Patient Transport Via Commercial Airlines
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
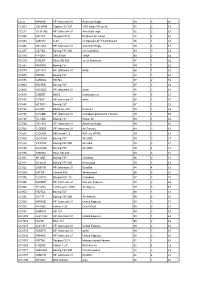
CC22 N848AE HP Jetstream 31 American Eagle 89 5 £1 CC203 OK
CC22 N848AE HP Jetstream 31 American Eagle 89 5 £1 CC203 OK-HFM Tupolev Tu-134 CSA -large OK on fin 91 2 £3 CC211 G-31-962 HP Jetstream 31 American eagle 92 2 £1 CC368 N4213X Douglas DC-6 Northern Air Cargo 88 4 £2 CC373 G-BFPV C-47 ex Spanish AF T3-45/744-45 78 1 £4 CC446 G31-862 HP Jetstream 31 American Eagle 89 3 £1 CC487 CS-TKC Boeing 737-300 Air Columbus 93 3 £2 CC489 PT-OKF DHC8/300 TABA 93 2 £2 CC510 G-BLRT Short SD-360 ex Air Business 87 1 £2 CC567 N400RG Boeing 727 89 1 £2 CC573 G31-813 HP Jetstream 31 white 88 1 £1 CC574 N5073L Boeing 727 84 1 £2 CC595 G-BEKG HS 748 87 2 £2 CC603 N727KS Boeing 727 87 1 £2 CC608 N331QQ HP Jetstream 31 white 88 2 £1 CC610 D-BERT DHC8 Contactair c/s 88 5 £1 CC636 C-FBIP HP Jetstream 31 white 88 3 £1 CC650 HZ-DG1 Boeing 727 87 1 £2 CC732 D-CDIC SAAB SF-340 Delta Air 89 1 £2 CC735 C-FAMK HP Jetstream 31 Canadian partner/Air Toronto 89 1 £2 CC738 TC-VAB Boeing 737 Sultan Air 93 1 £2 CC760 G31-841 HP Jetstream 31 American Eagle 89 3 £1 CC762 C-GDBR HP Jetstream 31 Air Toronto 89 3 £1 CC821 G-DVON DH Devon C.2 RAF c/s VP955 89 1 £1 CC824 G-OOOH Boeing 757 Air 2000 89 3 £1 CC826 VT-EPW Boeing 747-300 Air India 89 3 £1 CC834 G-OOOA Boeing 757 Air 2000 89 4 £1 CC876 G-BHHU Short SD-330 89 3 £1 CC901 9H-ABE Boeing 737 Air Malta 88 2 £1 CC911 EC-ECR Boeing 737-300 Air Europa 89 3 £1 CC922 G-BKTN HP Jetstream 31 Euroflite 84 4 £1 CC924 I-ATSA Cessna 650 Aerotaxisud 89 3 £1 CC936 C-GCPG Douglas DC-10 Canadian 87 3 £1 CC940 G-BSMY HP Jetstream 31 Pan Am Express 90 2 £2 CC945 7T-VHG Lockheed C-130H Air Algerie -
Netletter #1379 | November 29, 2017
NetLetter #1379 | November 29, 2017 Vickers Viscount CF-THS Dear Reader, Welcome to the NetLetter, an Aviation based newsletter for Air Canada, TCA, CP Air, Canadian Airlines and all other Canadian based airlines that once graced the Canadian skies. The NetLetter is published on the second and fourth weekend of each month. If you are interested in Canadian Aviation History, and vintage aviation photos, especially as it relates to Trans-Canada Air Lines, Air Canada, Canadian Airlines International and their constituent airlines, then we're sure you'll enjoy this newsletter. Our website is located at www.thenetletter.net Please click the links below to visit our NetLetter Archives and for more info about the NetLetter. Women in Aviation Valentina Tereshkova, the Soviet cosmonaut, became the first woman in space in 1963. More info at Wikipedia. Air Canada News Controllers ignore Mayday calls. Canadian officials say they’ll talk to their counterparts in India after air traffic controllers reportedly ignored a series of Mayday calls from an Air Canada Boeing 787 and ordered the crew to enter holds instead. The Dreamliner had finished a 16-hour flight from Toronto to Mumbai on Sept. 18 but a runway overrun by a SpiceJet Boeing 737 closed the active runway. Rather than going to its alternate, the aircraft was put in a series of holds by Mumbai controllers. After an hour of turning left, the Air Canada plane was getting low on fuel so the crew asked for clearance to its alternate. They were told the unidentified alternate airport was unavailable because it was at capacity and unable to take any more traffic. -

Unsolved Rapes Raise Safety Fears
