Memory Systems
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Semantic Memory - Psychology - Oxford Bibliographies
1/16/2019 Semantic Memory - Psychology - Oxford Bibliographies Semantic Memory Michael N. Jones, Johnathan Avery LAST MODIFIED: 15 JANUARY 2019 DOI: 10.1093/OBO/97801998283400231 Introduction Semantic memory refers to our general world knowledge that encompasses memory for concepts, facts, and the meanings of words and other symbolic units that constitute formal communication systems such as language or math. In the classic hierarchical view of memory, declarative memory was subdivided into two independent modules: episodic memory, which is our autobiographical store of individual events, and semantic memory, which is our general store of abstracted knowledge. However, more recent theoretical accounts have greatly reduced the independence of these two memory systems, and episodic memory is typically viewed as a gateway to semantic memory accessed through the process of abstraction. Modern accounts view semantic memory as deeply rooted in sensorimotor experience, abstracted across many episodic memories to highlight the stable characteristics and mute the idiosyncratic ones. A great deal of research in neuroscience has focused on both how the brain creates semantic memories and what brain regions share the responsibility for storage and retrieval of semantic knowledge. These include many classic experiments that studied the behavior of individuals with brain damage and various types of semantic disorders but also more modern studies that employ neuroimaging techniques to study how the brain creates and stores semantic memories. Classically, semantic memory had been treated as a miscellaneous area of study for anything in declarative memory that was not clearly within the realm of episodic memory, and formal models of meaning in memory did not advance at the pace of models of episodic memory. -

Compare and Contrast Two Models Or Theories of One Cognitive Process with Reference to Research Studies
! The following sample is for the learning objective: Compare and contrast two models or theories of one cognitive process with reference to research studies. What is the question asking for? * A clear outline of two models of one cognitive process. The cognitive process may be memory, perception, decision-making, language or thinking. * Research is used to support the models as described. The research does not need to be outlined in a lot of detail, but underatanding of the role of research in supporting the models should be apparent.. * Both similarities and differences of the two models should be clearly outlined. Sample response The theory of memory is studied scientifically and several models have been developed to help The cognitive process describe and potentially explain how memory works. Two models that attempt to describe how (memory) and two models are memory works are the Multi-Store Model of Memory, developed by Atkinson & Shiffrin (1968), clearly identified. and the Working Memory Model of Memory, developed by Baddeley & Hitch (1974). The Multi-store model model explains that all memory is taken in through our senses; this is called sensory input. This information is enters our sensory memory, where if it is attended to, it will pass to short-term memory. If not attention is paid to it, it is displaced. Short-term memory Research. is limited in duration and capacity. According to Miller, STM can hold only 7 plus or minus 2 pieces of information. Short-term memory memory lasts for six to twelve seconds. When information in the short-term memory is rehearsed, it enters the long-term memory store in a process called “encoding.” When we recall information, it is retrieved from LTM and moved A satisfactory description of back into STM. -

Dissociation Between Declarative and Procedural Mechanisms in Long-Term Memory
! DISSOCIATION BETWEEN DECLARATIVE AND PROCEDURAL MECHANISMS IN LONG-TERM MEMORY A dissertation submitted to the Kent State University College of Education, Health, and Human Services in partial fulfillment of the requirements for the degree of Doctor of Philosophy By Dale A. Hirsch August, 2017 ! A dissertation written by Dale A. Hirsch B.A., Cleveland State University, 2010 M.A., Cleveland State University, 2013 Ph.D., Kent State University, 2017 Approved by _________________________, Director, Doctoral Dissertation Committee Bradley Morris _________________________, Member, Doctoral Dissertation Committee Christopher Was _________________________, Member, Doctoral Dissertation Committee Karrie Godwin Accepted by _________________________, Director, School of Lifespan Development and Mary Dellmann-Jenkins Educational Sciences _________________________, Dean, College of Education, Health and Human James C. Hannon Services ! ""! ! HIRSCH, DALE A., Ph.D., August 2017 Educational Psychology DISSOCIATION BETWEEN DECLARATIVE AND PROCEDURAL MECHANISMS IN LONG-TERM MEMORY (66 pp.) Director of Dissertation: Bradley Morris The purpose of this study was to investigate the potential dissociation between declarative and procedural elements in long-term memory for a facilitation of procedural memory (FPM) paradigm. FPM coupled with a directed forgetting (DF) manipulation was utilized to highlight the dissociation. Three experiments were conducted to that end. All three experiments resulted in facilitation for categorization operations. Experiments one and two additionally found relatively poor recognition for items that participants were told to forget despite the fact that relevant categorization operations were facilitated. Experiment three resulted in similarly poor recognition for category names that participants were told to forget. Taken together, the three experiments in this investigation demonstrate a clear dissociation between the procedural and declarative elements of the FPM task. -

