Siemens 3T Standard Operating Procedures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Generic Procedures for Assessment and Response During a Radiological
IAEA-TECDOC-1162 Generic procedures for assessment and response during a radiological emergency August 2000 The originating Section of this publication in the IAEA was: Radiation Safety Section International Atomic Energy Agency Wagramer Strasse 5 P.O. Box 100 A-1400 Vienna, Austria Emended version, March 2013. Details of revisions are available at: www.pub.iaea/books/ GENERIC PROCEDURES FOR ASSESSMENT AND RESPONSE DURING A RADIOLOGICAL EMERGENCY IAEA, VIENNA, 2000 IAEA-TECDOC-1162 ISSN 1011–4289 © IAEA, 2000 Printed by the IAEA in Austria August 2000 FOREWORD One of the most important aspects of managing a radiological emergency is the ability to promptly and adequately determine and take actions to protect members of the public and emergency workers. Radiological accident assessment must take account of all critical information available at any time and must be an iterative and dynamic process aimed at reviewing the response as more detailed and complete information becomes available. This manual provides the tools, generic procedures and data needed for an initial response to a non-reactor radiological accident. This manual is one out of a set of IAEA publications on emergency preparedness and response, including Method for the Development of Emergency Response Preparedness for Nuclear or Radiological Accidents (IAEA-TECDOC-953), Generic Assessment Procedures for Determining Protective Actions During a Reactor Accident (IAEA-TECDOC-955) and Intervention Criteria in a Nuclear or Radiation Emergency (Safety Series No. 109). The procedures and data in this publication have been prepared with due attention to accuracy. However, as part of the ongoing revision process, they are undergoing detailed quality assurance checks; comments are welcomed, and following a period of time that will have allowed for a more extensive review, the IAEA will revise the publication as part of the process of continuous improvement. -

Cricothyrotomy
NURSING Cricothyrotomy: Assisting with PRACTICE & SKILL What is Cricothyrotomy? › Cricothyrotomy (CcT; also called thyrocricotomy, inferior laryngotomy, and emergency airway puncture) is an emergency surgical procedure that is performed to secure a patient’s airway when other methods (e.g., nasotracheal or orotracheal intubation) have failed or are contraindicated. Typically, CcT is performed only when intubation, delivery of oxygen, and use of ventilation are not possible • What: CcT is a type of tracheotomy procedure used in emergency situations (e.g., when a patient is unable to breathe through the nose or mouth). The two basic types of CcT are needle CcT (nCcT) and surgical CcT (sCcT). Both types of CcTs result in low patient morbidity when performed by a trained clinician. Compared with the sCcT method, the nCcT method requires less time to set up and is associated with less bleeding and airway trauma • How: Ideally, a CcT is performed within 30 seconds to 2 minutes by making an incision or puncture through the skin and the cricothyroid membrane (i.e., the thin part of the larynx [commonly called the voice box])that is between the cricoid cartilage and the thyroid cartilage) into the trachea –An nCcT is a temporary emergency procedure that involves the use of a catheter-over-needle technique to create a small opening. Because it involves a relatively small opening, it is not suitable for use in extended ventilation and should be followed by the performance of a surgical tracheotomy when the patient is stabilized. nCcT is the only type of CcT that is recommended for children who are under 10 years of age - A formal tracheotomy is a more complex procedure in which a surgical incision is made in the lower part of the neck, through the thyroid gland, and into the trachea. -
Emergency Plan Checklist Center Name: License ID
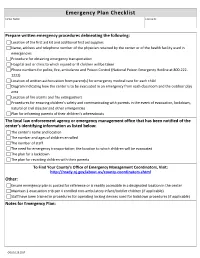
Emergency Plan Checklist Center Name: License ID: Prepare written emergency procedures delineating the following: Location of the first aid kit and additional first aid supplies Name, address and telephone number of the physician retained by the center or of the health facility used in emergencies Procedure for obtaining emergency transportation Hospital and or clinic to which injured or ill children will be taken Phone numbers for police, fire, ambulance and Poison Control (National Poison Emergency Hotline at 800-222- 1222) Location of written authorization from parent(s) for emergency medical care for each child Diagram indicating how the center is to be evacuated in an emergency from each classroom and the outdoor play area Location of fire alarms and fire extinguishers Procedures for ensuring children’s safety and communicating with parents in the event of evacuation, lockdown, natural or civil disaster and other emergencies Plan for informing parents of their children’s whereabouts The local law enforcement agency or emergency management office that has been notified of the center’s identifying information as listed below: The center’s name and location The number and ages of children enrolled The number of staff The need for emergency transportation; the location to which children will be evacuated The plan for a lockdown The plan for reuniting children with their parents To Find Your County’s Office of Emergency Management Coordinators, Visit: http://ready.nj.gov/about-us/county-coordinators.shtml Other: Ensure emergency plan is posted for reference or is readily accessible in a designated location in the center Maintain 1 evacuation crib per 4 enrolled non-ambulatory infant/toddler children (if applicable) Staff have been trained in procedures for operating locking devices used for lockdown procedures (if applicable) Notes for Emergency Plan: OOL/10.28.2017 . -

