Ev27n3p287.Pdf (892.5Kb)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Life and Death of Smallpox Ian and Jenifer Glynn Frontmatter More Information
Cambridge University Press 0521845424 - The Life and Death of Smallpox Ian and Jenifer Glynn Frontmatter More information The Life and Death of Smallpox This is an engaging and fascinating story of a conditional human success story. Smallpox has been one of the most devastating scourges of humanity throughout recorded history, and it is the only human illness to have been eradicated, though polio may soon follow it to official extinction through human agency. However, while smallpox is officially extinct in nature, our fears that stocks of smallpox virus may return as a weapon of bioterrorists have led to the stockpiling of vaccine, and continuing vigilance, even though the official victory over smallpox is now 15 years old. The Life and Death of Smallpox presents the entire engaging history of our struggle and ultimate (?) victory over one of our oldest and worst enemies. The story of the campaign to track down and eradicate the virus, throughout the world – the difficulties, setbacks, and the challenges successfully met – is a highlight of a fascinating book, but we cannot be confident of the ending. The final chapter of the book clearly and authoritatively explains the current status of the threat from the deliberate release of smallpox or other potential agents of biological terrorism. Ian Glynn is Professor Emeritus of Physiology at Cambridge University and Fellow of Trinity College. He is the author of An Anatomy of Thought (1999). Jenifer Glynn is a Cambridge historian and author of Tidings From Zion (2000). © Cambridge University Press www.cambridge.org Cambridge University Press 0521845424 - The Life and Death of Smallpox Ian and Jenifer Glynn Frontmatter More information The Life and Death of Smallpox IAN AND JENIFER GLYNN © Cambridge University Press www.cambridge.org Cambridge University Press 0521845424 - The Life and Death of Smallpox Ian and Jenifer Glynn Frontmatter More information PUBLISHED BY CAMBRIDGE UNIVERSITY PRESS 40 We s t 20th Street, New York, NY 10011-4211, USA http://www.cambridge.org c Ian and Jenifer Glynn 2004 This book is in copyright. -
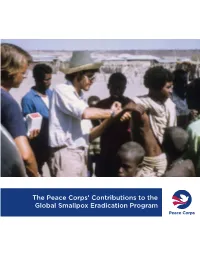
The Peace Corps' Contributions to the Global Smallpox Eradication Program
The Peace Corps’ Contributions to the Global Smallpox Eradication Program About the Office of Strategic Information, Research, and Planning (OSIRP) It is the mission of OSIRP to advance evidence-based management at the Peace Corps by guiding agency strategic planning; monitoring and evaluating agency-level performance and programs; conducting research to generate new insights in the fields of international development, cultural exchange, and Volunteer service; enhancing the stewardship and governance of agency data; and helping to shape agency engagement on high-level, governmentwide initiatives. Front Cover: Peace Corps Volunteers Robert Steinglass and Doug Arbuckle administering the smallpox vaccine in Mille, Ethiopia, in 1974. Photo: Steinglass, personal collection. ii Dedication This report is dedicated to the memory of Dr. Donald Ainslie “D. A.” Henderson (September 7, 1928—August 19, 2016), a seminal figure in the field of smallpox eradication. The Peace Corps is deeply appreciative of having had the opportunity to correspond with Dr. Henderson about the contributions of Peace Corps Volunteers and returned Volunteers within the context of the global eradication program. His charismatic leadership, tireless energy, and unflagging devotion to this program inspired countless public health workers around the world, including many of the returned Peace Corps Volunteers interviewed for this report. iii Acknowledgments In 1806, approximately 10 years after Dr. Edward Jenner conducted the first documented experiment with smallpox vaccination, laying the foundations of modern medicine, President Thomas Jefferson wrote to the English physician and scientist. Jefferson acknowledged the importance of this discovery, extending “a portion of the tribute of gratitude due to you from the whole human family. -

Worldwide Smallpox Eradication, 1957–67
Med. Hist. (2020), vol. 64(1), pp. 71–93. c The Authors 2019. Published by Cambridge University Press 2019 This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited. doi:10.1017/mdh.2019.77 Re-assessing the Foundations: Worldwide Smallpox Eradication, 1957–67 SANJOY BHATTACHARYA 1* and CARLOS EDUARDO D’AVILA PEREIRA CAMPANI 2 1Centre for Global Health Histories, Department of History, University of York, York YO10 5DD, UK 2Department of Health Sciences, University of York, York YO10 5DD, UK Abstract: An expansive, worldwide smallpox eradication programme (SEP) was announced by the World Health Assembly in 1958, leading this decision-making body to instruct the World Health Organization Headquarters in Geneva to work with WHO regional offices to engage and draw in national governments to ensure success. Tabled by the Soviet Union’s representative and passed by a majority vote by member states, the announcement was subject to intense diplomatic negotiations. This led to the formation, expansion and reshaping of an ambitious and complex campaign that cut across continents and countries. This article examines these inter-twining international, regional and national processes, and challenges long-standing historiographical assumptions about the fight against smallpox only gathering strength from the mid-1960s onwards, after the start of a US-supported programme in western Africa. The evidence presented here suggests a far more complex picture. It shows that although the SEP’s structures grew slowly between 1958 and 1967, a worldwide eradication programme resulted from international negotiations made possible through gains during this period. -

