The INVISIBLE RAINBOW
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Protestant and Catholic Medicine in the Sixteenth Century? the Case of Ingolstadt Anatomy
Medical History, 2001, 45: 83-96 Protestant and Catholic Medicine in the Sixteenth Century? The Case of Ingolstadt Anatomy JURGEN HELM* There is an ongoing debate about the relation between religious confession and sixteenth-century medicine. Although it is generally agreed that Richard Toellner's statement "In Wittenberg the Reformation does not affect the medical faculty", which closes a paper published in 1984,' cannot be maintained in this apodictic formulation, recent research still discusses how and to what extent confessional matters might have influenced sixteenth-century medical thinking. Interest has focused in particular on the "anatomical Renaissance", as Andrew Cunningham's book is entitled,2 which reviewed the works of Andreas Vesalius (1514-1564) and several sixteenth-century anatomists as well as the dissemination of their ideas celebrated by generations ofmedical historians as the beginning ofmodem anatomical research. In his paper on 'Wittenberg anatomy' Vivian Nutton showed in 1994 that a special view of anatomical knowledge was taken at Wittenberg University.3 According to Nutton, Wittenberg anatomy must be considered as an "education process in which a variety of messages was transmitted" to the students.4 Here, at the Leucorea, the heart of Lutheran Reformation, anatomy was focused on its theological implications: it dealt particularly with the links between the body and the Christian soul and hence affected Christian morality. Furthermore, anatomy, the disclosure of the wonderful structure of the human body, was most suitable for demonstrating the Creator's skill in designing nature. Philipp Melanchthon's (1497-1560) Commentarius Jiurgen Helm, Dr med., Martin-Luther- in A Buck (ed.), Renaissance Reformation. -

AMERICAN MANHOOD in the CIVIL WAR ERA a Dissertation Submitted
UNMADE: AMERICAN MANHOOD IN THE CIVIL WAR ERA A Dissertation Submitted to the Graduate School of the University of Notre Dame in Partial Fulfillment of the Requirements for the Degree of Doctor in Philosophy by Michael E. DeGruccio _________________________________ Gail Bederman, Director Graduate Program in History Notre Dame, Indiana July 2007 UNMADE: AMERICAN MANHOOD IN THE CIVIL WAR ERA Abstract by Michael E. DeGruccio This dissertation is ultimately a story about men trying to tell stories about themselves. The central character driving the narrative is a relatively obscure officer, George W. Cole, who gained modest fame in central New York for leading a regiment of black soldiers under the controversial General Benjamin Butler, and, later, for killing his attorney after returning home from the war. By weaving Cole into overlapping micro-narratives about violence between white officers and black troops, hidden war injuries, the personal struggles of fellow officers, the unbounded ambition of his highest commander, Benjamin Butler, and the melancholy life of his wife Mary Barto Cole, this dissertation fleshes out the essence of the emergent myth of self-made manhood and its relationship to the war era. It also provides connective tissue between the top-down war histories of generals and epic battles and the many social histories about the “common soldier” that have been written consciously to push the historiography away from military brass and Lincoln’s administration. Throughout this dissertation, mediating figures like Cole and those who surrounded him—all of lesser ranks like major, colonel, sergeant, or captain—hem together what has previously seemed like the disconnected experiences of the Union military leaders, and lowly privates in the field, especially African American troops. -

