Management of Surgical Wound Dehiscence
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Arterial Leg Ulcer Clinical Pathway
Waterloo Wellington Integrated Wound Care Program Evidence-Based Wound Care Arterial Leg Ulcer Clinical Pathway 0-7 Days Expected Outcomes Notes Most Responsible Physician(MRP)/Nurse Practitioner (NP) Refer patient to ‘Care Connects’ if no responsible practitioner currently involved with patient identified/informed Determine if MRP/NP is part of Family Health Team (FHT) or Community Health Centre (CHC) and consider additional supports available Medical/surgical history and co-morbidity management Risk factors include: Chronic renal disease considered within care plan Smoking Congestive heart failure Diabetes mellitus Impaired liver function Hyperlipidemia Use of systemic steroids, Hypertension immunosuppressive and chemotherapy Coronary artery disease >70 years of age History of cerebral vascular accident Age 50-69 years with history of diabetes (CVA) or smoking Low hemoglobin < 50 years with diabetes and one other Obesity atherosclerotic factor Poor nutrition History of vascular surgery or deep vein Decreased thyroid function thrombosis Psoriasis Bleeding disorders Autoimmune diseases Family history of arterial disease Medication reconciliation and their impact on wound healing Prescription, non-prescription, naturopathic and illicit drug use (including e-cigarettes, reviewed inhaled substances and nicotine replacement therapy) Medications that can affect healing include: chemotherapy, anticoagulants, antiplatelets, corticosteroids, vasoconstrictors, antihypertensives, diuretics and immunosepressive drugs Other -

Caring for Yourself After Surgery: Preventing Surgical Site Infections
CARE AT HOME SERIES CARE AT HOME SERIES Caring for Yourself After Surgery Caring for Yourself After Surgery Preventing Surgical Site Infections Preventing Surgical Site Infections Wounds Canada has developed this simple guide that can be used by patients and their care partners when they are looking after a surgical wound. It provides guidance on things to do before and after surgery to help prevent infections and recognize the signs of infections if they do occur. In the past, people stayed in hospital for days or weeks following surgery. In those days, many of the complications that can occur soon after surgery (like infections, heart problems or bleeding) were treated when patients were still recovering in hospital. Today, patients having surgery get home Uninfected, healed surgical incision site. (See page 4 for faster than ever, often even the same day. Surgical uninfected and infected surgical incision sites.) site infections (SSIs) that were once treated in hospital are now being managed by patients at home. The good news is that there are actions you can take before and after your surgery to reduce the chances of developing a serious SSI. What is a surgical site infection? A surgical site infection is a problem where there are too many bacteria or really dangerous, active bacteria in your surgical incision. SSIs cause pain and delay wound healing. In more severe cases, SSIs can spread into the bloodstream (a condition called sepsis), which can lead to tissue loss, organ failure and death. A surgical site infection can be on the surface or deep. How much damage it does depends on how healthy you are as well as how strongly the bacteria affect your tissues. -