The Smallpox Threat: a Time to Reconsider Global Policy
Biosecurity and Bioterrorism: Biodefense Strategy, Practice, and Science Volume 12, Number 3, 2014 ª Mary Ann Liebert, Inc. DOI: 10.1089/bsp.2014.1509.comm Commentary The Smallpox Threat: A Time to Reconsider Global Policy D. A. Henderson and Isao Arita n May of this year, the 67th World Health Assembly more than 8 to 10 countries have sufficient vaccine to Iwill again debate the question of when the remaining cope with an outbreak. A WHO global emergency reserve, specimens of smallpox virus should be destroyed. Over the recommended 10 years ago, is steadily shrinking. Strategic past 18 years, this has been on the agenda of 5 previous plans for outbreak containment have been little discussed. Assemblies, the last being in 2011. At that time, the dele- At the same time, 2 initiatives have received special at- gates ‘‘affirmed strongly the decisions of previous Health tention and resources: one to develop a vaccine that would Assemblies that the remaining stocks of variola virus should protect without adverse reactions, and one to perfect an- be destroyed.’’1 They asked that the date be decided by the tiviral drugs to treat cases should they occur. Both have 2014 Assembly. failed to meet expectations. Inordinate amounts of time, effort, and resources have In writing this commentary, we have jointly drawn on been spent in endeavoring to reach consensus on this one our own half-century of experience with smallpox to offer a component of a smallpox threat strategy: whether to de- brief historic context for a better comprehension of current stroy or not destroy smallpox virus strains now being efforts and to critique the contemporary status of pre- retained in the 2 World Health Organization (WHO) paredness and response in coping with the unlikely return Collaborating Laboratories (in the United States and of smallpox, which has played such a dominant role Russia). -

WHO Advisory Committee on Variola Virus Research
WHO/HSE/GAR/BDP/2009.3 WHO Advisory Committee on Variola Virus Research Report of the Eleventh Meeting Geneva, Switzerland 4–5 November 2009 GLOBAL ALERT AND RESPONSE © World Health Organization 2009 All rights reserved. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distin- guished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall theWorld Health Organization be liable for damages arising from its use. This publication contains the collective views of an international group of experts and does not necessarily represent the decisions or the policies of the World Health Organization. Printed by the WHO Document Production Services, Geneva, Switzerland WHO Advisory Committee on Variola Virus Research Report of the Eleventh Meeting, Geneva, Switzerland, 4–5 November 2009 Executive summary The major accomplishments in the WHO variola virus programme were as follows: WHO smallpox vaccine e mergency stockpile of 32.6 m illion doses was established, well in excess of the original target of five million. -

Seventh Meeting of the WHO/SEAR EPI Technical Consultative Group on Polio Eradication and Vaccine- Preventable Diseases
SEA-Polio-22 Distribution: General Seventh Meeting of the WHO/SEAR EPI Technical Consultative Group on Polio Eradication and Vaccine- Preventable Diseases Conclusions and Recommendations Calcutta, India, 24 - 26 August 2000 WHO Project: ICP VAB 200 World Health Organization Regional Office for South-East Asia New Delhi November 2000 © Word Health Organization (2000) This document is not a formal publication of the World Health Organization (WHO), and all rights are reserved by the Organization. The document may, however, by freely reviewed, abstracted, reproduced or translated, in part or in whole, but not for sale or for use in conjunction with commercial purposes. The views expressed in documents by named authors are solely the responsibility of those authors. CONTENTS Page 1. INTRODUCTION...........................................................................................1 2. GENERAL SUMMARY.....................................................................................1 3. POLIOMYELITIS ERADICATION .....................................................................2 3.1 Surveillance for Detection of Wild Polioviruses........................................5 3.2 Supplementary Immunization.................................................................7 4. ENSURING VACCINE SUPPLY AND QUALITY ..............................................11 5. ROUTINE IMMUNIZATION .........................................................................12 6. WILD POLIOVIRUS LABORATORY CONTAINMENT.....................................13 7. -
Reflections, Frank Fenner
327 Chapter 18. Reflections, Frank Fenner In this final chapter, I want to reflect on two matters, one that spanned my working life, namely special friendships, and the other an analysis of the relative importance of nature, nurture and chance, as they affected my father and myself. Special Friends Friendships are an important element in everyone©s life. Lifelong friendship with one©s wife is the most important and one that I enjoyed in full measure, but I have had many other friends. Here I want to acknowledge the debt I owe to several special friends who have been important to me at various periods of my life, many of who still are. I mention a number of them at some length in the ©boxes© in earlier chapters; those who were close personal friends were Ted Ford, Cecil Hackett, Francis Ratcliffe, Ian Marshall, Gwen Woodroofe, D. A. Henderson and Isao Arita. Two of my mentors, Macfarlane Burnet and René Dubos, were also close friends. Here I will list some other friends chronologically and alphabetically and provide a few comments on each of them. School Days The one person who I remember as a special friend from primary school days is John Dowie, a noted sculptor and painter who still lives in the same house as he did in the 1920s. I greatly enjoyed visiting him in his house and studio, with my sister Winn and my brother Bill, as recently as April 2005. The one person I remember from Thebarton Technical High School is Alf Chittoch, who I met again when I visited Tennant Creek in 1968, where he has lived since the war and risen from being a `battler' in the mines to Mayor. -