The Integrated Nature of Metamemory and Memory
The Integrated Nature of Metamemory and Memory John Dunlosky and Robert A. Bjork Introduction Memory has been of interest to scholars and laypeople alike for over 2,000 years. In a rather gruesome example from antiquity, Cicero tells the story of Simonides (557– 468 BC), who discovered the method of loci, which is a powerful mental mnemonic for enhancing one’s memory. Simonides was at a banquet of a nobleman, Scopas. To honor him, Simonides sang a poem, but to Scopas’s chagrin, the poem also honored two young men, Castor and Pollux. Being upset, Scopas told Simonides that he was to receive only half his wage. Simonides was later called from the banquet, and legend has it that the banquet room collapsed, and all those inside were crushed. To help bereaved families identify the victims, Simonides reportedly was able to name every- one according to the place where they sat at the table, which gave him the idea that order brings strength to our memories and that to employ this ability people “should choose localities, then form mental images of things they wanted to store in their memory, and place these in the localities” (Cicero, 2001). Tis example highlights an early discovery that has had important applied impli- cations for improving the functioning of memory (see, e.g., Yates, 1997). Memory theory was soon to follow. Aristotle (385–322 BC) claimed that memory arises from three processes: Events are associated (1) through their relative similarity or (2) rela- tive dissimilarity and (3) when they co-occur together in space and time. -

Working Memory and Cued Recall Max V
Georgia Southern University Digital Commons@Georgia Southern University Honors Program Theses 2016 Working memory and cued recall Max V. Fey 8602950 Karen Naufel Georgia Southern University Lawrence Locker Georgia Southern University Follow this and additional works at: https://digitalcommons.georgiasouthern.edu/honors-theses Part of the Cognitive Psychology Commons Recommended Citation Fey, Max V. 8602950; Naufel, Karen; and Locker, Lawrence, "Working memory and cued recall" (2016). University Honors Program Theses. 220. https://digitalcommons.georgiasouthern.edu/honors-theses/220 This thesis (open access) is brought to you for free and open access by Digital Commons@Georgia Southern. It has been accepted for inclusion in University Honors Program Theses by an authorized administrator of Digital Commons@Georgia Southern. For more information, please contact [email protected]. 1 Working Memory and Cued Recall Working Memory and Cued Recall An Honors Thesis submitted in partial fulfillment of the requirements for Honors in the Department of Psychology. By Maximilian Fey Under the mentorship of Dr. Karen Naufel ABSTRACT Previous research has found that individuals with high working memory have greater recall capabilities than those with low working memory (Unsworth, Spiller, & Brewers, 2012). Research did not test the extent to which cues affect one’s recall ability in relation to working memory. The present study will examine this issue. Participants completed a working memory measure. Then, they were provided with cued recall tasks whereby they recalled Facebook friends. The cues varied to be no cues, ambiguous cues high in imageability, and cues directly related to Facebook. The results showed that there was no difference between individual’s ability to recall their Facebook friends and their working memory scores. -

The Effects of Happy and Sad Emotional States on Episodic Memory
The Effects of Happy and Sad Emotional States on Episodic Memory Richard Topolski ([email protected]) Department of Psychology, Augusta State University 2500 Walton Way, Augusta GA 30904 USA Sarah R. Daniel ([email protected]) Department of Psychology, Augusta State University 2500 Walton Way, Augusta GA 30904 USA Introduction methodology for measuring EM largely independent of semantic memory. Episodic memory (EM) is composed of personally experienced events in which ‘the what, where, and when’ Method are essential components while semantic memory is simply composed of accumulated facts about the world (Tulving, Happy, neutral, or sad mood states were induced in 88 2002). A wide variety of tasks have been used to tap students via a 20 minute long viewing of either a stand-up episodic memory including: recalling words from an early comedy routine, a documentary, or holocaust footage. learned list; yes-no recognition of previously presented Immediately following the mood induction, participants common objects or pictures; and free recall of past personal engaged in eight interactive tasks which involved both experiences. These tasks are used to evaluate episodic familiar objects (pennies and paperclips) and novel memory because in order to know which words, pictures, or geometric forms created by bending paper clips with blue experiences to retrieve, some contextual (episodic) beads into unique shapes, (Rock, Schreilber, and Ro, 1994). information must first be accessed (Mayes & Roberts, A four-item force-choice recognition test for the novel 2001). While all of these measures seem to share this geometric forms was employed, with the task name serving contextual component, none adequately examines the as the retrieval cue. -