Causes of Surgical Wound Dehiscence: a Multicenter Study
J Wound Manag Res 2018 September;14(2):74-79 pISSN 2586-0402 https://doi.org/10.22467/jwmr.2018.00374 eISSN 2586-0410 Journal of Wound Management and Research Causes of Surgical Wound Dehiscence: A Multicenter Study Jeong Jin Chun1, Seok Min Yoon1, Woo Jin Song1, Hyun Gyo Jeong1, Chang Yong Choi2, Syeo Young Wee1 1Department of Plastic and Reconstructive Surgery, College of Medicine, Soonchunhyang University, Gumi; 2Department of Plastic and Reconstructive Surgery, College of Medicine, Soonchunhyang University, Bucheon, Korea Abstract Surgical wound dehiscence is a postoperative complication involving breakdown of surgical incision site. Despite the in- creased knowledge of wound healing mechanism before and after surgery, wound dehiscence may increase the length of hospital stay, increase patient inconvenience and rates of re-operation. The purpose of this study was to analyze the causes of wound dehiscence in patients undergoing reoperation at 4 hospitals of Soonchunhyang Medical Center. The number of patients in each hospital and those operated previously were compared. In addition, other characteristics of patients were compared in patients who underwent reoperation. In 22 out of 1,026 patients consulted at the Seoul hos- pital, 32 cases out of 1,295 at Bucheon hospital, 14 cases out of 1,687 at Cheonan hospital and 15 cases out of 374 at Gumi hospital, wound revision was performed for wound dehiscence. Patients at the Department of Obstetrics and Gy- necology were the most common and included 33 patients (39.8%). The most common intervention before wound revi- sion was Cesarean section in 14 patients (19.3%). In this study, we retrospectively reviewed patients who underwent wound revision due to wound dehiscence and analyzed the underlying causes of the postoperative complication. -
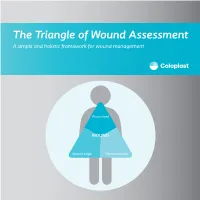
The Triangle of Wound Assessment a Simple and Holistic Framework for Wound Management
The Triangle of Wound Assessment A simple and holistic framework for wound management Wound bed WOUND Wound edge Periwound skin We asked healthcare professionals around the world about their priorities ? for wound care We found that most people Respondents said that treating wounds are not protecting the periwound specialists in a hospital1 skin is very important1 Approximately Up to 79% of wounds are 70% of being treated in wounds are the community2 surrounded by unhealthy skin3 2 ...none However, in a recent met all of the study of 14 wound criteria for assessment tools ... optimal wound assessment4 The Triangle of Wound Assessment is a holistic framework that allows practitioners üto assess and manage all areas of the wound, including the periwound skin. It is a simple and systematic approach that guides the user Wound bed from complete wound WOUND assessment to setting management goals, and Wound edge Periwound skin selecting the optimal treatment. 3 The Triangle of Wound Assessment offers a systematic approach to wound management Optimal wound management starts with a holistic wound assessment. This will help to more efficiently set management goals, which will increase the potential for better treatment outcomes. Assessment Management Goals Treatment 4 This is achieved through a holistic framework The Triangle of Wound Assessment provides a framework to assess all three areas of the wound while remembering the patient behind the wound within their social context. Patient Wound bed Social context WOUND Wound Wound edge Periwound skin 5 It’s not just about the wound but also the patient behind the wound Optimal management of the wound starts with assessing the patient behind the wound, and the social context in which the patient lives. -

Guideline: Wound Bed Preparation for Healable and Non Healable Wounds
British Columbia Provincial Nursing Skin and Wound Committee Guideline: Wound Bed Preparation for Healable and Non Healable Wounds Developed by the BC Provincial Nursing Skin and Wound Committee in collaboration with Wound Clinicians from: / TITLE Guideline: Wound Bed Preparation for Healable and Non-Healable Wounds in Adults & Children1 Practice Level Nurses in accordance with health authority and agency policy. Conservative sharp wound debridement (CSWD) is a restricted activity according to the Nurse’s (Registered) and Nurse Practitioner Regulation. 2 CRNBC states that registered nurses must successfully complete additional education and follow an established guideline when carrying out CSWD. Biological debridement therapy is a restricted activity according to the Nurse’s (Registered) and Nurse Practitioner Regulation. 3 CRNBC states that registered nurses must follow an established guideline when carrying out biological debridement. Clients 4 with wounds needing wound bed preparation require an interprofessional approach to provide comprehensive, evidence-based assessment and treatment. This clinical practice guideline focuses solely on the role of the nurse, as one member of the interprofessional team providing care to these clients. Background Factors affecting wound healability include the presence of adequate circulation in the area of the wound, wound related factors such as the size and duration of the wound, the ability to treat the cause of the wound and the presence of risk factors impacting wound healing. While many wounds heal, others are determined to be non-healing or slow-to-heal based on the presence or absence of these factors. Wound healability must be determined prior to debridement and moist wound healing. Although wound healing normally occurs in a predictable fashion, wound healing trajectories can be heterogeneous and non- uniform resulting is delayed wound healing for some clients. -