Cats missing Get tested 'Bali begins A number of cats have Local residents are urged to get More than 40 youth from Terrace, mysteriously disappeared from the their blood tested for the hepatitis Smithers and Kitimat turned out Horseshoe area\NEWS A3 C virus\COMMUNITY B1 for a fastball clinic\SPORTS B6 WEDNESDAY $1.00 PLUS 7¢ GST (S1.10 plus 8¢ GST outside of the April 12, 2000 Terrace area) T . NDARD VOL. 13 NO. 1 Unsolved rapes raise safety fears By CHRISTIANA WIENS of Kalum Street, happened around 8 RCMP say her attackers are be- Udsen said regional investigators not normally hear about." TERRACE RCMP are question- a.m., Wednesday, March 22. tween 18 and 23 years old. One of the based in Prince Rupert, in town last Of particular concern, she said, is ing a number of suspects after two The suspect - believed to be a na- men is believed to be native, while Tuesday to help Terrace's drug section the March 31 attack on Davis Street. the other's ethnicity isn't known. execute two warrants, were tied up "Two (attackers) is not a random extremely violent sexual attacks tive male wearing a blue bandana to mask his face - is described as having Udsen said the attacks do not ap- and unable to help this case. act," she said. "They have to discuss on women in the past three weeks. a thin to medium build. pear to be related to earlier stalking Meanwhile, he said, local women and they have to debrief." But as of Apr. -
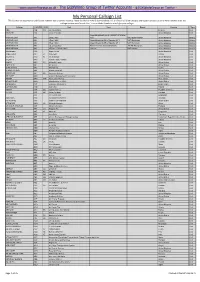
My Personal Callsign List This List Was Not Designed for Publication However Due to Several Requests I Have Decided to Make It Downloadable
- www.egxwinfogroup.co.uk - The EGXWinfo Group of Twitter Accounts - @EGXWinfoGroup on Twitter - My Personal Callsign List This list was not designed for publication however due to several requests I have decided to make it downloadable. It is a mixture of listed callsigns and logged callsigns so some have numbers after the callsign as they were heard. Use CTL+F in Adobe Reader to search for your callsign Callsign ICAO/PRI IATA Unit Type Based Country Type ABG AAB W9 Abelag Aviation Belgium Civil ARMYAIR AAC Army Air Corps United Kingdom Civil AgustaWestland Lynx AH.9A/AW159 Wildcat ARMYAIR 200# AAC 2Regt | AAC AH.1 AAC Middle Wallop United Kingdom Military ARMYAIR 300# AAC 3Regt | AAC AgustaWestland AH-64 Apache AH.1 RAF Wattisham United Kingdom Military ARMYAIR 400# AAC 4Regt | AAC AgustaWestland AH-64 Apache AH.1 RAF Wattisham United Kingdom Military ARMYAIR 500# AAC 5Regt AAC/RAF Britten-Norman Islander/Defender JHCFS Aldergrove United Kingdom Military ARMYAIR 600# AAC 657Sqn | JSFAW | AAC Various RAF Odiham United Kingdom Military Ambassador AAD Mann Air Ltd United Kingdom Civil AIGLE AZUR AAF ZI Aigle Azur France Civil ATLANTIC AAG KI Air Atlantique United Kingdom Civil ATLANTIC AAG Atlantic Flight Training United Kingdom Civil ALOHA AAH KH Aloha Air Cargo United States Civil BOREALIS AAI Air Aurora United States Civil ALFA SUDAN AAJ Alfa Airlines Sudan Civil ALASKA ISLAND AAK Alaska Island Air United States Civil AMERICAN AAL AA American Airlines United States Civil AM CORP AAM Aviation Management Corporation United States Civil -
Appendix 25 Box 31/3 Airline Codes
