Notification Recurring Update Notification *Unless otherwise specified, the effective date is the date of service. -

Urinary Tract Infection (Uti) Fact Sheet
URINARY TRACT INFECTION (UTI) FACT SHEET Overview A urinary tract infection (UTI) is an infection that involves any part of the urinary tract, including the kidneys, bladder and urethra. It is usually caused by exposure of the urinary tract to a fecal organism such as Escherichia coli (E. coli) but also may be caused by other organisms. An indwelling urinary catheter is a drainage tube that is inserted into the urinary bladder through the urethra, is left in place and is connected to a closed urine collection system. Urinary tract infections in patients with an indwelling urinary catheter are called catheter-associated UTIs, or CAUTIs. Signs and Symptoms Common symptoms of UTI include: • fever; • pain or burning in the lower abdomen; • burning during urination; • an increase in the frequency of urination; and • cloudy appearing urine. Causes and Transmission A UTI occurs when germs (usually bacteria) enter the urinary tract through the meatus (the opening of the urinary tract). These germs then cause infection. The urinary tract is normally sterile, meaning it contains no germs. A CAUTI occurs when germs (usually bacteria) enter the urinary tract through the urinary catheter and cause infection. This can occur when health care worker hands are not properly cleaned before the insertion of a catheter or during the process of cleaning or emptying of the urine collection system. Risk Factors Sexually active women, people with blockages in the urinary tract, such as prostate enlargement, and women using certain types of birth control, such as diaphragms, or those who are undergoing menopause are at higher risk of UTI. -

Impact of Urolithiasis and Hydronephrosis on Acute Kidney Injury in Patients with Urinary Tract Infection
bioRxiv preprint doi: https://doi.org/10.1101/2020.07.13.200337; this version posted July 13, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Impact of urolithiasis and hydronephrosis on acute kidney injury in patients with urinary tract infection Short title: Impact of urolithiasis and hydronephrosis on AKI in UTI Chih-Yen Hsiao1,2, Tsung-Hsien Chen1, Yi-Chien Lee3,4, Ming-Cheng Wang5,* 1Division of Nephrology, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chia-Yi, Taiwan 2Department of Hospital and Health Care Administration, Chia Nan University of Pharmacy and Science, Tainan, Taiwan 3Department of Internal Medicine, Fu Jen Catholic University Hospital, Fu Jen Catholic University, New Taipei, Taiwan 4School of Medicine, College of Medicine, Fu Jen Catholic University, New Taipei, Taiwan 5Division of Nephrology, Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan *[email protected] 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.07.13.200337; this version posted July 13, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Abstract Background: Urolithiasis is a common cause of urinary tract obstruction and urinary tract infection (UTI). This study aimed to identify whether urolithiasis with or without hydronephrosis has an impact on acute kidney injury (AKI) in patients with UTI. -