Handbook of Metamemory and Memory Evolution of Metacognition
This article was downloaded by: 10.3.98.104 On: 29 Sep 2021 Access details: subscription number Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: 5 Howick Place, London SW1P 1WG, UK Handbook of Metamemory and Memory John Dunlosky, Robert A. Bjork Evolution of Metacognition Publication details https://www.routledgehandbooks.com/doi/10.4324/9780203805503.ch3 Janet Metcalfe Published online on: 28 May 2008 How to cite :- Janet Metcalfe. 28 May 2008, Evolution of Metacognition from: Handbook of Metamemory and Memory Routledge Accessed on: 29 Sep 2021 https://www.routledgehandbooks.com/doi/10.4324/9780203805503.ch3 PLEASE SCROLL DOWN FOR DOCUMENT Full terms and conditions of use: https://www.routledgehandbooks.com/legal-notices/terms This Document PDF may be used for research, teaching and private study purposes. Any substantial or systematic reproductions, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The publisher shall not be liable for an loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material. Evolution of Metacognition Janet Metcalfe Introduction The importance of metacognition, in the evolution of human consciousness, has been emphasized by thinkers going back hundreds of years. While it is clear that people have metacognition, even when it is strictly defined as it is here, whether any other animals share this capability is the topic of this chapter. -
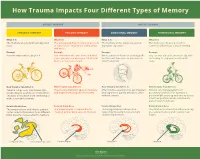
How Trauma Impacts Four Different Types of Memory
How Trauma Impacts Four Different Types of Memory EXPLICIT MEMORY IMPLICIT MEMORY SEMANTIC MEMORY EPISODIC MEMORY EMOTIONAL MEMORY PROCEDURAL MEMORY What It Is What It Is What It Is What It Is The memory of general knowledge and The autobiographical memory of an event The memory of the emotions you felt The memory of how to perform a facts. or experience – including the who, what, during an experience. common task without actively thinking and where. Example Example Example Example You remember what a bicycle is. You remember who was there and what When a wave of shame or anxiety grabs You can ride a bicycle automatically, with- street you were on when you fell off your you the next time you see your bicycle out having to stop and recall how it’s bicycle in front of a crowd. after the big fall. done. How Trauma Can Affect It How Trauma Can Affect It How Trauma Can Affect It How Trauma Can Affect It Trauma can prevent information (like Trauma can shutdown episodic memory After trauma, a person may get triggered Trauma can change patterns of words, images, sounds, etc.) from differ- and fragment the sequence of events. and experience painful emotions, often procedural memory. For example, a ent parts of the brain from combining to without context. person might tense up and unconsciously make a semantic memory. alter their posture, which could lead to pain or even numbness. Related Brain Area Related Brain Area Related Brain Area Related Brain Area The temporal lobe and inferior parietal The hippocampus is responsible for The amygdala plays a key role in The striatum is associated with producing cortex collect information from different creating and recalling episodic memory. -

Spared Face Recognition in Amnesia Is Based on Familiarity
Neuropsychologia 48 (2010) 3941–3948 Contents lists available at ScienceDirect Neuropsychologia journal homepage: www.elsevier.com/locate/neuropsychologia Faces are special but not too special: Spared face recognition in amnesia is based on familiarity Mariam Aly a,∗, Robert T. Knight b, Andrew P. Yonelinas a a University of California, Department of Psychology, 134 Young Hall, One Shields Avenue, Davis, CA 95616, United States b University of California, Department of Psychology and Helen Wills Neuroscience Institute, 3210 Tolman Hall, Berkeley, CA 94720, United States article info abstract Article history: Most current theories of human memory are material-general in the sense that they assume that the Received 10 June 2010 medial temporal lobe (MTL) is important for retrieving the details of prior events, regardless of the spe- Received in revised form 30 August 2010 cific type of materials. Recent studies of amnesia have challenged the material-general assumption by Accepted 2 September 2010 suggesting that the MTL may be necessary for remembering words, but is not involved in remember- Available online 15 September 2010 ing faces. We examined recognition memory for faces and words in a group of amnesic patients, which included hypoxic patients and patients with extensive left or right MTL lesions. Recognition confidence Keywords: judgments were used to plot receiver operating characteristics (ROCs) in order to more fully quantify Episodic memory Recollection recognition performance and to estimate the contributions of recollection and familiarity. Consistent Familiarity with the extant literature, an analysis of overall recognition accuracy showed that the patients were Amnesia impaired at word memory but had spared face memory. -

