Nepal | Editorial Committee
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Duty Station: Kathmandu, Nepal
INDIVIDUAL CONSULTANT PROCUREMENT NOTICE (International Consultant – Human Rights Expert) UNDP/PN/31/2017 Date: 31 July 2017 Country: Nepal Description of the assignment: SPSP project needs a Human Rights Expert. He/She will be responsible to provide day-to-day management and technical support to implement the Project activities and ensure that the Project objectives are met as set out in the Project document. The expert will report directly to the Deputy Country Director (Programme) and be responsible to the secretary of the NHRC. Number of consultant required: 1 Project name: Strategic Plan Support Project for the National Human Rights Commission (SPSP) Period of assignment/services (if applicable): 01 September – 31 December 2017 (not to exceed 87 days in total) Duty Station: Kathmandu, Nepal Proposal should be submitted at the following address: Procurement Unit, UNDP (Ref.: UNDP/PN/31/2017: Human Rights Expert, UN House, Pulchowk, PO Box 107, Kathmandu, Nepal or by email to [email protected] not later than 1730 hours (Nepal Standard Time) of 09 August 2017. Any request for clarification must be sent in writing, or by standard electronic communication to the e- mail: [email protected] mentioning Procurement Notice Ref: UNDP/PN/31/2017: Human Rights Expert, on or before 03 August 2017. The procurement unit will respond in writing, including an explanation of the query without identifying the source of inquiry, to all consultants or via bulletin published on the UNDP website: http://www.np.undp.org/content/nepal/en/home/operations/procurement.html. Inquiries received after the above date and time shall not be entertained. -

Docusign Envelope ID: 3F71DABF-9E5D-4742-9D5D-E477C06C49A4 Docusign Envelope ID: 3F71DABF-9E5D-4742-9D5D-E477C06C49A4
DocuSign Envelope ID: 3F71DABF-9E5D-4742-9D5D-E477C06C49A4 DocuSign Envelope ID: 3F71DABF-9E5D-4742-9D5D-E477C06C49A4 IMPORTANT INFORMATION or at Phuentsholing check post. Further advice from Customs authorities in the US At Greaves Tours LLC we strongly hope that your information on Visas for Bhutan may be before departing on your tour. When shopping holiday lives up to your expectations. Our years discussed with your travel consultant or for expensive items such as precious stones, of experience in dealing with the Indian through the Bhutan Mission to the United carpets etc, the shopkeepers may guarantee the Subcontinent has gone into formulating the tour Nations in New York Tel: 1-212-682-2268 authenticity of the item, however expert programs on offer. Due care has been taken to knowledge is essential to ascertain their true put the best possible ground arrangements in TIBET: value. Please note that Greaves Tours LLC place for you to have a memorable holiday. Visas for Tibet will be processed by Greaves cannot be held responsible for any purchase that Tours LLC. The cost of the Visa for Tibet is you make and nor can we take up However, we seek your patience and included in your tour price. Visa applications correspondence on your behalf if you are not understanding while travelling in the and documentation will be completed by you satisfied with the item purchased or if goods are Subcontinent. Sometimes minor problems may on tour whilst in Kathmandu, en route to Tibet. not delivered in time. We pride ourselves on the occur, but our ground staff will always be on Only once the Visa has been cleared can quality of our sightseeing guides, however if at hand to try and solve such occurrences. -
![JOURNEY to the END of the EARTH BY-TISHANI DOSHI CLASS XII ENGLISH [CORE] VISTAS PRESENTED by MRS LILY KUMAR DELHI PUBLIC SCHOOL RANCHI Akademik Shokalskiy](https://docslib.b-cdn.net/cover/5738/journey-to-the-end-of-the-earth-by-tishani-doshi-class-xii-english-core-vistas-presented-by-mrs-lily-kumar-delhi-public-school-ranchi-akademik-shokalskiy-615738.webp)
JOURNEY to the END of the EARTH BY-TISHANI DOSHI CLASS XII ENGLISH [CORE] VISTAS PRESENTED by MRS LILY KUMAR DELHI PUBLIC SCHOOL RANCHI Akademik Shokalskiy