CONFINED SPACE ENTRY PROGRAM Owner: Risk Management Document Number: EHS S-004 Revision No: 01 Date Last Revised: 08-2-2018
CONFINED SPACE ENTRY PROGRAM Owner: Risk Management Document number: EHS S-004 Revision No: 01 Date last revised: 08-2-2018 Contents 1.0 Applicability ......................................................................................................................................................2 2.0 Scope ...............................................................................................................................................................2 3.0 Definitions ........................................................................................................................................................2 4.0 Core Information and Requirements ...............................................................................................................4 5.0 Roles and Responsibilities ............................................................................................................................ 29 6.0 Goals, Objectives and Performance Measures ............................................................................................ 32 7.0 Training ......................................................................................................................................................... 33 8.0 Program Evaluation ...................................................................................................................................... 34 9.0 Resources .................................................................................................................................................... -
Emergency Procedures Manual
Emergency Procedures Manual Table of Contents I. Purpose ............................................................................................................................................ 3 II. Scope ........................................................................................................................................... 3 III. Procedures ................................................................................................................................... 3 III.A. Emergency Notification Process ........................................................................................... 3 III.A.1. Emergency Notification Diagram...................................................................................... 5 III.A.2. Emergency Numbers ........................................................................................................ 5 III.B. Categories of Emergencies (Threat Levels) ........................................................................... 6 III.B.1. Threat Level 1 .................................................................................................................. 7 III.B.2. Threat Level 2 .................................................................................................................. 7 III.B.3. Threat Level 3 .................................................................................................................. 7 III.C. Organization........................................................................................................................ -

Model SOP Standard Operating Procedure
Model SOP for Training Purposes Only Firetactics.com Model SOP Standard Operating Procedure Firetactics.com Paul Grimwood FIFireE ‐ SOP 1/Version 2/2009 1. TACTICAL DEPLOYMENT INTO FIRE INVOLVED STRUCTURES Sections 1. Purpose 1. Purpose The following bulletin serves as a training 2. Pre‐planning document that covers a range of critical 3. Information ‘in’ tasking issues associated with the safe 4. Risk Management and effective deployment of firefighters 5. Information ‘out’ into fire involved structures. It is not a 6. Situation Awareness complete SOP by any means but simply 7. Staffing stands to inform of a risk‐assessed 8. Water Supply process for compartment and structural 9. Primary Attack fire‐fighting. 10. Search & Rescue However, this document may serve as a 11. Securing Team Safety model upon which more detailed 12. Tactical Ventilation operational procedures may be 13. Primary (First Response) Command & Control developed. 14. Accountability 15. BA Emergency Procedure All students are strongly advised to follow 16. Communication their own departmental SOPs at all times. 17. Principal Officer (First Chief) Command & Control Any deviation from such procedure must 18. Large Volume Structures only be made with good reason and 19. High‐rise Buildings should be held accountable at a later stage. 20. The Most Common Reasons for Traumatic Fire‐fighter Life Losses 2. Pre‐planning It is essential that familiarization visits are made to all large volume structures, or those presenting excessive or unusual risks, so that plans may are organised and provided on‐site in special premises information boxes located at main entry points. Alternatively, these may be held on computer terminals and down loaded into a fire engine’s computer system as they arrive on‐scene. -