Reformation Roots Edited by John B
THE LIVING THEOLOGICAL HERITAGE OF THE UNITED CHURCH OF CHRIST Barbara Brown Zikmund Series Editor L T H VOLUME TWO Reformation Roots Edited by John B. Payne The Pilgrim Press Cleveland, Ohio Contents The Living Theological Heritage of the United Church of Christ ix Reformation Roots 1 Part L Late Medieval and Renaissance Piety and Theology 37 1. The Book of the Craft of Dying (c. mid-15th century) 37 2. The Imitation of Christ (c. 1427) 51 THOMAS À KEMPIS 3. Eternal Predestination and Its Execution in Time (1517) 69 JOHN VON STAUPITZ 4.Paraclesis(1516) 86 DESIDERIUS ERASMUS Part II. Reformation in Germany, Switzerland, and the 98 Netherlands Martin Luther and the German Reformation 5. The Freedom of a Christian (1520) 98 MARTIN LUTHER 6. Formula of Mass and Communion for the Church 121 at Wittenberg (1523) MARTIN LUTHER 7. Hymn: Out of the Depths I Cry to Thee (1523) 137 MARTIN LUTHER 8. Small Catechism (1529) 140 MARTIN LUTHER 9. The Augsburg Confession (1530) 160 Zwingli and the Swiss Reformation 10. Sixty-Seven Articles (1523) 196 ULRICH ZWINGLI 11. Action or Use of the Lord's Supper (1525) 205 ULRICH ZWINGLI 12. The Schleitheim Confession of Faith (1527) 214 13. The Marburg Colloquy (1529) 224 VI • CONTENTS 14. Sermon One, Decade One: Of the Word of God 248 from Decades (1549-51) HEINRICH BULLINGER Calvin and the Genevan Reformation 15. The Law from Institution of the Christian Religion (1536) 266 JOHN CALVIN 16. The Geneva Confession (1536) 272 WILLIAM FAREL AND JOHN CALVIN 17. The Strasbourg Liturgy (1539) 280 MARTIN BUCER 18. -

The Woman's Medical College of Pennsylvania : an Historical Outline
WDMAN^S MEDICAL :eDtl;EGI OF PENNSYimNll^^ N,lll||»|,;,l,|l4^,.^, William ©Ecamaxx. Jr. /a1> - Purrha'^«>d for the University of Toronto Library from funds donated by Hannah Institute for the History of Medicine ^^-^^^-^^'Z^ i^^j=-<^^^^.^4^^ THE Woman's Medical College Of Pennsylvania. AN HISTORICAL OUTLINE BY CLARA MARSHALL, M.D., Dean of the College. Philadelphia : P. BLAKISTON, SON & CO., I0I2 WALNUT STREET, 1897. >.rB»^aR^ Copyright, 1897, BY P. BLAKISTON, SON & CO. TO THE ALUMN/E OF THE woman's medical college OF PENNSYLVANIA. PREFACE. T^HE following account of the Woman's Medical College of Pennsylvania was originally prepared with the expectation that it would constitute one of a collection of histories of the medical colleges for women in this country, which were to be embodied " in the as part of the Report on Women in Medicine United States," prepared by Dr. Frances Emily White for the World's Congress of Representative Women, held in Chicago in 1893. The delay in the publication of the large body of the reports of this Congress, promised by the United States Govern- ment, and the receipt of frequent and urgent re- the quests for more detailed information in regard to part taken by this College in the education of women in medicine, have induced the author to publish this report as a separate volume. C. M. Philadelphia^ July i, iSgf. " 'T'HE history of the movement for introducing wo- men into the full practice of the medical profes- sion is one of the most interesting of modern times. This movement has already achieved much, and far more than is often supposed. -

The Artistic Patronage of Albrecht V and the Creation of Catholic Identity in Sixteenth
The Artistic Patronage of Albrecht V and the Creation of Catholic Identity in Sixteenth- Century Bavaria A dissertation presented to the faculty of the College of Fine Arts of Ohio University In partial fulfillment of the requirements for the degree Doctor of Philosophy Adam R. Gustafson June 2011 © 2011 Adam R. Gustafson All Rights Reserved 2 This dissertation titled The Artistic Patronage of Albrecht V and the Creation of Catholic Identity in Sixteenth- Century Bavaria by ADAM R. GUSTAFSON has been approved for the School of Interdisciplinary Arts and the College of Fine Arts _______________________________________________ Dora Wilson Professor of Music _______________________________________________ Charles A. McWeeny Dean, College of Fine Arts 3 ABSTRACT GUSTAFSON, ADAM R., Ph.D., June 2011, Interdisciplinary Arts The Artistic Patronage of Albrecht V and the Creation of Catholic Identity in Sixteenth- Century Bavaria Director of Dissertation: Dora Wilson Drawing from a number of artistic media, this dissertation is an interdisciplinary approach for understanding how artworks created under the patronage of Albrecht V were used to shape Catholic identity in Bavaria during the establishment of confessional boundaries in late sixteenth-century Europe. This study presents a methodological framework for understanding early modern patronage in which the arts are necessarily viewed as interconnected, and patronage is understood as a complex and often contradictory process that involved all elements of society. First, this study examines the legacy of arts patronage that Albrecht V inherited from his Wittelsbach predecessors and developed during his reign, from 1550-1579. Albrecht V‟s patronage is then divided into three areas: northern princely humanism, traditional religion and sociological propaganda. -