JOURNEY TO THE END OF THE EARTH BY-TISHANI DOSHI CLASS XII ENGLISH [CORE] VISTAS PRESENTED BY MRS LILY KUMAR DELHI PUBLIC SCHOOL RANCHI Akademik Shokalskiy • MV Akademik Shokalskiy (Russian: Академик Шокальский) is an Akademik Shuleykin-class ice- strengthened ship, built in Finland in 1982 and originally used for oceanographic research.In 1998 she was fully refurbished to serve as a research ship for Arctic and Antarctic work; she is used also for expedition cruising. She is named after the Russian oceanographer Yuly Shokalsky. • For two weeks from 25 December 2013 Akademik Shokalskiy was trapped in thick ice in Commonwealth Bay, Antarctica, while operating an expedition for the Australasian Antarctic Expedition 2013-2014. The scientists and passengers were evacuated on 2 January. Introduction to the author: tishani doshi Tishani Doshi (9 December 1975) is an Indian poet, journalist and a dancer based in Chennai. Born in Madras, India, to a Welsh mother and Gujarati father, she graduated with a Master’s degree in Creative Writing from the Johns Hopkins University. She received Eric Gregory Award in 2001. Her first poetry collection Countries of the Body won the 2006 Forward Poetry Prize for the best first collection. Her First novel The Pleasure Seekers was published by Bloomsbury in 2010 and was long-listed for the Orange Prize in 2011 and shortlisted for The Hindu Best Fiction Award in 2010. She works as a freelance writer and worked with choreographer Chandralekha. Her poetry collection Everything Begins Elsewhere was published by Copper Canyon Press in 2013. Her most recent book of poetry, Girls Are Coming Out Of the Woods, was published by HarperCollins India in 2017. -

PGNP Native OLE DB Provider for Postgresql, Greenplum, Redshift Developer’S Manual
CATA 2021 PGNP Native OLE DB Provider for PostgreSQL, Greenplum, Redshift Developer’s Manual This document contains description of various PGNP features, use cases and programming techniques. It is written for professional developers. Konstantin Izmailov Copyright © 2006-2019. All Rights Reserved. 2/12/2021 This document is property of PGNP team. Neither a part nor the entire document can be reproduced, changed, distributed or published without prior written permission of owners. Please contact us if you have any questions: [email protected]. Page 2 Table of Contents 1 Introduction .................................................................................................................................................................... 6 2 Installation and Product Activation ................................................................................................................................ 7 2.1.1 UI based installation ........................................................................................................................................ 7 2.1.2 Unattended/silent installation ...................................................................................................................... 10 2.1.3 Activation on a computer behind a firewall (in DMZ) .................................................................................. 11 3 Provider’s Features ...................................................................................................................................................... -

NATIVE SAML SUPPORT for SSO FFTH – RSA Archer 6.8
▪ Dell Customer Communication - Confidential NATIVE SAML SUPPORT FOR SSO FFTH – RSA Archer 6.8 1 ▪ Dell Customer Communication - Confidential AGENDA NATIVE SAML 2.0 SUPPORT FOR SSO ▪ Background ▪ Overview ▪ Troubleshooting ▪ Demo 2 ▪ Dell Customer Communication - Confidential BACKGROUND ▪ Main Goal: Provide native SAML 2.0 support for SSO to RSA Archer platform ▪ Prior To 6.8, RSA Archer could not process SAML 2.0 assertions natively ▪ Required using ADFS as middleware to convert SAML assertions to Windows Federated claims ▪ Increased complexity of enabling integration with SAML IDP ▪ Security concerns with ADFS served as an implementation roadblock ▪ Enabling native processing of SAML assertions eliminates the need for ADFS 3 ▪ Dell Customer Communication - Confidential OTHER GOALS ▪ Support multiple SAML identity providers for a single instance ▪ Provide vanity URLs to automatically redirect to a specific identity provider ▪ Provide Service Provider metadata for easier setup in identity provider ▪ Support automatic user provisioning ▪ Support user profile, group membership, and role assignment updates via SSO ▪ Improved logging to aid in troubleshooting authentication issues − Errors point to specific log reference in stand-alone SAML log file − Info level logging provides entire request and assertion contents ▪ Leave Federation SSO option as is 4 ▪ Dell Customer Communication - Confidential OVERVIEW 5 ▪ Dell Customer Communication - Confidential CONFIGURING SAML SSO ▪ SAML SSO is enabled by selecting the new SAML Single Sign-On Mode -