Risk Factors for Surgical Wound Dehiscence by Hazim Ibrahim DPM 1
! The Northern Ohio Foot and Ankle Journal Official Publication of the NOFA Foundation A Literature Review of Causes and Risk Factors for Surgical Wound Dehiscence by Hazim Ibrahim DPM 1 The Northern Ohio Foot and Ankle Journal 4(26): 1-5 Abstract: Postoperative wound healing plays a significant role in facilitating a patient’s recovery and rehabilitation. Surgical wound dehiscence (SWD) impacts mortality and morbidity rates and significantly contributes to prolonged hospital stays and associated psychosocial stressors on individuals and their families. Most common risk factors associated with SWD include obesity and wound infections, particularly in the case of orthopedic surgery. There is limited reporting of variables associated with SWD across other surgical domains and a lack of risk assessment tools. Furthermore, there was a lack of clarity in the definition of SWD in the literature. This review provides an overview of the available research and provides a basis for more rigorous analysis of factors that contribute to SWD. Key words: Dehiscence, wound infection, obesity This is an Open Access article distributed under the terms of the Creative Commons Attribution License. It permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ©The Northern Ohio Foot and Ankle Foundation Journal. (www.nofafoundation.org) 2016. All rights reserved. time. The third week after surgery the durability equals 20% of the initial strength, and after 6-12 Wound dehiscence is one of the most weeks it reaches 70-80% (1). Sutures placed during surgery allow the tissues the necessary time to regain common complications of surgical incision sites. -
Suturing with U-Technique Versus Un
Official Title of the Study: Suturing with U-Technique versus Un- Reapproximated wound Edges during removal of Closed Thoracostomy-tube drain - A single centre Open-label randomized prospective trial (SUTURE TRIAL) NCT NUMBER: Not Yet Assigned DATE OF DOCUMENT: January 16, 2019 1 STUDY SUMMARY Title: Suturing with U-Technique versus Un-Reapproximated wound Edges during removal of Closed Thoracostomy-tube drain - A single centre Open-label randomized prospective trial (SUTURE TRIAL) Background: Closed thoracostomy tube drainage or chest tube insertion is one of the most commonly performed procedures in thoracic surgery. There are several published evidence-based guidelines on safe performance of a chest tube insertion. However, there is absence of prospective controlled trials or systematic reviews indicating the safest technique of closing the wound created at the time of chest tube insertion and that best guarantees good wound and overall outcomes, post-chest tube removal. The use of a horizontal mattress non-absorbable suture or U- suture which is placed at the time of chest tube insertion and used to create a purse-string wound re-approximation at the time of tube removal has been an age-long and time-honored practice in most thoracic surgical settings. It has been established by a recent study that an occlusive adhesive-absorbent dressing can also be safely used to occlude the wound at the time of chest tube removal with good wound and overall outcomes though the study focused on tubes inserted during thoracic surgical operations. -