233 the Use of Absorbent Pads Increases the Risk For
233 Omli R1, Skotnes L H1, Romild U1, Kuhry E1 1. Namsos Hospital THE USE OF ABSORBENT PADS INCREASES THE RISK FOR LOWER URINARY TRACT INFECTIONS IN NURSING HOMES RESIDENTS. Hypothesis / aims of study Urinary incontinence is a common medical problem in the nursing home population. The aim of this study was to determine whether use of absorbent pads is a risk factor for the development of lower urinary tract infections in nursing home residents. Introduction Lower urinary tract infections (UTIs) are a common medical problem in the elderly. Different kinds of absorbent products, such as diapers, pad and pant combinations, are used in incontinence care. In some cases, indwelling catheters, external condom catheters or in-and-out catheterisation are options for managing bladder dysfunction. About 23% of the residents in nursing homes don’t need toilet assistance. That means that the majority of residents is dependent on help from nursing staff for toileting and help to change soiled absorbent pads. Transmission of bacteria during incontinence care is associated with UTIs in elderly. In the vulnerable nursing home population, UTIs are a frequent problem and can lead to increased morbidity and even mortality. The prevalence of UTIs in nursing home residents is approximately 30%. Improving hand hygiene among staffing in nursing homes is one of the most important and effective methods to reduce hand born transmission of pathological microbes. Studies in long-term-care facilities document a lack of hand hygiene in connection to staff-resident interactions. This study studies the association between the use of absorbent pads and symptomatic UTIs in the nursing home population. -
Module 3: Benign Prostatic Hypertrophy
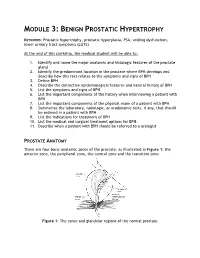
MODULE 3: BENIGN PROSTATIC HYPERTROPHY KEYWORDS: Prostatic hypertrophy, prostatic hyperplasia, PSA, voiding dysfunction, lower urinary tract symptoms (LUTS) At the end of this clerkship, the medical student will be able to: 1. Identify and name the major anatomic and histologic features of the prostate gland 2. Identify the predominant location in the prostate where BPH develops and describe how this fact relates to the symptoms and signs of BPH 3. Define BPH 4. Describe the distinctive epidemiological features and natural history of BPH 5. List the symptoms and signs of BPH 6. List the important components of the history when interviewing a patient with BPH 7. List the important components of the physical exam of a patient with BPH 8. Summarize the laboratory, radiologic, or urodynamic tests, if any, that should be ordered in a patient with BPH 9. List the indications for treatment of BPH 10. List the medical and surgical treatment options for BPH. 11. Describe when a patient with BPH should be referred to a urologist PROSTATE ANATOMY There are four basic anatomic zones of the prostate, as illustrated in Figure 1: the anterior zone, the peripheral zone, the central zone and the transition zone. Figure 1: The zones and glandular regions of the normal prostate. The anterior zone is entirely fibromuscular and non-glandular, and it appears to have little significance in prostatic function or pathology. This area comprises approximately 20% of the bulk of prostatic tissue. The peripheral zone is composed entirely of acinar tissue. It comprises the posterior surface of the prostate, including the apical, lateral, posterolateral and anterolateral portions of the prostate. -

Urinary Incontinence ! ! !What Is Urinary Incontinence? Leakage of Urine Is Called Urinary Incontinence
! ! ! Urinary Incontinence ! ! !What is urinary incontinence? Leakage of urine is called urinary incontinence. Some women leak small amounts of !urine. At other times, leakage of urine is frequent or severe. !Are there different types of urinary incontinence? !There are several types of urinary incontinence: • Stress urinary incontinence is loss of urine when a woman coughs, laughs, or sneezes. Leaks also can happen when a woman walks, runs, or exercises. It is caused by a weakening of the tissues that support the bladder or the muscles of the ! urethra. • Urge incontinence is leakage of urine caused by overactive bladder muscles that ! contract too often or problems with the nerves that send signals to the bladder !• Mixed incontinence is a combination of both stress and urge incontinence symptoms • Overflow incontinence is a steady loss of small amounts of urine when the bladder does not empty all the way during voiding. It can be caused by an underactive bladder ! muscle or blockage of the urethra. !What are the symptoms of urinary incontinence? !In addition to leaking urine, a woman with incontinence also may have other symptoms: • Urgency— A strong urge to urinate whether or not the bladder is full, often with pelvic ! pressure !• Frequency— Voiding more often than she considers usual !• Nocturia — The need to void during hours of sleep !• Dysuria — Painful voiding !• Enuresis— Bed-wetting or leaking while sleeping ! What causes urinary incontinence? ! Urinary incontience can have short-term causes and long-term causes. Short-term !causes are easier to treat and include the following: • Urinary tract infection— Loss of bladder control may be caused by an infection of the urinary tract. -