Episodic Memory-From Brain to Mind
HIPPOCAMPUS 16:691–703 (2006) Episodic Memory—From Brain to Mind Janina Ferbinteanu,* Pamela J. Kennedy, and Matthew L. Shapiro ABSTRACT: Neuronal mechanisms of episodic memory, the conscious by the rapid formation of relational representations of recollection of autobiographical events, are largely unknown because highly processed sensory information that are used electrophysiological studies in humans are conducted only in excep- tional circumstances. Unit recording studies in animals are thus crucial flexibly and are not necessarily expressed through overt for understanding the neurophysiological substrate that enables people motor behavior. Episodic memory is also sensitive to to remember their individual past. Two features of episodic memory— lesions of the prefrontal cortex (Wheeler et al., 1995; autonoetic consciousness, the self-aware ability to \travel through Nyberg et al., 2000; Burgess et al., 2002; Wheeler time", and one-trial learning, the acquisition of information in one and Stuss, 2003), develops later in an individual’s life, occurrence of the event—raise important questions about the validity of animal models and the ability of unit recording studies to capture essen- encodes events within a personal framework, and pos- tial aspects of memory for episodes. We argue that autonoetic experi- sesses a temporal dimension because it is oriented ence is a feature of human consciousness rather than an obligatory as- towards the past and the future (Tulving, 1972, 2001, pect of memory for episodes, and that episodic memory is reconstruc- 2002; Tulving and Markowitsch, 1998). Autobio- tive and thus its key features can be modeled in animal behavioral tasks graphic information contains memories about what that do not involve either autonoetic consciousness or one-trial learning. -

Dissociating Recollection and Familiarity Processes Using Rtms
Behavioural Neurology 19 (2008) 23–27 23 IOS Press Recognition memory and prefrontal cortex: Dissociating recollection and familiarity processes using rTMS Patrizia Turriziania,b,∗, Massimiliano Oliveria,b, Silvia Salernoa, Floriana Costanzoa, Giacomo Kochb,c, Carlo Caltagironeb,c and Giovanni Augusto Carlesimob,c aDipartimento di Psicologia, Universita` di Palermo, Palermo, Italy bIRCCS Fondazione Santa Lucia, Roma, Italy cClinica Neurologica, Universita` di Roma Tor Vergata, Roma, Italy Abstract. Recognition memory can be supported by both the assessment of the familiarity of an item and by the recollection of the context in which an item was encountered. The neural substrates of these memory processes are controversial. To address these issues we applied repetitive transcranial magnetic stimulation (rTMS) over the right and left dorsolateral prefrontal cortex (DLPFC) of healthy subjects performing a remember/know task. rTMS disrupted familiarity judgments when applied before encoding of stimuli over both right and left DLPFC. rTMS disrupted recollection when applied before encoding of stimuli over the right DLPFC. These findings suggest that the DLPFC plays a critical role in recognition memory based on familiarity as well as recollection. Keywords: Recognition memory, recollection, familiarity, prefrontal cortex 1. Introduction An alternative view is that distinct medial temporal regions differentially contribute to familiarity and rec- Recognition memory can be based on the recollec- ollection, whereas the prefrontal cortex supports both tion of specific information associated with a previous these processes [1,18]. This idea draws support from episode and on the assessment of the familiarity of an some neuropsychological [4,5], neuroimaging [2,7,12, item [18]. However, it remains unclear whether these 20] and electrophysiological[3,6,16] studies in humans two forms of memory reflect distinct processes at a and from single-unit studies in monkeys [17] that link neural level. -
PSYC20006 Notes
PSYC20006 BIOLOGICAL PSYCHOLOGY PSYC20006 1 COGNITIVE THEORIES OF MEMORY Procedural Memory: The storage of skills & procedures, key in motor performance. It involves memory systems that are independent of the hippocampal formation, in particular, the cerebellum, basal ganglia, cortical motor sites. Doesn't involve mesial-temporal function, basal forebrain or diencephalon. Declarative memory: Accumulation of facts/data from learning experiences. • Associated with encoding & maintaining information, which comes from higher systems in the brain that have processed the information • Information is then passed to hippocampal formation, which does the encoding for elaboration & retention. Hippocampus is in charge of structuring our memories in a relational way so everything relating to the same topic is organized within the same network. This is also how memories are retrieved. Activation of 1 piece of information will link up the whole network of related pieces of information. Memories are placed into an already exiting framework, and so memory activation can be independent of the environment. MODELS OF MEMORY Serial models of Memory include the Atkinson-Shiffrin Model, Levels of Processing Model & Tulving’s Model — all suggest that memory is processed in a sequential way. A parallel model of memory, the Parallel Distributed Processing Model, is one which suggests types of memories are processed independently. Atkinson-Shiffrin Model First starts as Sensory Memory (visual / auditory). If nothing is done with it, fades very quickly but if you pay attention to it, it will move into working memory. Working Memory contains both new information & from long-term memory. If it goes through an encoding process, it will be in long-term memory.