LPP-Matching Grant Program Performance and Evaluation Report San Jose Del Monte, Bulacan Philippines
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

SAN JOSE KOOP CONTENTS SAN JOSE DEL MONTE SAVINGS and COOPERATIVE 1 - Chairperson’S Corner
SAN JOSE KOOP CONTENTS SAN JOSE DEL MONTE SAVINGS AND COOPERATIVE 1 - Chairperson’s Corner 2-11 - Regular Activities ● Grand Opening Minuyan Satellite Office ManaGEMENT BoaRD CHAIRPERSON ● 4th Business Forum CHAIR. ROMEO A. DE JESUS ● Cake Decorating Seminar / Feeding Program CHIEF EXECUTIVE OFFICER CEO CAROLINE D. DAVE & Rice Donation for Home for the Elderly LEGAL COUNSEL ● Officers Retreat ATTY. RODELIO B. PUNZALAN ● 2019 Gawad Parangal / 2nd Laboratory Test EDITORIAL BoaRD ● Senior Citizen’s Day EDITOR-IN-CHIEF MS. MARISSA C. PANTALEON ● Multi Cab Donation ASSOCIATE EDITORS ● Sister Society “Rachael Reilling visits” MR. MORRIS DANIEL BRODITH ● Basic Baking Seminar CONTRIBUTOR DIR. JOVITA V. MATEO DIR. JOHN PAUL VILLAR ● ACCESS Renewal MS. NANCY MAGNO MS. MICHELLE CRUZ VILLANUEVA 12-13 - Main Event MS. CAROLINE D. DAVE MR. RUDOLF Z. GADO ● SSS Moa Signing MS. MARY GRACE B. ALE MS. GLENDA M. LORENZO 14 –Skylab Corner MR. EUGENE D. CABUHAT MS. MARY ANN ANGEL DOMINGO MS. RASEL STA. MARIA 15 - Member’s Corner MR. MIA GRACE V. EVANGELISTA 16 - GAD Corner’s EDITORIAL OFFICE 17-24 - For Your Information OFFICE MANAGER ● Financial Highlight as of September 2019 MS. NYRALYN N. DELA TORRE ● Policy Updates GRAPHIC ARTIST MR. MORRIS DANIEL BRODITH ● Featured Products ● San Jose Koop Partners MASIKAP o MAgasing SInasalamin ang KAPatiran ng mga MAmamayang SImbolo ng KAunlaran at Pag-asa is the ● Abuluyan Program 3rd Quarter 2019 official gazette of the San Jose Del Monte Savings and Credit Cooperative published quarterly with the editorial office at ADMIN ● Loyalty Program Office 2nd Floor SJDMSCC Building, San Pedro St. Poblacion 1, City of San Jose del Monte, Bulacan 3023, Philippines. -

Province, City, Municipality Total and Barangay Population AURORA
2010 Census of Population and Housing Aurora Total Population by Province, City, Municipality and Barangay: as of May 1, 2010 Province, City, Municipality Total and Barangay Population AURORA 201,233 BALER (Capital) 36,010 Barangay I (Pob.) 717 Barangay II (Pob.) 374 Barangay III (Pob.) 434 Barangay IV (Pob.) 389 Barangay V (Pob.) 1,662 Buhangin 5,057 Calabuanan 3,221 Obligacion 1,135 Pingit 4,989 Reserva 4,064 Sabang 4,829 Suclayin 5,923 Zabali 3,216 CASIGURAN 23,865 Barangay 1 (Pob.) 799 Barangay 2 (Pob.) 665 Barangay 3 (Pob.) 257 Barangay 4 (Pob.) 302 Barangay 5 (Pob.) 432 Barangay 6 (Pob.) 310 Barangay 7 (Pob.) 278 Barangay 8 (Pob.) 601 Calabgan 496 Calangcuasan 1,099 Calantas 1,799 Culat 630 Dibet 971 Esperanza 458 Lual 1,482 Marikit 609 Tabas 1,007 Tinib 765 National Statistics Office 1 2010 Census of Population and Housing Aurora Total Population by Province, City, Municipality and Barangay: as of May 1, 2010 Province, City, Municipality Total and Barangay Population Bianuan 3,440 Cozo 1,618 Dibacong 2,374 Ditinagyan 587 Esteves 1,786 San Ildefonso 1,100 DILASAG 15,683 Diagyan 2,537 Dicabasan 677 Dilaguidi 1,015 Dimaseset 1,408 Diniog 2,331 Lawang 379 Maligaya (Pob.) 1,801 Manggitahan 1,760 Masagana (Pob.) 1,822 Ura 712 Esperanza 1,241 DINALUNGAN 10,988 Abuleg 1,190 Zone I (Pob.) 1,866 Zone II (Pob.) 1,653 Nipoo (Bulo) 896 Dibaraybay 1,283 Ditawini 686 Mapalad 812 Paleg 971 Simbahan 1,631 DINGALAN 23,554 Aplaya 1,619 Butas Na Bato 813 Cabog (Matawe) 3,090 Caragsacan 2,729 National Statistics Office 2 2010 Census of Population and -