Gonorrhoea, Chlamydia and Non-Gonococcal Urethritis (Ngu)
MAKING IT COUNT BRIEFING SHEET 4 GONORRHOEA, CHLAMYDIA AND NON-GONOCOCCAL URETHRITIS (NGU) This Making it Count briefing sheet provides an overview on gonorrhoea, chlamydia and non-gonococcal urethritis (NGU) for sexual health promoters working with gay men, bisexual men and other men that have sex with men (MSM). These sexually transmitted infections (STIs) are three of the most common affecting MSM in the UK. They are often grouped together because they have similar modes of transmission, symptoms and treatment. What ARE THEY? • 4,488 gay and bisexual men were diagnosed with In men, gonorrhoea and chlamydia can affect the urethra chlamydia. (the tube in the penis which urine comes out of), the 5,485 gay and bisexual men were diagnosed with NGU. rectum and the throat. NGU only affects the urethra. • Among MSM, chlamydia diagnoses have been rising rapidly Gonorrhoea is caused by infection with the bacteria • over the past decade and the numbers reported as having Neisseria gonorrhoeae. NGU have also increased. There has been a reduction in • Chlamydia is caused by infection with the bacteria gonorrhoea cases in recent years. However, nearly a third of Chlamydia trachomatis. all gonorrhoea diagnoses in men occur in MSM, while approximately one in twelve men infected with chlamydia Non-gonococcal urethritis (NGU) describes • or NGU are MSM. inflammation of the urethra, for which the cause is unknown. How ARE THEY pASSED ON? NGU is usually caused by an unidentified bacteria. In many Gonorrhoea and chlamydia are caused by bacteria which cases if the necessary tests were done, this would turn out may be found in semen, in the urethra and in the rectum of to be Chlamydia trachomatis or Mycoplasma genitalium. -

Nongonococcal Urethritis/NGU Brown Health Services Patient Education Series
Nongonococcal Urethritis/NGU Brown Health Services Patient Education Series What is NGU? How long after exposure do symptoms NGU is an infection of the urethra. The urethra is appear? the tube connecting the bladder to the outside of The incubation period (time between exposure and the body. In people with penises, the urethra also appearance of symptoms) for NGU varies from conveys ejaculate fluid. Urethritis is the medical several days to a few weeks. term for when the urethra gets irritated or inflamed. NGU is considered a sexually transmitted infection (STI). How is it diagnosed? Sexually Transmitted Infections that NGU is usually diagnosed by urine tests for Gonorrhea and Chlamydia. In some cases, your cause NGU: Provider may collect swabs from the penis or ● Chlamydia vagina. Note: a pelvic exam and blood test may also ● Mycoplasma Genitalium be required. ● Trichomoniasis Treatment ● Ureaplasma ● Gonorrhea Treatment usually involves taking antibiotics. If your doctor or nurse thinks you have urethritis, you will If left untreated, organisms causing NGU can cause probably get treatment right away. You do not need serious infections in the testicles and prostate or to wait until your test results come back. the uterus and fallopian tubes. Special Note: What are the symptoms of NGU? Take all of the medication you are given, even if the Most common symptoms include: symptoms start to go away before the medicine is ● pain, burning, or stinging when urinating gone. If you stop taking the medicine, you may ● discharge, often described as “fluid leak” leave some of the infection in your body. from the penis or vagina ● redness or swelling at the tip of the penis If given a seven day course of antibiotics, partners ● occasional rectal pain should abstain from sex for seven days after completion of the antibiotic and until they have no Note: If you have a vagina, these symptoms may be more symptoms. -
Lower Urinary Tract Infection Schiffert Health Center
Schiffert Health Center www.healthcenter.vt.edu Patient Information: Lower Urinary Tract Infection CYSTITIS AND URETHRITIS to SHC for a urinalysis (a urine test). If you are experiencing any of the above symptoms AND The urine you produce in your kidneys is stored in chills and/or fever, you need immediate your urinary bladder until it is excreted. When you treatment. In either case, do not attempt to treat urinate, urine leaves your body by way of your urethra. yourself, and do not take any drugs not This pamp hlet discusses some problems associated with prescribed for your condition. Taking the bladder and urethra. inappropriate medications could affect your What is cystitis? urinalysis and impede your treatment. Cystitis is inflammation of the urinary bladder usually CYSTITIS TREATMENT caused by bacteria. Cystitis is not a sexually transmitted If you have cystitis, your SHC health care provider disease, but sexual intercourse does increase the risk of may prescribe antibiotics to treat your infection and/or a cystitis (bladder infection) in women. medication to relieve your discomfort. Take the antibiotics What is urethritis? exactly as prescribed (see the VT SHC pamphlet titled Using Antibiotics Correctly for more information on Urethritis is inflammation of the urethra. Like cystitis antibiotics). As part of your treatment, you should follow it can be caused by infection. Unlike cystitis, urethritis the instructions for cystitis prevention - especially resulting from infection is often caused by sexually concerning fluid intake and urination! If you experience transmitted organisms and urethritis is a sign of a sexually three or more episodes of cystitis in a six month period, transmitted disease such as chlamydia or gonorrhea. -