March 2021 APPENDIX 25 BOX 31/3 AIRLINE CODES The information in this document is provided as a guide only and is not professional advice, including legal advice. It should not be assumed that the guidance is comprehensive or that it provides a definitive answer in every case. Appendix 25 - SAD Box 31/3 Airline Codes March 2021 Airline code Code description 000 ANTONOV DESIGN BUREAU 001 AMERICAN AIRLINES 005 CONTINENTAL AIRLINES 006 DELTA AIR LINES 012 NORTHWEST AIRLINES 014 AIR CANADA 015 TRANS WORLD AIRLINES 016 UNITED AIRLINES 018 CANADIAN AIRLINES INT 020 LUFTHANSA 023 FEDERAL EXPRESS CORP. (CARGO) 027 ALASKA AIRLINES 029 LINEAS AER DEL CARIBE (CARGO) 034 MILLON AIR (CARGO) 037 USAIR 042 VARIG BRAZILIAN AIRLINES 043 DRAGONAIR 044 AEROLINEAS ARGENTINAS 045 LAN-CHILE 046 LAV LINEA AERO VENEZOLANA 047 TAP AIR PORTUGAL 048 CYPRUS AIRWAYS 049 CRUZEIRO DO SUL 050 OLYMPIC AIRWAYS 051 LLOYD AEREO BOLIVIANO 053 AER LINGUS 055 ALITALIA 056 CYPRUS TURKISH AIRLINES 057 AIR FRANCE 058 INDIAN AIRLINES 060 FLIGHT WEST AIRLINES 061 AIR SEYCHELLES 062 DAN-AIR SERVICES 063 AIR CALEDONIE INTERNATIONAL 064 CSA CZECHOSLOVAK AIRLINES 065 SAUDI ARABIAN 066 NORONTAIR 067 AIR MOOREA 068 LAM-LINHAS AEREAS MOCAMBIQUE Page 2 of 19 Appendix 25 - SAD Box 31/3 Airline Codes March 2021 Airline code Code description 069 LAPA 070 SYRIAN ARAB AIRLINES 071 ETHIOPIAN AIRLINES 072 GULF AIR 073 IRAQI AIRWAYS 074 KLM ROYAL DUTCH AIRLINES 075 IBERIA 076 MIDDLE EAST AIRLINES 077 EGYPTAIR 078 AERO CALIFORNIA 079 PHILIPPINE AIRLINES 080 LOT POLISH AIRLINES 081 QANTAS AIRWAYS -

Air Passenger Origin and Destination, Canada-United States Report
Catalogue no. 51-205-XIE Air Passenger Origin and Destination, Canada-United States Report 2005 How to obtain more information Specific inquiries about this product and related statistics or services should be directed to: Aviation Statistics Centre, Transportation Division, Statistics Canada, Ottawa, Ontario, K1A 0T6 (Telephone: 1-613-951-0068; Internet: [email protected]). For information on the wide range of data available from Statistics Canada, you can contact us by calling one of our toll-free numbers. You can also contact us by e-mail or by visiting our website at www.statcan.ca. National inquiries line 1-800-263-1136 National telecommunications device for the hearing impaired 1-800-363-7629 Depository Services Program inquiries 1-800-700-1033 Fax line for Depository Services Program 1-800-889-9734 E-mail inquiries [email protected] Website www.statcan.ca Information to access the product This product, catalogue no. 51-205-XIE, is available for free in electronic format. To obtain a single issue, visit our website at www.statcan.ca and select Publications. Standards of service to the public Statistics Canada is committed to serving its clients in a prompt, reliable and courteous manner. To this end, the Agency has developed standards of service which its employees observe in serving its clients. To obtain a copy of these service standards, please contact Statistics Canada toll free at 1-800-263-1136. The service standards are also published on www.statcan.ca under About us > Providing services to Canadians. Statistics Canada Transportation Division Aviation Statistics Centre Air Passenger Origin and Destination, Canada-United States Report 2005 Published by authority of the Minister responsible for Statistics Canada © Minister of Industry, 2007 All rights reserved. -

Bombardier Business Aircraft and Are Not Added to This Report