The INVISIBLE RAINBOW
The INVISIBLE RAINBOW A History of Electricity and Life Arthur Firstenberg Chelsea Green Publishing White River Junction, Vermont London, UK Copyright © 2017, 2020 by Arthur Firstenberg. All rights reserved. Drawings on pages 3 and 159 copyright © 2017 by Monika Steinhoff. “Two bees” drawing by Ulrich Warnke, used with permission. No part of this book may be transmitted or reproduced in any form by any means without permission in writing from the publisher. Originally published in 2017 by AGB Press, Santa Fe, New Mexico; Sucre, Bolivia. This paperback edition published by Chelsea Green Publishing, 2020. Book layout: Jim Bisakowski Cover design: Ann Lowe Printed in Canada. First printing February 2020. 10 9 8 7 6 5 4 3 2 1 20 21 22 23 24 Our Commitment to Green Publishing Chelsea Green sees publishing as a tool for cultural change and ecological stewardship. We strive to align our book manufacturing practices with our editorial mission and to reduce the impact of our business enterprise in the environment. We print our books and catalogs on chlorine-free recycled paper, using vegetable-based inks whenever possible. This book may cost slightly more because it was printed on paper that contains recycled fiber, and we hope you’ll agree that it’s worth it. The Invisible Rainbow was printed on paper supplied by Marquis that is made of recycled materials and other controlled sources. Library of Congress Control Number: 2020930536 ISBN 978-1-64502-009-7 (paperback) | 978-1-64502-010-3 (ebook) Chelsea Green Publishing 85 North Main Street, Suite 120 White River Junction, VT 05001 (802) 295-6300 www.chelseagreen.com In memory of Pelda Levey—friend, mentor, and fellow traveler. -

A Comedy of Scientific Errors BOVINES
SACRED A COMEDY OF SCIENTIFIC ERRORS BOVINES DOUGLAS ALLCHIN, DEPARTMENT EDITOR William Shakespeare may well have foreshadowed the modern television experiment with balm, groundsel, and spinach. All modified the air to sitcom. His comic misadventures were expertly crafted. In A Comedy of support sustained burning. Animals, too, could breathe longer in the Errors, for example, twins (with twin servants), each separated at birth, treated air. Plants, Priestley had found, could restore the “goodness” of converge unbeknownst to each other in the same town. Mistaken iden- the air depleted by respiration or combustion. American correspondent tity leads to miscommunication. More mistaken identity follows, with Benjamin Franklin immediately perceived the global implications: plants more misdelivered messages and yet more misinterpretations. Hilarious help restore the atmosphere that humans and other animals foul. The consequences ensue. It is a stock comedic formula in modern entertain- system ensures our survival. That view fit neatly with Priestley’s religious ment. A character first makes an unintentional error. Then ironically, in belief in an intentionally designed (and rational) natural world. It was a trying to correct it, things only get laughably worse. remarkable discovery. For this and other work on airs, the Royal Society Science, we imagine, is safeguarded against such embarrassing in 1772 awarded Priestley the Copley Medal, then the most prestigious episodes. In the lore of scientists, echoed among teachers, science is honor in science. “self-correcting.” Replication, in particular, ensures that errors are Others were eager to build on Priestley’s discovery about plants and exposed for what they are. Research promptly returns to its fruitful tra- the restoration of air. -