UTI and Pyelonephritis Summary
CHI Franciscan Health UTI & Pyelonephritis Summary UTI/pyelonephritis is one of the most common infectious processes but is also often over-treated. Inappropriate treatment rates vary between 17-26%1,2 and up to 52% in patients with indwelling urinary catheters3. Overtreatment can result in unnecessary medication side effects, the development of Clostridium difficile resistance4, colonization with drug-resistant organisms, and undue costs to the health system. Pharmacists can play and important role in optimizing drug therapy to include the recommendation to stop inappropriate antibiotics when their use is not indicated. Asymptomatic bacteriuria (ASB): the presence of bacteria in the urine without signs/symptoms of infection5 o McGeer Criteria often used to define infection, particularly in the long-term care setting6 Clinical (at least one of the following) Lab (at least one of the following) □ Acute dysuria □ Voided specimen: positive urine culture □ Acute pain, swelling, or tenderness of testes, (> 105 CFU/mL), no more than 2 epididymis, or prostate organisms □ Fever or leukocytosis with one of the following: □ Straight cath specimen: positive urine ○ Acute CVA pain or tenderness culture (> 105 CFU/mL), any number of ○ Suprapubic pain organisms ○ Gross hematuria ○ New or marked increase in incontinence ○ New or marked increase in urgency ○ New or marked increase in frequency □ Two of the preceding symptoms in the absence of fever or leukocytosis o ASB should only be treated in pregnant women and patients undergoing invasive urologic procedures5 o People with ASB also often have WBC in the urine (pyuria) but, in the absence of symptoms, this is not indicative of infection o Caused by: colonization of the bladder or contamination of the sample . -

Pyelonephritis (Kidney Infection)
Pyelonephritis (Kidney Infection) Cathy E. Langston, DVM, DACVIM (Small Animal) BASIC INFORMATION urine collected from the bladder to be negative despite infection in the Description kidney. Abdominal x-rays and an ultrasound may be recommended. Bacterial infection of the kidney is termed pyelonephritis . Infection Although culture of a piece of kidney tissue obtained by biopsy may occur within kidney tissue or in the renal pelvis, the area of increases the chance of finding the infection, the invasiveness of the kidney where urine collects before being transported to the the procedure makes it too risky for general use (the biopsy would bladder. need to be taken from deeper within the kidney than the average Causes kidney biopsy). Contrast x-ray studies, such as an excretory uro- In most cases, a urinary tract infection starts in the bladder and gram (intravenous pyelogram), are sometimes helpful. An excre- the bacteria travel upstream to the kidney. Anything that decreases tory urogram involves taking a series of x-rays after a dye (that the free flow of urine, such as obstruction of the urethra (tube shows up white on x-rays) is given intravenously. Other tests may that carries urine from the bladder to the outside), bladder, ureter be recommended to rule out diseases that cause similar clinical (tube that carries urine from the kidney to the bladder), or kid- signs and other causes of kidney disease. ney, increases the risk that the infection will spread to the kid- ney. The presence of stones and growths in the bladder and kidney TREATMENT AND FOLLOW-UP also increases the risk.