Research Report Irides Fact-Finding and Relationship-Building Mission
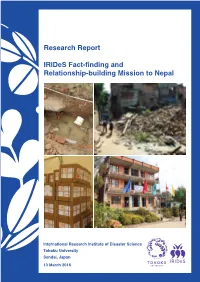
Research Report InternationalResearch Research Institute of Disaster Science Research Report IRIDeS Fact-finding and Relationship-building Mission to Nepal IRIDeS Fact-finding and Relationship-building Mission to Nepal International Research Institute of Disaster Science Tohoku University Sendai, Japan 13 March 2016 IRIDeS Fact-Finding and relationship-building mission to Nepal IRIDeS Task Force Team Hazard and Risk Evaluation Research Division: Prof. F. Imamura, Prof. S. Koshimura, Dr. J. D. Bricker, Dr. E. Mas Human and Social Response Research Division: Prof. M. Okumura, Dr. R. Das, Dr. E. A. Maly Regional and Urban Reconstruction Research Division: Dr. S. Moriguchi, Dr. C. J. Yi Disaster Medical Science Division: Prof. S. Egawa (Team Leader), Prof. H. Tomita, Emeritus Prof. T. Hattori, Dr. H. Chagan-Yasutan, Dr. H. Sasaki Disaster Information Management and Public Collaboration Division: Dr. A. Sakurai i IRIDeS Fact-Finding and relationship-building mission to Nepal IRIDeS would like to expresses our gratitude to the following people: IRIDeS Task Force Team ¥ Mr. Khagaraj Adhikari Minister, MoHP ¥ Dr. Lohani Guna Raj, Secretary, MoHP ¥ Dr. Basu Dev. Pandey, Director, Division of Leprosy Control, MoHP ¥ Dr. Khem Karki; Member Secretary, Nepal Health Research Council, MoHP Hazard and Risk Evaluation Research Division: ¥ Mr. Edmondo Perrone, Cluster coordinator/World Food Program Prof. F. Imamura, Prof. S. Koshimura, Dr. J. D. Bricker, Dr. E. Mas ¥ Mr. Surendra Babu Dhakal, World Vision Internationa ¥ Mr. Prafulla Pradhan, UNHabitat ¥ Mr. Vijaya P. Singh, Assistant Country Director, UNDP Nepal Office Human and Social Response Research Division: ¥ Mr. Rajesh Sharma, Programme Specialist UNDP Bangkok Regional Hub Prof. M. Okumura, Dr. R. Das, Dr. -
Time Zone Table
TIME ZONE TABLE To set the time on your equipment console, use the table below to locate the INDEX number associated with your time zone. INDEX NAME OF TIME ZONE TIME IANA TIME ZONE 10 Azores Standard Time (GMT-01:00) Azores Atlantic/Azores 12 Cape Verde Standard Time (GMT-01:00) Cape Verde Islands Atlantic/Cape_Verde 43 Mid-Atlantic Standard Time (GMT-02:00) Mid-Atlantic Atlantic/South_Georgia 27 E. South America Standard Time (GMT-03:00) Brasilia America/Sao_Paulo 58 SA Eastern Standard Time (GMT-03:00) Buenos Aires, Georgetown America/Argentina/Buenos_Aires 35 Greenland Standard Time (GMT-03:00) Greenland America/Godthab 51 Newfoundland Standard Time (GMT-03:30) Newfoundland and Labrador America/St_Johns 06 Atlantic Standard Time (GMT-04:00) Atlantic Time (Canada) America/Halifax 60 SA Western Standard Time (GMT-04:00) Caracas, La Paz America/La_Paz 17 Central Brazilian Standard Time (GMT-04:00) Manaus America/Cuiaba 54 Pacific SA Standard Time (GMT-04:00) Santiago America/Santiago 59 SA Pacific Standard Time (GMT-05:00) Bogota, Lima, Quito America/Bogota 28 Eastern Standard Time (GMT-05:00) Eastern Time (US and Canada) America/New_York 70 US Eastern Standard Time (GMT-05:00) Indiana (East) America/Indiana/Indianapolis 15 Central America Standard Time (GMT-06:00) Central America America/Costa_Rica 21 Central Standard Time (GMT-06:00) Central Time (US and Canada) America/Chicago 22 Central Standard Time (Mexico) (GMT-06:00) Guadalajara, Mexico City, Monterrey America/Monterrey 11 Canada Central Standard Time (GMT-06:00) Saskatchewan -

Service Bulletin: Viafit 2.0 Supplement Sheet