1623400766-2020-Sec17a.Pdf
COVER SHEET 2 0 5 7 3 SEC Registration Number M E T R O P O L I T A N B A N K & T R U S T C O M P A N Y (Company’s Full Name) M e t r o b a n k P l a z a , S e n . G i l P u y a t A v e n u e , U r d a n e t a V i l l a g e , M a k a t i C i t y , M e t r o M a n i l a (Business Address: No. Street City/Town/Province) RENATO K. DE BORJA, JR. 8898-8805 (Contact Person) (Company Telephone Number) 1 2 3 1 1 7 - A 0 4 2 8 Month Day (Form Type) Month Day (Fiscal Year) (Annual Meeting) NONE (Secondary License Type, If Applicable) Corporation Finance Department Dept. Requiring this Doc. Amended Articles Number/Section Total Amount of Borrowings 2,999 as of 12-31-2020 Total No. of Stockholders Domestic Foreign To be accomplished by SEC Personnel concerned File Number LCU Document ID Cashier S T A M P S Remarks: Please use BLACK ink for scanning purposes. 2 SEC Number 20573 File Number______ METROPOLITAN BANK & TRUST COMPANY (Company’s Full Name) Metrobank Plaza, Sen. Gil Puyat Avenue, Urdaneta Village, Makati City, Metro Manila (Company’s Address) 8898-8805 (Telephone Number) December 31 (Fiscal year ending) FORM 17-A (ANNUAL REPORT) (Form Type) (Amendment Designation, if applicable) December 31, 2020 (Period Ended Date) None (Secondary License Type and File Number) 3 SECURITIES AND EXCHANGE COMMISSION SEC FORM 17-A ANNUAL REPORT PURSUANT TO SECTION 17 OF THE SECURITIES REGULATION CODE AND SECTION 141 OF CORPORATION CODE OF THE PHILIPPINES 1. -
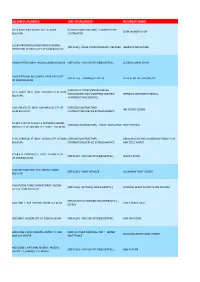
Business Address Line of Business Business Name
BUSINESS ADDRESS LINE OF BUSINESS BUSINESS NAME # 013 BRGY. POBLACION I CITY OF SJDM [SERVICES/CONTRACTORS] - LAUNDRY SHOP SJDM LAUNDRY SHOP BULACAN CONTRACTOR # 166A PROVINCIAL ROAD FARMVIEW BRGY. [RETAILER] - DRUG STORE/PHARMACY RETAILER GENERIKA DRUGSTORE TUNGKONG MANGGA CITY OF SJDM BULACAN # 1824 PARTIDA BRGY MUZON CSJDM BULACAN [RETAILER] - SARI-SARI STORE(ESSENTIAL) CLAIRE & AIRISH STORE # 260 NATIONAL ROAD BRGY. GAYA GAYA CITY [RETAILER] - TRADING (RETAILER) FIL-BEST METAL TRADING INC. OF SJDM BULACAN [LESSORS OF APARTMENT\BOARDING # 277 CARRIEDO ST. BRGY. MUZON CITY OF SJDM HSE\LODGING\INNS \SHOPPING CENTERS] - LERMENG APARTMENT RENTAL BULACAN APARTMENT (RESIDENTIAL) # 28 CORINTH ST. BRGY. SAN MANUEL CITY OF [SERVICES/CONTRACTORS] - INK STUDIO DESIGN SJDM BULACAN CONTRACTORS/SERVICE ESTABLISHMENTS # 3 BLK 1 LOT 34 PHASE F-1 FRANCISCO HOMES [SERVICES/CONTRACTORS] - PHOTO DEVELOPING PRINT STATION NARRA CITY OF SAN JOSE DEL MONTE BULACAN # 332 CARRIEDO ST. BRGY. MUZON CITY OF SJDM [SERVICES/CONTRACTORS] - GENDOR GLASS AND ALUMINUM FABRICATION BULACAN CONTRACTORS/SERVICE ESTABLISHMENTS AND STEEL WORKS # 358 STO. DOMINGO ST. BRGY. FATIMA I CITY [RETAILER] - SARI-SARI STORE(ESSENTIAL) CESAR`S STORE OF SJDM BULACAN # 40 IGAY ROAD BGY. STO. CRISTO, CSJDM [RETAILER] - PAINT RETAILER GJ LAGMAN PAINT CENTER BULACAN # 56 MUZON PUBLIC MARKET BRGY. MUZON [RETAILER] - RETAILER [ NON-ESSENTIAL ] CORAZON DEROY PLASTIC WARE TRADING CITY OF SJDM BULACAN [RESTAURANT\CARINDERIAS\EATERIES\ETC.] - # 64 ZONE 1, BGY. MUZON, CSJDM, BULACAN TINS`S SNACK HAUZ EATERY #001 BRGY. MUZON CITY OF SJDM BULACAN [RETAILER] - SARI-SARI STORE(ESSENTIAL) SARI SARI STORE #001 ZONE 1 BRGY, MUZON, DISTRICT 1, SAN [BANK & OTHER FINANCIAL INST.] - MONEY BOAQUIÑA REMITTANCE CENTER JOSE DEL MONTE REMITTANCE #001 ZONE 1 NATIONAL RD BRGY, MUZON, [RETAILER] - SARI-SARI STORE(ESSENTIAL) MBS-R STORE DISTRICT 1, SAN JOSE DEL MONTE #005 B1 L5 ST. -