POCATELLO FIRE/EMERGENCY PROCEDURE Updated 05/01/18 1
IDAHO STATE VETERANS HOME – POCATELLO FIRE/EMERGENCY PROCEDURE Table of Contents GENERAL STATEMENT ........................................................................................................... 3 GENERAL EMERGENCY INFORMATION ........................................................................... 3 FIRE (Code Red) ...................................................................................................................... 4 FIRE PROCEDURE................................................................................................................. 4 FIRE ALARM (FIRE) PROCEDURES FOR ALL PERSONNEL ..................................... 5 IN CASE OF A FALSE ALARM: ........................................................................................... 5 FIRE AND SAFETY PLAN FOR FOOD SERVICE ............................................................ 5 FIRE SAFETY PLAN FOR NURSING CARE UNIT .......................................................... 6 DAY SHIFT ....................................................................................................................... 6 P.M. SHIFT: ....................................................................................................................... 6 NIGHT SHIFT: ................................................................................................................... 6 DINING ROOM--ALTERNATE FIRE/SAFETY PLAN ..................................................... 7 DAY SHIFT: ..................................................................................................................... -

Emergency Management Planning
A Sample Fire Safety Plan…3 Hospital Planning Considerations…4 Aging Services Facility Planning Considerations…7 Emergency Management Self-assessment Checklist…10 Resources…12 REPUBLISHED 2013 Emergency Management Planning: Assessing the Risks, Preparing for Recovery Hurricane Sandy in October 2012 incapacitated four New York those organizations that have invested sufficient effort in recovery City hospitals (including Bellevue Hospital, the city’s major public planning will be better able not only to minimize losses and costly trauma center), disrupting the city’s healthcare delivery system. interruptions, but also to provide essential emergency services for Similarly, the massive tornado that flattened much of Joplin, their community. (For more detailed information about continuity Missouri in May 2011 destroyed one of the town’s two hospitals, and insurance considerations, see “What’s So Important About killing several patients and staff – exactly when the local populace Business Interruption Coverage?,” a CNA risk management bulletin.* was most in need of emergency care. The two disasters served Brokers are another important source of information about busi- as a grim reminder of nature’s ability to inflict catastrophic loss on ness interruption risks and strategies.) healthcare facilities of every description, from large systems to This CNA resource presents general strategies and safety meas- small specialty providers. ures to help identify disaster-related risks and potential losses, Hurricane Sandy and the Joplin tornado also demonstrate why all protect patients/residents and staff from danger, and minimize organizations need a workable, detailed, enterprise-wide emergency disruption to both clinical practice and business operations. Side- management plan addressing both natural and man-made crises. -

Handbook on Emergency Procedures
International Committee on Museum Security HANDBOOK ON EMERGENCY PROCEDURES Developed by members of the ICMS With the financial support of: ICOM Ministry of Culture of The Netherlands Rijksmuseum Amsterdam (The Netherlands) Van Gogh Museum (The Netherlands) Mondriaan Foundation (The Netherlands) ICMS Editor: Willem Hekman (The Netherlands) October 2010 Content Introduction 4 Chapter 1 : Risk analysis 5 Chapter 2 : Vandalism 8 Chapter 3 : Theft 11 Chapter 4 : Fire 15 Chapter 5 : Floods 20 Chapter 6 : Chemical spills 26 Chapter 7 : Earthquake 30 Chapter 8 : Terrorism 35 Chapter 9 : Museums under threat of bomb and rocket attacks and war 42 Chapter 10: Building facility risks 47 2 http://icom.museum ICOM in short Created in 1946, ICOM (International Council of Museums) is an international non- governmental organization maintaining formal relations with UNESCO and having a consultative status with the United Nations' Economic and Social Council. ICOM is the only international organisation representing museums and museum professionals. ICOM is: • A diplomatic forum made up of representatives from 137 countries and territories • Standards of excellence for museums including ethics (Code of ethics for museums) • An international network composed of 30,000 museum professionals around the world • A think-tank composed by 31 International Committees which represent ICOM’s specialities • Missions of international public service notably in the fight against illicit traffic and emergency programmes in case of natural disasters or armed conflicts 3 -