The Poliovirus Was Belatedly Produced When the Child Found Itself Unprotected by the Immunity Provided by Breast Feeding
HYGIEA INTERNATIONALIS An Interdisciplinary Journal for the History of Public Health Volume 11, No. 1, 2015 ISSN, Print: 1403-8668; Electronic: 1404-4013 URL: http://www.ep.liu.se/ej/hygiea/ Editorial Board Giovanni Berlinguer, University of Rome “La Sapienza”, Italy Virginia Berridge, London School of Hygiene and Tropical Medicine, U.K. Patrice Bourdelais, École des Hautes Études en Sciences Sociales, France Linda Bryder, University of Auckland, New Zealand Marcos Cueto, Instituto de Estudios Peruanos, Peru Christopher Hamlin, University of Notre Dame, U.S.A. Robert Jütte, Robert Bosch Stiftung, Germany Øivind Larsen, University of Oslo, Norway Marie C. Nelson, Linköping University, Sweden Dorothy E. Porter, University of California, U.S.A. Günter B. Risse, University of California, U.S.A. Esteban Rodriguez-Ocaña, University of Granada, Spain John Rogers, Uppsala University, Sweden Jan Sundin, Linköping University, Sweden Lars-Göran Tedebrand, Umeå University, Sweden John H. Woodward, The University of Sheffield, U.K. Editorial Committee Laurinda Abreu, Patrice Bourdelais, Jan Sundin and Sam Willner Copyright This journal is published under the auspices of Linköping University Electronic Press. All Authors retain the copyright of their articles. © The Authors Table of Contents Volume 11, No. 1, 2015 Sam Willner Foreword 5 Juan Antonio Rodriguez Introduction (Guest Editor) 7 Adrian Carbonetti, Poliomyelitis in the city of Córdoba: Lila Aizenberg Morbidity, knowledge and the research Marina Laura Rodriguez performed by a medical elite -

Nature, Nurture and Chance: the Lives of Frank
Nature, Nurture and Chance THE LIVES OF FRANK AND CHARLES FENNER Nature, Nurture and Chance THE LIVES OF FRANK AND CHARLES FENNER FRANK FENNER VISITING FELLOW, JOHN CURTIN SCHOOL OF MEDICAL RESEARCH THE AUSTRALIAN NATIONAL UNIVERSITY Published by ANU E Press The Australian National University Canberra ACT 0200, Australia Email: [email protected] Web: http://epress.anu.edu.au National Library of Australia Cataloguing-in-Publication entry Fenner, Frank, 1914- . Nature, nurture and chance : the lives of Frank and Charles Fenner. ISBN 1 920942 62 9 ISBN 1 920942 63 7 (online) 1. Fenner, Frank, 1914- . 2. Fenner, Charles, 1884-1955. 3. Microbiologists - Australia - Biography. 4. Virologists - Australia - Biography. 5. Geographers - Australia - Biography. 6. Educators - Australia - Biography. I. Title. 579.092 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying or otherwise, without the prior permission of the publisher. Indexed by Frank Fenner. Cover design by Teresa Prowse. Frank Fenner, by Mathew Lynn, 1999, courtesy of the John Curtin School of Medical Research. Charles Fenner, by Ivor Hele, 1935, courtesy of Education Centre, Adelaide. This edition © 2006 ANU E Press iii Table of Contents List of Figures v Preface vii Acknowledgements xiii Acronyms xv Part I. The Life of Frank Fenner Introduction 3 Chapter 1. Childhood, 1914 to 1932 9 Chapter 2. The University Years, 1933 to 1940 21 Chapter 3. The War Years, May 1940 to February 1946 27 Chapter 4. Walter and Eliza Hall Institute, 1946 to 1948; Rockefeller Institute, 1948 to 1949 47 Chapter 5. -