[Ff-T,^; Region Lll-Central Luzon D.M
Republic of the Philippines DEPARTMENT OF EDUCA [ff-T,^; Region lll-Central Luzon D.M. Government Center, Maimpis, City of San Email: [email protected] Tel: (045) 45$.2309 X Fa(: (045)45$2312 April3,2A17 REGIONAT MEMORANDUM ruo.-jf series 2017 CLRAA PARTICIPATION TO THE 2017 PALARONG PAMBANSA To: All Schools Division Superintendents Heads, Public and Private Elementary and Secondary School AllOthers Concern 1. DepEd Regional Office lll announces the participation of Central Luzon Regional Athletic Association (CLRAA) to the 2017 Palarong Pambansa which shall be held at Binirayan Sports Comple& San Jose, Antique on April 23-29, 2037. The delegation shalt participate in all regular sports events. The objectives of the Palarong Pambansa are: a. to promote physical education and sports as an integral part on the Basic Education for holistic development of the youth to become responsible and globally competitive citizens of the country; b. to inculcate the spirit of discipline, teamwork, excellence, fair play, solidarity, sportsmanship, and other values inherent in sports; c. to promote and achieve peace by means of sports; d. to widen the base for talent identification, selection, recruitment, training and exposure of elementary pupils and secondary students to serve as athletes' rooster to the National Sports Associations for international competitions and; e. to provide database that will serve as basis for further improve the school sports development programs. 3. The delegation is composed of Delegation Officials and Working Staff (Enclosure No.1). The designated Team Managers shall oversee a specific team. He/She shall monitor and supervise the team, attend meetings and eventually relay information to the coaches. -

Cities #Withrefugees Statement
Please consider signing the Cities #WithRefugees solidarity statement. Launched in advance of World Refugee Day (June 20) in 2018, the Cities #WithRefugees initiative has brought together more than 125 cities in 41 countries in a call for more local authorities and municipalities to join them in welcoming and including refugees in their communities. Cities can continue to sign onto the document here to send a strong message of global grass roots solidarity for families forced to flee. Cities #WithRefugees Statement We, mayors and local authorities from around the world, stand #WithRefugees. The role of towns, cities, counties and provinces in creating inclusive communities and promoting hope has never been as important. Today, over 25 million people worldwide are living outside their countries to escape violence and persecution. Refugees leave nearly everything behind to seek safety: their homes, their jobs, and sometimes even their families. Despite the unimaginable sacrifices refugees make to find safety, many keep their hopes and dreams for the future. Refugees’ will to survive and their drive to help their families and communities prosper are not easily extinguished by adversity. When refugees arrive to a new country, nearly two out of three settle in an urban area. As cities, we are undeniably at the forefront of refugee crises, and our communities benefit from their tenacity and courage. Welcoming refugees creates opportunities for economic, civic and social growth. The diversity of experiences and ideas refugees bring spurs creativity and innovation. For example, both Albert Einstein and Sergey Brin were refugees. Their contributions did not just change our communities; they changed the course of human history. -