BACKGROUNDER June 30, 2015 Program Status Report - CRJ Series aircraft Deliveries Total Total Current Apr - Jun FYTD 1 Orders Delivered Backlog 2015 CRJ100 226 226 0 0 0 CRJ200 709 709 0 0 0 CRJ440 86 86 0 0 0 CRJ700 Series 701 2 334 326 8 1 2 CRJ700 Series 705 16 16 0 0 0 CRJ900 391 351 40 11 24 CRJ1000 68 40 28 0 1 Challenger 800 3 33 33 0 0 0 Total 1863 1787 76 12 27 June 30, 2015 Page 1 of 3 Program Status Report - CRJ Series aircraft CRJ700 CRJ700 CRJ700 CRJ700 Customer Total Total CRJ100 CRJ100 CRJ200 CRJ200 CRJ440 CRJ440 Series 701 Series 701 Series 705 Series 705 CRJ900 CRJ900 CRJ1000 CRJ1000 Orders Delivered Backlog Ordered Delivered Ordered Delivered Ordered Delivered Ordered Delivered Ordered Delivered Ordered Delivered Ordered Delivered Adria Airways 12 11 1 0 0 5 5 0 0 0 0 0 0 7 6 0 0 AeroLineas MesoAmericanas 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 Air Canada 56 56 0 24 24 17 17 0 0 0 0 15 15 0 0 0 0 Air Dolimiti 5 5 0 0 0 5 5 0 0 0 0 0 0 0 0 0 0 Air Littoral 19 19 0 19 19 0 0 0 0 0 0 0 0 0 0 0 0 Air Nostrum 81 56 25 0 0 35 35 0 0 0 0 0 0 11 11 35 10 Air One 10 10 0 0 0 0 0 0 0 0 0 0 0 10 10 0 0 Air Wisconsin 64 64 0 0 0 64 64 0 0 0 0 0 0 0 0 0 0 American Airlines 54 30 24 0 0 0 0 0 0 0 0 0 0 54 30 0 0 American Eagle 47 47 0 0 0 0 0 0 0 47 47 0 0 0 0 0 0 Arik Air 7 5 2 0 0 0 0 0 0 0 0 0 0 4 4 3 1 Atlantic Southeast (ASA) 57 57 0 0 0 45 45 0 0 12 12 0 0 0 0 0 0 Atlasjet 3 3 0 0 0 0 0 0 0 0 0 0 0 3 3 0 0 Austrian arrows 4 13 13 0 0 0 13 13 0 0 0 0 0 0 0 0 0 0 BRIT AIR 49 49 0 20 20 0 0 0 0 15 15 0 0 0 0 14 14 British European 4 4 0 0 0 4 4 0 0 0 0 0 0 0 0 0 0 China Eastern Yunnan 6 6 0 0 0 6 6 0 0 0 0 0 0 0 0 0 0 China Express 28 18 10 0 0 0 0 0 0 0 0 0 0 28 18 0 0 Cimber Air 2 2 0 0 0 2 2 0 0 0 0 0 0 0 0 0 0 COMAIR 130 130 0 110 110 0 0 0 0 20 20 0 0 0 0 0 0 DAC AIR 2 2 0 0 0 2 2 0 0 0 0 0 0 0 0 0 0 Delta Connection 168 168 0 0 0 94 94 0 0 30 30 0 0 44 44 0 0 Delta Air Lines 40 40 0 0 0 0 0 0 0 0 0 0 0 40 40 0 0 Estonian Air 3 3 0 0 0 0 0 0 0 0 0 0 0 3 3 0 0 The Fair Inc. -
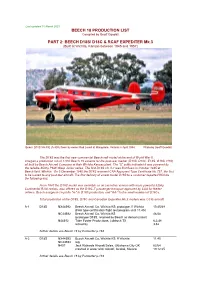
BEECH D18S/ D18C & RCAF EXPEDITER Mk.3 (Built at Wichita, Kansas Between 1945 and 1957)
Last updated 10 March 2021 BEECH 18 PRODUCTION LIST Compiled by Geoff Goodall PART 2: BEECH D18S/ D18C & RCAF EXPEDITER Mk.3 (Built at Wichita, Kansas between 1945 and 1957) Beech D18S VH-FIE (A-808) flown by owner Rod Lovell at Mangalore, Victoria in April 1984. Photo by Geoff Goodall The D18S was the first new commercial Beechcraft model at the end of World War II. It began a production run of 1,800 Beech 18 variants for the post-war market (D18S, D18C, E18S, G18S, H18), all built by Beech Aircraft Company at their Wichita Kansas plant. The “S” suffix indicated it was powered by the reliable 450hp P&W Wasp Junior series. The first D18S c/n A-1 was first flown in October 1945 at Beech field, Wichita. On 5 December 1945 the D18S received CAA Approved Type Certificate No.757, the first to be issued to any post-war aircraft. The first delivery of a new model D18S to a customer departed Wichita the following day. From 1947 the D18C model was available as an executive version with more powerful 525hp Continental R-9A radials, also offered as the D18C-T passenger transport approved by CAA for feeder airlines. Beech assigned c/n prefix "A-" to D18S production, and "AA-" to the small number of D18Cs. Total production of the D18S, D18C and Canadian Expediter Mk.3 models was 1,035 aircraft. A-1 D18S NX44592 Beech Aircraft Co, Wichita KS: prototype, ff Wichita 10.45/48 (FAA type certification flight test program until 11.45) NC44592 Beech Aircraft Co, Wichita KS 46/48 (prototype D18S, retained by Beech as demonstrator) N44592 Tobe Foster Productions, Lubbock TX 6.2.48 retired by 3.52 further details see Beech 18 by Parmerter p.184 A-2 D18S NX44593 Beech Aircraft Co, Wichita KS: ff Wichita 11.45 NC44593 reg. -