Service Bulletin: ViaFit 2.0 Supplement Sheet Prepared by: Date Prepared: Regina Templeton 9/23/2015 Models Affected: Elite T7 PROBLEM A limited number of new treadmills with ViaFit 2.0 software have been sent to customers. The cartons were missing a supplement sheet highlighting changes from the v1.0 software. The serial numbers of these treadmills are listed on the following page. SOLUTION The attached 4-page supplement sheet should be used in place of pages 8 and 9 in the OPERATION GUIDE. The supplement sheet is now being included in the carton, and it is also posted on the Horizon website. Treadmill Serial Numbers Container Number Serial Number TM4751505CC00001-TM4751505CC00007 TM4751505CC00009-TM4751505CC00012 TM4751505CC00014-TM4751505CC00027 TM4751505CC00030-TM4751505CC00041 TM4751505CC00043-TM4751505CC00054 GESU5188024 TM4751505CC00057-TM4751505CC00058 TM4751505CC00060-TM4751505CC00070 TM4751505CC00073-TM4751505CC00083 TM4751505CC00085-TM4751505CC00086 TM4751505CC00090-TM4751505CC00098 TM4751507CA00099-TM4751507CA00113 FCIU9814414 TM4751507CB00197-TM4751507CB00294 TGHU6676427 TM4751507CA00001-TM4751507CA00098 TM4751508CB00006 TM4751508CB00010-TM4751508CB00023 TM4751508CB00028 TM4751508CB00044 TM4751508CB00050 CBHU8429138 TM4751508CB00054-TM4751508CB00105 TM4751508CB00107-TM4751508CB00110 TM4751508CB00112-TM4751508CB00115 TM4751508CB00145 TM4751508CB00161 TM4751508CB00179-TM4751508CB00196 TM4751508CB00197-TM4751508CB00220 TM4751508CB00235-TM4751508CB00242 TM4751508CB00251-TM4751508CB00256 TM4751508CB00305-TM4751508CB00313 TM4751508CB00315-TM4751508CB00322 -

Oracle Hyperion Data Relationship Management Web Service API Developer's Guide
Oracle® Hyperion Data Relationship Management, Fusion Edition Release 11.1.2.2.000 Web Service API Developer's Guide Overview ............................................................................................................................... 2 About the Data Relationship Management Web Service ........................................................ 2 Using the Data Relationship Management Web Service ......................................................... 3 Time Zone IDs ..................................................................................................................... 4 Using JDeveloper to Create a Web Service Client .................................................................. 6 New Features in This Release ................................................................................................ 6 Methods .............................................................................................................................. 6 Types .................................................................................................................................. 6 Upgrading Existing API Programs ......................................................................................... 7 Upgrading 11.1.2.1 API Programs ....................................................................................... 7 Changes to Existing Types....................................................................................................... 7 Regenerating Web Service Proxy Classes ................................................................................. -

Destination Knowledge
NEPAL be sent by us. The schedule for the onward flight must be All travellers to Nepal must hold a valid passport. Your confirmed from the nearest Druk Air/Bhutan Airlines passport must be valid for at least six months beyond Office (highly recommended). Please be at the check-in your expected date of departure from Nepal. An entry counter two hours before the expected departure time visa for Nepal is also required. It can be obtained either in for the flight with your passport, e-ticket and Visa advance from your local embassy or upon arrival in Clearance document. Check-in/boarding the flight will not TRAVEL GUIDELINES TO INDIA, NEPAL, Nepal. If you plan to obtain it in Nepal be sure to bring be entertained without the valid passport and Visa BHUTAN & SRI LANKA one extra passport-size photo with you for this purpose. Clearance document. BHUTAN Exit by Air: VISA FORMALITIES Slovenia, Solomon Islands, South Africa, Spain, Sri Lanka, Your passport should be valid for at least six months