(Region Iii & R Mega Manila Subway Project
JAPAN INTERNATIONAL COOPERATION AGENCY (JICA) NATIONAL ECONOMIC DEVELOPMENT AUTHORITY (NEDA) ROADMAP FOR TRANSPORT INFRASTRUCTURE DEVELOPMENT FOR METRO MANILA AND ITS SURROUNDING AREAS (REGION III & REGION IV-A) FINAL REPORT SUPPLEMENTAL REPORT NO. 2 MEGA MANILA SUBWAY PROJECT March 2014 ALMEC CORPORATION The rate used in the report is USD1.0= Php 40 TABLE OF CONTENTS 1. INTRODUCTION ............................................................................................................. 1 2. PROJECT CONCEPT ..................................................................................................... 2 2.1 Overall Urban Rail Network ................................................................................................2 2.2 Expected Role of the Project ..............................................................................................7 3. Preliminary Demand Forecast .................................................................................... 10 3.1 Methodology .....................................................................................................................10 3.2 Estimated Ridership ..........................................................................................................17 4. PRELIMINARY SYSTEM DESIGN ................................................................................ 25 4.1 Routes and Alignments .....................................................................................................25 4.2 Related Subsystems and Facilities...................................................................................30 -
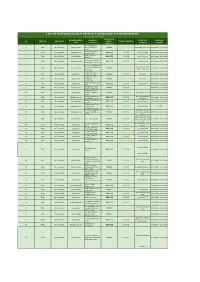
List of Licensed Covid-19 Testing Laboratory in the Philippines
LIST OF LICENSED COVID-19 TESTING LABORATORY IN THE PHILIPPINES ( as of November 26, 2020) OWNERSHIP MUNICIPALITY / NAME OF CONTACT LICENSE REGION PROVINCE (PUBLIC / TYPE OF TESTING # CITY FACILITY NUMBER VALIDITY PRIVATE) Amang Rodriguez 1 NCR Metro Manila Marikina City Memorial Medical PUBLIC Cartridge - Based PCR 8948-0595 / 8941-0342 07/18/2020 - 12/31/2020 Center Asian Hospital and 2 NCR Metro Manila Muntilupa City PRIVATE rRT PCR (02) 8771-9000 05/11/2020 - 12/31/2020 Medical Center Chinese General 3 NCR Metro Manila City of Manila PRIVATE rRT PCR (02) 8711-4141 04/15/2020 - 12/31/2020 Hospital Detoxicare Molecular 4 NCR Metro Manila Mandaluyong City PRIVATE rRT PCR (02) 8256-4681 04/11/2020 - 12/31/2020 Diagnostics Laboratory Dr. Jose N. Rodriguez Memorial Hospital and (02) 8294-2571; 8294- 5 NCR Metro Manila Caloocan City PUBLIC Cartridge - Based PCR 08/13/2020 - 12/31/2020 Sanitarium 2572 ; 8294-2573 (GeneXpert)) Lung Center of the 6 NCR Metro Manila Quezon City PUBLIC rRT PCR 8924-6101 03/27/2020 - 12/31/2020 Philippines (LCP) Lung Center of the 7 NCR Metro Manila Quezon City Philippines PUBLIC Cartridge - Based PCR 8924-6101 05/06/2020 - 12/31/2020 (GeneXpert) Makati Medical Center 8 NCR Metro Manila Makati City PRIVATE rRT PCR (02) 8888-8999 04/11/2020 - 12/31/2020 (HB) Marikina Molecular 9 NCR Metro Manila Marikina City PUBLIC rRT PCR 04/30/2020 - 12/31/2020 Diagnostic laboratory Philippine Genome 10 NCR Metro Manila Quezon City Center UP-Diliman PUBLIC rRT PCR 