Crash Survivability and the Emergency Brace Position
航空宇宙政策․法學會誌 第 33 卷 第 2 號 논문접수일 2018. 11. 30 2018년 12월 30일 발행, pp. 199~224 논문심사일 2018. 12. 14 http://dx.doi.org/10.31691/KASL33.2.6. 게재확정일 2018. 12. 30 Regulatory Aspects of Passenger and Crew Safety: Crash Survivability and the Emergency Brace Position Jan M. Davies* 46) CONTENTS Ⅰ. Introduction Ⅱ. Passenger and Crew Crash Survivability and the Emergency Brace Position Ⅲ. Regulations, and their Gaps, Relating to the Emergency Brace Position Ⅳ. Conclusions * Professor Jan M Davies MSc MD FRCPC FRAeS is a Professor of Anesthesiology, Perioperative and Pain Medicine in the Cumming School of Medicine and an Adjunct Professor of Psychology in the Faculty of Arts, University of Calgary. She is the chair of IBRACE, the International Board for Research into Aircraft Crash Events. (https://en. wikipedia.org/wiki/International_Board_for_Research_into_Aircraft_Crash_Events) Amongst other publications, she is the co-author, with Linda Campbell, of An Investigation into Serial Deaths During Oral Surgery. In: Selby H (Ed) The Inquest Handbook, Leichardt, NSW, Australia: The Federation Press; 1998;150-169 and co-author with Drs. Keith Anderson, Christopher Pysyk and JN Armstrong of Anaesthesia. In: Freckelton I and Selby H (Eds). Expert Evidence. Thomson Reuters, Australia, 2017. E-Mail : [email protected] 200 航空宇宙政策․法學會誌 第 33 卷 第 2 號 Ⅰ. Introduction Barely more than a century has passed since the first passenger was carried by an aircraft. That individual was Henri Farman, an Anglo-French painter turned aviator. He was a passenger on a flight piloted by Léon Delagrange, a French sculptor turned aviator, and aircraft designer and manufacturer. -

Prof. Paul Stephen Dempsey
AIRLINE ALLIANCES by Paul Stephen Dempsey Director, Institute of Air & Space Law McGill University Copyright © 2008 by Paul Stephen Dempsey Before Alliances, there was Pan American World Airways . and Trans World Airlines. Before the mega- Alliances, there was interlining, facilitated by IATA Like dogs marking territory, airlines around the world are sniffing each other's tail fins looking for partners." Daniel Riordan “The hardest thing in working on an alliance is to coordinate the activities of people who have different instincts and a different language, and maybe worship slightly different travel gods, to get them to work together in a culture that allows them to respect each other’s habits and convictions, and yet work productively together in an environment in which you can’t specify everything in advance.” Michael E. Levine “Beware a pact with the devil.” Martin Shugrue Airline Motivations For Alliances • the desire to achieve greater economies of scale, scope, and density; • the desire to reduce costs by consolidating redundant operations; • the need to improve revenue by reducing the level of competition wherever possible as markets are liberalized; and • the desire to skirt around the nationality rules which prohibit multinational ownership and cabotage. Intercarrier Agreements · Ticketing-and-Baggage Agreements · Joint-Fare Agreements · Reciprocal Airport Agreements · Blocked Space Relationships · Computer Reservations Systems Joint Ventures · Joint Sales Offices and Telephone Centers · E-Commerce Joint Ventures · Frequent Flyer Program Alliances · Pooling Traffic & Revenue · Code-Sharing Code Sharing The term "code" refers to the identifier used in flight schedule, generally the 2-character IATA carrier designator code and flight number. Thus, XX123, flight 123 operated by the airline XX, might also be sold by airline YY as YY456 and by ZZ as ZZ9876. -