Eradication of Infectious Diseases: Its Concept, Then And
Jpn. J. Infect. Dis., 57, 1-6, 2004 Review Eradication of Infectious Diseases: Its Concept, Then and Now Isao Arita*, John Wickett1 and Miyuki Nakane Agency for Cooperation in International Health, Kumamoto 862-0901, Japan and 1World Health Organization, Geneva, Switzerland (Received December 18, 2003. Accepted January 19, 2004) CONTENTS: 1. Background 5. Discussion 2. Building up the concept of eradication based 5-1. Smallpox on the eradication of smallpox 5-2. Polio 3. Application of smallpox experience to polio 5-3. Measles eradication 5-4. Changing world 4. Application to measles eradication of experience 6. Reconsideration of the concept of eradication gained from the smallpox and polio eradication 7. Conclusion programs SUMMARY: The concept of disease eradication emerged as recently as the mid-20th century. The successful eradication of smallpox resulted in the concept of the extinction of the causative agent in man as well as in the environment, leading to the cessation of all control measures including vaccination. Subsequently, world resources have been invested in global polio eradication and measles eradication in the Western Hemisphere. The former is apparently now at the “end game”, the latter, after successful campaign in the Americas, aims at program development worldwide. However, both endeavors are being challenged by delays in schedules, unexpected technical problems, lack of global coordination, and ever-increasing political unrest. It is proposed that disease eradication be redefined as the extinction of the pathogen in man, not in nature, making for a more flexible approach in the post-eradication period. Smallpox eradication was a rare event. That concept is unrealistic in today’s world. -

Smallpox Eradication and Human Morality in Evolution Isao Arita* National Hospital Organization, Kumamoto Medical Center, Japan
ccines & a V f V a o c l c a i n Arita, J Vaccines Vaccin 2013, 4:4 n a r t u i o o n J Journal of Vaccines & Vaccination DOI: 10.4172/2157-7560.1000188 ISSN: 2157-7560 Review Article Open Access Smallpox Eradication and Human Morality in Evolution Isao Arita* National Hospital Organization, Kumamoto Medical Center, Japan Abstract Successful WHO smallpox eradication is considered to be the unprecedented event in history of human evolution, namely human species’ long struggle with vicious pathogen termed variola or smallpox. The victory resulted from human efforts, firstly recent scientific discovery of vaccine and epidemiological strategy to interrupt the smallpox transmission and secondly the human species’ joint effort to eradicate smallpox despite difference in nationality, race, religions and politics worldwide. In this article, specifically the second elements are discussed in view of Charles Darwin’s struggle for existence and natural selection and his few followers’ opinions that human genome may have an important role in evolution process, for instance, of ethics, morality, as expressed in” Nature via Nurture”: Genes, experience, what makes human. Since the time unmemorable human species suffered considerable tragedy of smallpox disaster, themselves as well as their family and friends without knowing how to escape: Perhaps their ancestors sad memories could have influenced the minds of the staff or villagers, how to contribute themselves for rescuing their fellow human species: Please read and think for the future of human species. Keywords: Smallpox; Human species; Vaccines; Environmental include the social (nature versus nurture) elements that evolved from stress people’s experience dealing with smallpox disasters that occurred since prehistoric time. -
CDC and the Smallpox Crusade
CDC and 'he Smallpox Crusade For riale by the Superintendent of Documents. U.S. Government Printing Office Washington, D.C. 20402 CDC and The Smallpox Crusade Horace G. Ogden U .S Department of Health and HumanServices Public Health Service Centers for Disease Control HHS Publication No. (CDC) 87-8400 Free at last. Recovering from smallpox, Bogra, Bangladesh. 1975. Photo by: Carol F. Music Free at last Rounding the comer of a health clinic bungalow, I gazed deeply into the pain and trust of a beautiful girlchild. She sat on a windowsill, behind bars, recovering from smallpox. A boy patient joined her. My heart winced. 1 felt the nightmare of a youngster’s fever and rash . a person’s struggle with pain and fear . a family’s struggle with separation and loss . a survivor’s struggle with life, indelibly marked and dishonored by the community. 1 experienced anew being a prisoner of one’s own skin in any community. Our eyes embraced. It was January 1975 in Bogra, Bangladesh. She yearned to breathe free. When would that be? For hundreds of years, smallpox had run unleashed among millions of people, keeping nations suppressed and a world held hostage. Yet, persistent advance ments after 1950 showed clear promise of global eradication of the disease; and to this end the World Health Assembly declared, in 1966, a worldwide Small pox Eradication Program, Remarkable leadership and personnel around the world provided crucial, ongo ing skills to augment each endemic nation’s campaign. Families of overseas consultants from the Centers for Disease Control, such as I, had a rare opportu nity to see a portion of the last vestiges of smallpox amidst the rigors of surveil lance and containment in the field.