A Focus on the Triangle of Wound Assessment — Addressing the Gap Challenge and Identifying Suspected Biofilm in Clinical Practice
Clinical practice A focus on the Triangle of Wound Assessment — addressing the gap challenge and identifying suspected biofilm in clinical practice Authors: Wound assessment should be comprehensive, systematic and evidence- Caroline Dowsett, Terry Swanson and Tonny Karlsmark based (World Union of Wound Healing Societies [WUWHS], 2016a). The Triangle of Wound Assessment offers clinicians a framework to assess the patient and their wound, taking into consideration the wound bed, wound edge and periwound skin (Dowsett et al, 2015). The framework can be adapted to incorporate new developments and new challenges in wound care such as the ‘gap challenge’ and biofilm prevention and management. Using the framework can assist in determining the status of the wound bed and support clinical decision making to prevent problems associated with exudate pooling at the wound bed and the potential for biofilm formation. he Triangle of Wound Assessment This article will discuss how the Triangle of was established in 2014 and provides Wound Assessment identifies infection and T a systematic approach to wound biofilm, tackles the gap challenge, and how assessment and in setting management goals, this framework can be developed for new to guide optimal treatment choice (Dowsett et challenges in wound care. al, 2015), ensuring that the periwound skin is incorporated into the assessment. Periwound The importance of holistic assessment skin can be a significant problem in patients Wounds are a significant source of cost to with chronic wounds, with between 60–70% patients, as well as to the health economy. of wounds found to be surrounded by either Chronic wounds are often hard to heal problematic or unhealthy periwound skin resulting in a cycle of pain, anxiety and (Cartier et al, 2014). -

Corticosteroids and Wound Healing: Clinical Considerations in the Perioperative Period
The American Journal of Surgery (2013) 206, 410-417 Review Corticosteroids and wound healing: clinical considerations in the perioperative period Audrey S. Wang, M.D.a,*, Ehrin J. Armstrong, M.D., M.Sc.b, April W. Armstrong, M.D., M.P.H.a aDepartment of Dermatology, University of California, Davis, 3301 C Street, Suite 1400, Sacramento, CA 95816; bDepartment of Internal Medicine, Division of Cardiovascular Medicine, University of California, Davis, 4860 Y Street, Suite 2820, Sacramento, CA 95817 KEYWORDS: Abstract Corticosteroids; BACKGROUND: Determining whether systemic corticosteroids impair wound healing is a clinically Wound healing; relevant topic that has important management implications. Perioperative METHODS: We reviewed literature on the effects of corticosteroids on wound healing from animal and human studies searching MEDLINE from 1949 to 2011. RESULTS: Some animal studies show a 30% reduction in wound tensile strength with perioperative corticosteroids at 15 to 40 mg/kg/day. The preponderance of human literature found that high-dose cor- ticosteroid administration for ,10 days has no clinically important effect on wound healing. In patients taking chronic corticosteroids for at least 30 days before surgery, their rates of wound complications may be increased 2 to 5 times compared with those not taking corticosteroids. Complication rates may vary depending on dose and duration of steroid use, comorbidities, and types of surgery. CONCLUSIONS: Acute, high-dose systemic corticosteroid use likely has no clinically significant effect on wound healing, whereas chronic systemic steroids may impair wound healing in susceptible individuals. Ó 2013 Elsevier Inc. All rights reserved. The effects of corticosteroids on wound healing have perioperative corticosteroid administration, namely, dosing, been a topic of great interest among surgeons, internists, and chronicity, and timing relative to surgery. -

Resistant Staphylococcus Aureus Infection in a Diabetic Patient with Femorotibial Vascular Bypass Occlusion
ORIGINALACUTE MEDICAL RESEARCH CARE ClinicalClinical Medicine Medicine 2020 2017 Vol 20, Vol No 17, 1: No 98–100 6: 98–8 Surgical wound dehiscence complicated by methicillin- resistant Staphylococcus aureus infection in a diabetic patient with femorotibial vascular bypass occlusion Authors: Enrico M Zardi,A Nunzio Montelione,B Rossella C Vigliotti,C Camilla Chello,D Domenico M Zardi,E Francesco SpinelliF and Francesco StiloG Diabetic patients with critical limb ischaemia may be affected combined with endarterectomy of the superficial femoral artery. A by severe wound and skin ulcer infections. We report a case of month later he underwent the calcaneal skin ulcers debridement. a patient with bilateral femorotibial occlusion and methicillin- The wound specimen for bacterial culture was positive for resistant Staphylococcus aureus infection. The patient was Staphylococcus haemolyticus, Corynebacterium aurimucosum treated with femoroperoneal vascular bypass, debridement and Corynebacterium simulans, he was treated with intravenous ABSTRACT of wound dehiscence and targeted antimicrobial therapy for teicoplanin at 400 mg once per day and intravenous meropenem symptom resolution and healing of the wound. at 500 mg every 8 hours. In June and July, he was admitted to our hospital for rest pain and persistence of bilateral calcaneal KEYWORDS: Diabetes, infection, skin ulcer, therapy, vascular bypass ulcers; he was treated with left femorotibial posterior bypass and right femorotibial anterior bypass, using the greater saphenous vein. After an additional -