Medical News
1763 health, however, soon broke down and after practising spectacles, a fact which was often the cause of injury to for some years in Ireland he settled to private practice their eyesight. He therefore gave out that he would supply in London. He married in 1865 Agnes Letitia, youngest any applicant whom he considered deserving with a pair of daughter of the late William Robinson, LL.D., of Totten- spectacles, and in addition he personally saw the applicants ham, Middlesex, of the Inner Temple, Barrister-at-law, J.P., and tested their sight. He was a firm supporter of the local and deputy-lieutenant of the county. He became a Fellow cottage hospital and dispensary, the former of which institu- of the Royal Medical and Chirurgical Society and served as tions was mainly founded by members of his family. a member of its council in 1894-95 ; he was also a member of the Clinical Society of London. Dr. Fitz-Patrick was, DEATHS OF EMIB’E1T FOREIGN MEDICAL MEN.-The however, far more than a talented physician. He was a deaths of the eminent men are ,,aLant in its highest sense and a linguist of high order, following foreign medical conversing in Italian, German, and French almost as announced :-Dr. Heinrich Laudahn, Director of the at the of 70 flnently as in his own language, while his attainments as Lindenburg Asylum, Cologne, age years.-Dr. the of a classical scholar were far above the average. More- Leopold Grossmann, doyen Hungarian ophthalmo- at the over, he could read modern Greek with as much ease and logists, age of 79 years.-Dr. -

Archaeological Data Recovery Excavations at 38Ch1107, Kiawah Island, South Carolina
ARCHAEOLOGICAL DATA RECOVERY EXCAVATIONS AT 38CH11079 KIAWAH ISLAND, SOUTH CAROLINA CHICORA RESEARCH CONTRIBUTION 178 © 2001 by Chicora Foundation, Inc. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, transmitted, or transcribed in any form or by any means, electronic, mechanical, photocopying, recording, or otherWise without prior permission of Chicora Foundation, Inc. except for brief quotations used in reviews. Full credit must be given to the authors, publisher, and project sponsor. ARCHAEOLOGICAL DATA RECOVERY EXCAVATIONS AT 38CH1107, KIAWAH ISLAND, SOUTH CAROLINA Prepared for: Mr. Ray Pantlik Kiawah Resort Associates 7 Beachwalker Drive Kiawah Island, South Carolina 29455 Prepared By: Michael Trinkley, Ph.D. Chicora Research Contribution 178 Chicora Foundation, Inc. P.O. Box 8664 • 861 Arbutus Drive Columbia, South Carolina 29202 803/787-6910 November 10, 1995 This report is printed on permanent recycled paperoo ABSTRACT This report documents and descnbes the with the Stanyame Plantation, built in the early results of archaeological data recovery excavations eighteenth century. undertaken for Kiawah Resort Associates at 38CH1107 on Kiawah Island in Charleston County, Initial investigations, which incorporated South Carolina. It was conducted in compliance auger tests and a metal detector survey, suggested with a Memorandum of Agreement between that the site had been heavily and deeply plowed. Kiawah Resort Associates, the Army Corps of This was confirmed by the excavation of 250 Engineers, and the South Carolina State Historic square feet of contiguous units, which exposed au Preservation Office. agricultural ditch, as well as modem plowscars. The plowzone varied from LO to nearly 1.2 feet in The site was originally identified by depth. -

Development of Preservice Biology Teachers‟ Skills in the Causal Process Concerning Photosynthesis
Journal of Education and Training Studies Vol. 7, No. 4; April 2019 ISSN 2324-805X E-ISSN 2324-8068 Published by Redfame Publishing URL: http://jets.redfame.com Development of Preservice Biology Teachers‟ Skills in the Causal Process Concerning Photosynthesis Arzu Saka Correspondence: Arzu Saka, Trabzon University, Fatih Faculty of Education, Trabzon, 61335,Turkey. Received: February 12, 2019 Accepted: March 7, 2019 Online Published: March 11, 2019 doi:10.11114/jets.v7i4.4022 URL: https://doi.org/10.11114/jets.v7i4.4022 Abstract Photosynthesis is the most effective cycle and sustainable natural process known in nature. Students who learn the subject of photosynthesis well will also make better sense of other issues such as environmental problems, the state of the atmosphere, greenhouse gases, climate changes, carbon footprints and conservation of forests. The aim of this study is to present an example of a worksheet that investigates the skill levels possessed by preservice teachers‟ in the causal process, and also to examine their ability to write a photosynthesis equation by means of a history-based approach that also includes reading skills. The study was conducted with the action research method. The study sample consisted of a total of 71 preservice biology teachers. At the first stage, before the implementation of the worksheet, 34 teacher candidates from within the sample were asked a question with a diagram summarising the photosynthesis process. At the second stage, all the prospective teachers were asked for the skill levels they possessed in the causal process to be assessed via implementation of the worksheet. The answers given by the preservice teachers in the defining variables section in particular make up the least answered section of the worksheet. -