4/22/2016 Qrycanadianairtaxi Page 1 Regst# O P E R a T O R S N a M E
qryCanadianAirTaxi 4/22/2016 Regst# O p e r a t o r s N a m e TypeofFiling City&Providence DateApvd 657 2080061 Ontario Inc (SkyCare) initial Sioux, Lookout ON 03/13/13 650-A 7506406 Canada Inc. amended Mississauga, Ontario 04/13/12 348 A.T.R. Seminars Inc. cob Airline Traini initial Toronto, Ontario 6/4/93 581-A Acass Canada Ltd. initial Montreal, Quebec 12/24/09 432-B Adler Aviation Ltd. initial Breslau, Ontario 10/15/96 202-B Aero Academy Inc. amended London, Ontario 2/18/10 645 AeroclubDeMontreal/Univair see 382 amended Saint-Hubert, Quebec 01/24/11 185-A Air 500 , a division of I.M.P. Group Li amended Halifax, Nova Scotia 10/1/05 644 Air Bravo Corp initial Blind River, Ontario 05/14/10 668 Air Gaspesie, Inc. initial St-Bruno, Quebec 09/10/14 410 Air Georgian Limited (Simo Air Limited initial Barrie. Ontario 4/6/95 510 Air Inuit Ltd./Air Inuit Ltee amended Dorval, Quebec 2/28/0 381 Air Killarney Limited initial Killarney, Ontario 4/11/94 538 Air Limo Canada Inc. initial Quebec, Canada 9/13/01 199 Air Nova Inc. initial St. John's, Newfoundla 4/3/87 578 Air Nunavut initial Iqualuit, X0A 0H0. CA 08/11/03 616-C Air Partners Corp. amended Canada 10/20/10 480 Air Rainbow Mid-Coast initial Campbell River, BC 6/4/98 Airbourne Energy Solutions Ltd. (See 347-A Airco Aircraft Charters Ltd. amended Edmonton, Alberta 02/22/2001 595-A AirExpress Ontario amended Oshawa, Ontario 05/04/10 511 Airspec Corporation Ltd. -

Jeox FP)1.0 CANADIAN TRANSPORTATION RESEARCH FORUM Lip LE GROUPE DE RECHERCHES SUR LES TRANSPORTS AU CANADA
jEOX FP)1.0 CANADIAN TRANSPORTATION RESEARCH FORUM Lip LE GROUPE DE RECHERCHES SUR LES TRANSPORTS AU CANADA 20th ANNUAL MEETING PROCEEDINGS TORONTO, ONTARIO MAY 1985 591 AT THE CROSSROADS - THE FINANCIAL HEALTH OF CANADA'S LEVEL I AIRLINES by R.W. Lake,. J.M. Serafin and A., Mozes Research Branch, Canadian Transport Commission INTRODUCTION In 1981 the Air Transport Committee and the 'Research Branch of the Canadian Transport Commission on a joint basis, and in conjunction with the major Canadian airlines, (who formed a Task Force) undertook a programme of studies concerning airline pricing and financial performance. This paper is based on a CTC Working Paper' which presented current data on the topic, and interpreted them in the context of the financial and regulatory circumstances faced by the airlines as of July 1984. ECONOMIC PERSPECTIVE The trends illustrated in Figure 1 suggest that air trans- portation may have reached the stage of a mature industry with air . travel/transport no longer accounting for an increasing proportion of economic activity. This mile/stone in the industry's life cycle, if in fact it has been reached, would suggest that an apparent fall in the income elasticity of demand for air travel between 1981 and 1983 could persist. As data reflecting the apparent demand re- surgence of 1984 become available, the picture may change, but 1 LAKE Figure 2 Figure 1 AIR FARE INDICES AIR TRANSPORT REVENUE AS A PERCENT OF GROSS NATIONAL PRODUCT 1.90 1.20.. 1.80. 1.70 - 1.10 -, 1.60. ..... 1.50. .. 8 .: . 1.40 -, r,.