Clinician Assessment Tools for Patients with Diabetic Foot Disease: a Systematic Review
Journal of Clinical Medicine Review Clinician Assessment Tools for Patients with Diabetic Foot Disease: A Systematic Review Raúl Fernández-Torres 1 , María Ruiz-Muñoz 1,* , Alberto J. Pérez-Panero 1 , Jerónimo C. García-Romero 2 and Manuel Gónzalez-Sánchez 3 1 Department of Nursing and Podiatry, University of Málaga, Arquitecto Francisco Peñalosa, s/n. Ampliación Campus de Teatinos, 29071 Málaga, Spain; [email protected] (R.F.-T.); [email protected] (A.J.P.-P.) 2 Medical School of Physical Education and Sports, University of Málaga, C/Jiménez Fraud 10. Edificio López de Peñalver, 29010 Málaga, Spain; [email protected] 3 Department of Physiotherapy, University of Málaga, Arquitecto Francisco Peñalosa, s/n. Ampliación campus de Teatinos, 29071 Málaga, Spain; [email protected] * Correspondence: [email protected]; Tel.: +34-951953215 Received: 10 April 2020; Accepted: 12 May 2020; Published: 15 May 2020 Abstract: The amputation rate in patients with diabetes is 15 to 40 times higher than in patients without diabetes. To avoid major complications, the identification of high-risk in patients with diabetes through early assessment highlights as a crucial action. Clinician assessment tools are scales in which clinical examiners are specifically trained to make a correct judgment based on patient outcomes that helps to identify at-risk patients and monitor the intervention. The aim of this study is to carry out a systematic review of valid and reliable Clinician assessment tools for measuring diabetic foot disease-related variables and analysing their psychometric properties. The databases used were PubMed, Scopus, SciELO, CINAHL, Cochrane, PEDro, and EMBASE. The search terms used were foot, ankle, diabetes, diabetic foot, assessment, tools, instruments, score, scale, validity, and reliability. -

Assessment and Management of Pressure Injuries for the Interprofessional Team Third Edition Disclaimer
Clinical Best Practice Guidelines MAY 2016 Assessment and Management of Pressure Injuries for the Interprofessional Team Third Edition Disclaimer Th ese guidelines are not binding on nurses, other health care professionals, or the organizations that employ them. Th e use of these guidelines should be fl exible, and based on individual needs and local circumstances. Th ey neither constitute a liability nor discharge from liability. While every eff ort has been made to ensure the accuracy of the contents at the time of publication, neither the authors nor the Registered Nurses’ Association of Ontario (RNAO) gives any guarantee as to the accuracy of the information contained in them or accepts any liability with respect to loss, damage, injury, or expense arising from any such errors or omissions in the contents of this work. Copyright With the exception of those portions of this document for which a specifi c prohibition or limitation against copying appears, the balance of this document may be produced, reproduced, and published in its entirety, without modifi cation, in any form, including in electronic form, for educational or non-commercial purposes. Should any adaptation of the material be required for any reason, written permission must be obtained from RNAO. Appropriate credit or citation must appear on all copied materials as follows: Registered Nurses’ Association of Ontario (2016). Assessment and Management of Pressure Injuries for the Interprofessional Team, Th ird Edition. Toronto, ON: Registered Nurses’ Association of Ontario. Th is work is funded by the Ontario Ministry of Health and Long-Term Care. All work produced by RNAO is editorially independent from its funding source.