8981-8500 Loc 4713 04/23/2020 - 12/31/2020 (NHB) Philippine Red Cross - (02) 8790-2300 local 11 NCR Metro Manila Mandaluyong City PRIVATE rRT PCR 04/23/2020 - 12/31/2020 National Blood Center 931/932/935 Philippine Red Cross - 12 NCR Metro Manila City of Manila PRIVATE rRT PCR (02) 8527-0861 04/14/2020 - 12/31/2020 Port Area Philippine Red Cross 13 NCR Metro Manila Mandaluyong City Logistics and PRIVATE rRT PCR (02) 8790-2300 31/12/2020 Multipurpose Center Research Institute for (02) 8807-2631; (02) 14 NCR Metro Manila Muntinlupa City Tropical Medicine, Inc. -

Philippine Drug Enforcement Agency Regional Office Iii
Republic of the Philippines OFFICE OF THE PRESIDENT PHILIPPINE DRUG ENFORCEMENT AGENCY REGIONAL OFFICE III DiosdadoMacapagal Regional Government Center Brgy. Maimpis, San Fernando City, Pampanga Telefax-(045) 649-1008; Telephone (045) 649-1009; email [email protected] REGIONAL OFFICE PROFILE BRIEFER ON PDEA REGIONAL OFFICE III The PDEA Regional Office III, or PDEA RO III, is among the Agency’s 18 regional office nationwide, which has primary operational control, supervision and jurisdiction in Central Luzon. After the enactment of Republic Act No. 9165 in July 2002, the PDEA RO III office was housed at the PNP Annex Building in No. 7372, Clark Special Economic Zone, Clarkfield, Pampanga. In October 2003, the Region forged a Memorandum of Agreement (MOA) with the PNP PRO 3 to relocate the PDEA RO III in the office space formerly occupied by the defunct PNP PRO 3 Narcotics Group at Camp Captain Julian Olivas in the City of San Fernando, Pampanga. Since then, the PDEA RO3 office is located in Camp Olivas, City of San Fernando, Pampanga. In 2008, plantilla positions were created for PDEA, in which 11 organic personnel holding different positions reported at PDEA RO III. Drug Enforcement Officers (DEOs) were also assigned in this Regional Office to cater to the demands of anti-drug problem. In 2009, the PDEA RO III initiated the request for NEDA RO 3 to assign an office lot for the Office at the Regional Government Center in Barangay Maimpis, City of San Fernando, Pampanga. In 2013, the Office constructed the PDEA RO III Regional Forensic Laboratory. In February 2014, the PDEA RO III was assigned with a 500 sq.m. -

46362-004: Angat Water Transmission Improvement Project
Resettlement Plan Project Number: 46362-004 February 2019 PHI: Angat Water Transmission Improvement Project Additional Financing This draft resettlement plan is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. CURRENCY EQUIVALENTS (as of March 2018) Currency unit – peso/s (₱) ₱1.00 = $0.01916 $1.00 = ₱52 ABBREVIATIONS ADB – Asian Development Bank AHs – Affected Households APs – Affected Persons AWTIP – Angat Water Tunnel Improvement Project BNAQ7P – Bigte-Novaliches Aqueduct 7 Project CMP – Community Mortgage Program CWA – Contractor’s Work Area DDR – Due Diligence Report DPWH – Department of Public Works and Highways EA – Executing Agency EO – Executive Order GRC – Grievance Redress Committee GRM – Grievance Redress Mechanism HHs – Household heads IA – Implementing Agency IP – Indigenous Peoples IR – Involuntary Resettlement IRR – Implementing Rules and Regulations ISF – Informal Settler Families LARRIPP – Land acquisition, Resettlement, Rehabilitation and Indigenous Peoples Policy (DPWH, 2007) LIAC – Local Inter-Agency Committee LGU – Local Government Unit MO – Memorandum Orders MWSS – Metropolitan Waterworks and Sewerage -