The Ancestry of James Patten
THE ANCESTRY OF JAMES PATTEN THE ANCESTRY OF JAMES PATTEN 1747?-1817 OF ARUNDEL (KENNEBUNKPORT) MAINE BY WALTER GOODWIN DA VIS PORTLAND, MAINE THE SOUTHWORTH-.ANTHOENSEN PRESS 1941 CONTENTS INTRODUCTION Vil I. MATTHEW PATTEN OF BIDDEFORD 1 II. HECTOR p A TTEN OF SACO 11 III. WILLIAM PATTEN OF Bosnrn 43 IV. RonERT PATTEN oF ARUNDEL HJ V. WILLIAM PATTEN 01<' WELLS ,·0 VI. JOHNSTON OF STROUDWATER. 89 INDEX 105 INTRODUCTION 'I'HE title of this pamphlet, The Ancestry of James Patten, is to a great extent deceptive, for on the paternal side James Patten's father is his only "ancestor" now, or likely to be, discovered, while on the maternal side we can trace a slight three generations to a shadowy great-grandfather. However, the pamphlet is the sev enth in a series dealing with the ancestry of my great-great grandparents, and for the sake of uniformity it is so entitled. Actually it deals with the descendants of six men who emigrated to New England in the early years of the eighteenth century, four of them being the brothers Matthew Patten of Biddeford, Hector Patten of Saco, Robert Patten of Arundel, and '\Villiam Patten of Boston. The fifth, ·william Patten of Wells, presumably a close kinsman of the brothers, is included as by so doing all of the Pat ten emigrants who settled in Maine are conveniently grouped in one volume, while the sixth, James Johnston, finds an appropriate place herein as his granddaughter was James Patten's mother. All of these men were of Scotch descent, springing from fami lies which left Scotland in the seventeenth century, encouraged by the British government, to settle in the northern counties of Ireland which formed the ancient kingdom of Ulster, where they became a tough and unwelcome minority. -
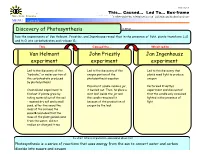
Discovery of Photosynthesis Jan Ingenhousz Experiment John
Cause / Effect TM This… Caused… Led To… Box-frame . Makes Sense Strategies © 2007 Edwin Ellis, All Rights© 2007 Reserved Edwin Published Ellis, byAll Makes Rights Sense Reserved Strategies, LLC, www.MakesSenseStrategies.com Lillian, AL www.MakesSenseStrategies.com MENU sample Name: Date: Discovery of Photosynthesis Is about … how the experiments of Van Helmont, Priestley, and Ingenhousz reveal that in the presence of light, plants transform C2O and H2O into carbohydrates and release O2. This Caused the… Which led to … Van Helmont John Priestly Jan Ingenhousz experiment experiment experiment · Led to the discovery of the · Led to the discovery of the · Led to the discovery that “hydrate,” or water portion of oxygen portion of the plants need light to produce the carbohydrate produced photosynthesis equation oxygen by photosynthesis · Placed a lit candle inside a jar, · Performed Priestly’s · Created and experiment to it burned out. Then, he place a experiment and discovered find out if plants grew by mint leaf inside the jar and that the candle only remained taking material out of the soil the candle remained lit lighted in the presence of – massed dry soil and a small because of the production of light seed, after five years the oxygen by the leaf mass of the soil was the sameèconcluded that the mass of the plant gained came from the water, did not realize air changed it too So what? What is important to understand about this? Photosynthesis is a series of reactions that uses energy from the sun to convert water and carbon dioxide into sugars and oxygen .