after The schedule for the return flight will be confirmed by us. Suriname, Swaziland, Sweden, Switzerland, Taiwan, your proposed date of departure from Bhutan. Please be at the check-in counter two hours before the INDIA Tajikistan, Tanzania, Thailand, Tonga, Trinidad & Tobago, expected departure time for the flight with the passport, All foreign nationals entering India are required to Turks & Caicos Island, Tuvalu, UAE, Ukraine, United Visa applications are cleared in advance, and a Visa e-ticket and Visa Clearance document. possess a passport with a valid visa obtained from an Kingdom, Uruguay, USA, Vanuatu, Vatican City-Holy See, Clearance document will be forwarded two weeks prior to Indian Mission or Post abroad. -
Database Manual : Cloudworks
DATABASE MANUAL : CLOUDWORKS Database Manual Document Number: CloudWorks Database Manual Client: User Date: 25 October 2018 Database Version: V7.0 Status: Draft Classification: Confidential S/W File Name CloudWorks Database Manual.docx Copyright Cape Digital Solutions. This document contains information relating to the rights of Cape Digital Solutions. The confidentiality agreement provisions are applicable to this document. When no longer needed for authorised purposes, this document must be destroyed or returned to Cape Digital Solutions. Cape Digital Solutions reserves the right to change the design or specifications of their products without prior notice. The contents of this manual is the property of Cape Digital Solutions and may not be copied or modified without prior permission, in writing, from Cape Digital Solutions, Cape Town, South Africa. DOCUMENT NAME CLASSIFICATION DATE PAGE CLOUDWORKS DATABASE MANUAL CONFIDENTIAL 15-JUL-21 1 OF 9 DATABASE MANUAL : CLOUDWORKS Table of Contents 1 Database Architecture ...................................................................................... 3 2 Connecting to the Database .............................................................................. 5 3 Database Tables ............................................................................................... 6 3.1 System Details Table ............................................................................................................... 6 3.2 System Users Table ................................................................................................................ -

Aras Innovator 11.0 Configuring Internationalization
Aras Innovator 11 Configuring Localization and Internationalization Support Document #: 11.0.02015040601 Last Modified: 1/4/2018 Aras Innovator 11 Configuring Localization and Internationalization Support Copyright Information Copyright © 2018 Aras Corporation. All Rights Reserved. Aras Corporation 300 Brickstone Square Suite 700 Andover, MA 01810 Phone: 978-691-8900 Fax: 978-794-9826 E-mail: [email protected] Website: http://www.aras.com Notice of Rights Copyright © 2018 by Aras Corporation. This material may be distributed only subject to the terms and conditions set forth in the Open Publication License, V1.0 or later (the latest version is presently available at http://www.opencontent.org/openpub/). Distribution of substantively modified versions of this document is prohibited without the explicit permission of the copyright holder. Distribution of the work or derivative of the work in any standard (paper) book form for commercial purposes is prohibited unless prior permission is obtained from the copyright holder. Aras Innovator, Aras, and the Aras Corp "A" logo are registered trademarks of Aras Corporation in the United States and other countries. All other trademarks referenced herein are the property of their respective owners. Notice of Liability The information contained in this document is distributed on an "As Is" basis, without warranty of any kind, express or implied, including, but not limited to, the implied warranties of merchantability and fitness for a particular purpose or a warranty of non- infringement. Aras shall have no liability to any person or entity with respect to any loss or damage caused or alleged to be caused directly or indirectly by the information contained in this document or by the software or hardware products described herein.