LOCAL GOVERNMENT RECORDS and PRACTICES Iyra S
JOURNAL OF PHILIPPINE LIBRARIANSHIP PRESERVING THE POSTWAR ARCHIVES HERITAGE AND COLLECTIVE MEMORY OF BULACAN: LOCAL GOVERNMENT RECORDS AND PRACTICES Iyra S. Buenrostro Abstract Presents the condition of the local government records and archives of the local governments of Malolos, Meycauayan and San Jose Del Monde in Bulacan. Discusses the approaches of these local governments in controlling local goventment records using the records continuum concept. Alongside the evolution of physical carriers and media in which information is recorded, is the development of thought as regards the theory and practice of Archival Science. Archival Science is seen as a discipline that originated from and is closely related to the field of historical sciences, in which documents are treated as traces of the past and are supposedly preserved and appreciated as part of society’s heritage (Cardin, 2000). Thus, it is clear that archives play a vital role in building collective memory and identity both in the micro and macro level of society; and this “memory” should be accessible and be transmitted to future generations. Theories and principles central to archival practices, as well as the standards set for the preservation of archives heritage have been laid for the archivists worldwide to follow and guarantee that there are enough and properly preserved representative records. Numerous texts on archival practices have been published by different archives theorists and archives organizations, including the collaborative efforts of the International Council on Archives (ICA) and United Nations Educational, Scientific and Cultural Organization (UNESCO). The UNESCO has launched the Memory of the World Programme that aims to preserve and disseminate the archives and library holdings worldwide. -

Meycauayan-Marilao-Obando River System WQMA (Based on NWRB Recommendation) 2
DENR DESIGNATIONDESIGNATION OFOF WATERWATER QUALITYQUALITY MANAGEMENTMANAGEMENT AREASAREAS ININ THETHE PHILIPPINESPHILIPPINES Ms. Leza A. Acorda-Cuevas Republic of the Philippines DefinitionDefinition WQMAWQMA AnAn areaarea coveringcovering thethe samesame physiographicphysiographic unitunit whichwhich affectsaffects thethe physicophysico--chemicalchemical andand biologicalbiological reactionsreactions andand diffusiondiffusion ofof pollutantspollutants inin thethe bodiesbodies ofof waterwater drainingdraining thethe saidsaid area.area. NAANAA BodiesBodies ofof waterwater wherewhere specificspecific pollutantspollutants havehave alreadyalready exceededexceeded waterwater qualityquality guidelinesguidelines andand thereforetherefore inin needneed ofof rehabilitation.rehabilitation. TheThe PhilippinePhilippine CleanClean WaterWater ActAct 20042004 (Republic Act No. 9275) 1 2 3 4 AIMS TO IMPROVE WATER QUALITY THROUGH FOCUSED INTERVENTIONS OR ACTIONS TO ADDRESS WQ PROBLEM(S) OF THE AREA WATERWATER QUALITYQUALITY MANAGEMENTMANAGEMENT SYSTEMSYSTEM PREPARATION AND IMPLEMENTATION OF WQMA ACTION PLANS DESIGNATION OF IDENTIFICATION WQMAs OF NAAs ObjectivesObjectives ofof DesignatingDesignating WQMAWQMA WQMAWQMA isis aa significantsignificant tooltool inin enforcingenforcing thethe CWA.CWA. AimsAims forfor thethe improvementimprovement ofof waterwater qualityquality toto meetmeet thethe guidelinesguidelines (DAO(DAO 34,34, ss 1990)1990) underunder whichwhich theythey havehave beenbeen classifiedclassified oror toto improveimprove theirtheir classificationclassification