Risk Management Manual 2020
Risk Management Manual 2020 “Creating Proactive Solutions to Empower and Protect” This page intentionally left blank Your Safety Matters Hi Everyone, I’m confident you know this — and it’s worth repeating: The City of Hillsboro is committed to providing a safe and healthful work environment for all employees. How do we walk our talk? Our Human Resources Department’s Risk Management Division… leads a Safety and Loss Control Program to prevent accidents by identifying hazards and training employees. Each City department… is responsible for providing and maintaining safe equipment and materials, and for ensuring employees are trained to perform their jobs safely. Risk Management staff help departments to develop and implement rules and operational procedures to ensure safe operations. Each City employee… must follow established rules and procedures, and report unsafe conditions and accidents to their supervisor. Supervisors then relay that information to assure that appropriate corrections are made. The City’s Safety Committees… play a significant role in workplace safety. Department managers and staff participate on and support the work of the committees. Maintaining a safe work environment requires your commitment, constant attention, and continual effort. Risk Management staff are available to assist you and your department. When you are healthy, injury‐free, and safe, your quality of life and your ability to perform well at work significantly increases. Let’s work together to achieve this. Robby Hammond City Manager P.S. Have fun at work. Just do it safely. This page intentionally left blank Table of Contents RISK MANAGEMENT Risk Management Overview ....................................................................................... 1 INSURANCE AND CLAIMS Insurance Program ..................................................................................................... -
Accomack County Fire Rescue Commission Standard Operating Guidelines
Accomack County Fire Rescue Commission Standard Operating Guidelines Subject: Responder Emergency Guidelines Section: Countywide Guideline Number: 101 Effective Date: August 1, 2013 - Updated May 1, 2014 Signature of Approval Jeffrey T. Terwilliger Fire Commission Chairperson PURPOSE: To establish standard operating guidelines (SOGs) regarding safety procedures for the Incident Commander (IC), responders and dispatch center to take when; a responder emergency occurs, a MayDay alert occurs, emergency traffic message is declared, emergency alert tone is sounded, and the establishment of rapid intervention crews. To establish procedures to enable responders to notify or be notified of an emergency condition or situation when they are assigned to an immediately dangerous to life or health (IDLH) environment. To establish procedures for emergency situations outside of an IDLH zone, and or an individual operating on an incident needing law enforcement or other assistance when faced with a physical threat to their safety or others on an incident scene. SCOPE: Applicable to all; fire, rescue, EMS responders and assisting and cooperating agencies involved with emergency fire and rescues operations in Accomack County, Virginia. GUIDELINES Purpose, Scope and Definitions 101 Pages: 1-3 Emergency Alert tone 101.1 Pages: 4,5 Emergency Traffic 101.2 Page: 6 Signal (1) 101.3 Pages: 7,8 MayDay 101.4 Pages: 9-13 Evacuation Orders 101.5 Page: 14 Rapid Intervention Crew 101.6 Pages: 15-18 Intent of the Responder Emergency Procedure Guidelines: 1. The communications system shall provide a standard method to give priority to the transmission of emergency messages and notification of imminent hazards over that of routine communications to all levels of the incident command structure. -
Production Services Standard Operating Procedure (S.O.P.)
Production Services Standard Operating Procedure (S.O.P.) Department: Production Services Title: Venue Related Emergency Procedure Supervisor: Event Services Manager Date: 10/21/15 Manager: Event Coordinators Space: All performance venues This Standard Operating Procedure for the Production Services Department of the Clarice Smith Performing Arts Center is designed to create safe and efficient work practice for all staff members, departments, students, residence artists and related personnel. Please see the Manager of the Standard Operating Procedure for any additional questions. Definitions Performance: The period of time in which public audience members are present in a performance venue to see a scheduled event. Emergency: An unexpected, and sometimes dangerous situation that requires the immediate attention and may be beyond the control or ability of the individuals involved. Standard Procedure I. Stopping a Performance/Evacuating the Venue a. The stage manager and house manager will work together on effectively communicating needs within the venue. i. The venue is the primary responsibility of the stage manager for the duration of the performance with the exception of the period of time immediately preceding and following as well as any intermissions when the primary responsibility falls to the house manager, however it is imperative that during all times the house manager and stage manager work together closely to manage the safety and experience of the patrons, performers and staff. ii. The “turning over of the house” from one party to another will occur via radio for each of these instances. b. If a circumstance arises during a performance the affects the performers, audience or venue, the stage manager and house manager (with input from their onsite supervisors) will decide the most effective way to proceed.