Community-Directed Interventions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -
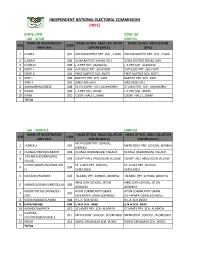
State: Oyo Code: 30 Lga : Afijio Code: 01 Name of Registration Name of Reg
INDEPENDENT NATIONAL ELECTORAL COMMISSION (INEC) STATE: OYO CODE: 30 LGA : AFIJIO CODE: 01 NAME OF REGISTRATION NAME OF REG. AREA COLLATION NAME OF REG. AREA CENTRE S/N CODE AREA (RA) CENTRE (RACC) (RAC) 1 ILORA I 001 OKEDIJI BAPTIST PRY. SCH., ILORA OKEDIJI BAPTIST PRY. SCH., ILORA 2 ILORA II 002 ILORA BAPTIST GRAM. SCH. ILORA BAPTIST GRAM. SCH. 3 ILORA III 003 L.A PRY SCH. ALAWUSA. L.A PRY SCH. ALAWUSA. 4 FIDITI I 004 CATHOLIC PRY. SCH FIDITI CATHOLIC PRY. SCH FIDITI 5 FIDITI II 005 FIRST BAPTIST SCH. FIDITI FIRST BAPTIST SCH. FIDITI 6 AWE I 006 BAPTIST PRY. SCH. AWE BAPTIST PRY. SCH. AWE 7 AWE II 007 AWE HIGH SCH. AWE HIGH SCH. 8 AKINMORIN/JOBELE 008 ST.JOHN PRY. SCH. AKINMORIN ST.JOHN PRY. SCH. AKINMORIN 9 IWARE 009 L.A PRY SCH. IWARE. L.A PRY SCH. IWARE. 10 IMINI 010 COURT HALL 1, IMINI COURT HALL 1, IMINI TOTAL LGA : AKINYELE CODE: 02 NAME OF REGISTRATION NAME OF REG. AREA COLLATION NAME OF REG. AREA COLLATION S/N CODE AREA (RA) CENTRE (RACC) CENTRE (RACC) METHODIST PRY. SCHOOL, 1 IKEREKU 001 METHODIST PRY. SCHOOL, IKEREKU IKEREKU 2 OLANLA/OBODA/LABODE 002 OLANLA (OGBANGAN) VILLAGE OLANLA (OGBANGAN) VILLAGE EOLANLA (OGBANGAN) 3 003 COURT HALL ARULOGUN VILLAGE COURT HALL ARULOGUN VILLAGE VILLAG OLODE/AMOSUN/ONIDUND ST. LUKES PRY. SCHOOL, ST. LUKES PRY. SCHOOL, 4 004 U ONIDUNDU ONIDUNDU 5 OJO-EMO/MONIYA 005 ISLAMIC PRY. SCHOOL, MONIYA ISLAMIC PRY. SCHOOL, MONIYA ANGLICAN SCHOOL, OTUN ANGLICAN SCHOOL, OTUN 6 AKINYELE/ISABIYI/IREPODUN 006 AGBAKIN AGBAKIN IWOKOTO/TALONTAN/IDI- AYUN COMMUNITY GRAM. -

Oyo State Ubec Fts Shortlist
UNIVERSAL BASIC EDUCATION COMMISSION (UBEC) FEDERAL TEACHERS’ SCHEME (FTS) SHORTLISTED CANDIDATES OYO STATE EXAM S/NO NAME STATE LGA SEX COURSE OF STUDY STATUS NO AMINAT ODEDELE 1 001YY OYO AFIJIO F PHYSICS/MATHEMATICS SHORTLISTED OMOLOLA ABOSEDE 2 002YY AKINRINOLA OYO AFIJIO F BIOLOGY EDUCATION SHORTLISTED DEBORAH ESTHER 3 003YY FEYISETAN OYO AFIJIO F EDUCATION/ENGLISH SHORTLISTED OLUWAFERANMI OLUWATOYIN INTEGRATED 4 004YY OLAGBAMI OYO AFIJIO F SHORTLISTED SCIENCE/BIOLOGY IFEOLUWA SUNDAY 5 005YY ADEKANBI OYO AFIJIO M MATHEMATICS SHORTLISTED OLANREWAJU OLUWATOSIN 6 006YY OYO AFIJIO M EDUCATION/MATHEMATICS SHORTLISTED AKANO JOHN BLESSING 7 007YY ADEBOWALE OYO AFIJIO F BIOLOGY /CHEMISTRY SHORTLISTED OPEYEMI ADEBUNMI OJO 8 008YY OYO AFIJIO F HOME ECONOMICS SHORTLISTED NIKE IFETAYO DAIRO 9 009YY OYO AFIJIO M HUMAN KINETICS SHORTLISTED ELIJAH ADEOLU ADELEYE 10 010YY OYO AFIJIO M SPECIAL EDUCATION/MATHE SHORTLISTED AKINTUNDE REUBEN 11 011YY FUNMILAYO OYO AFIJIO M YORUBA SHORTLISTED ADEGOKE TOHEEB AJAO SPECIAL 12 012YY OYO AFIJIO M SHORTLISTED OPEYEMI EDUCATION/MATHEM ABOSEDE 13 013YY OGUNTUNJI OYO AFIJIO F BIOLOGY SHORTLISTED REBECCA OMOLOLA 14 014YY OGUNKUNLE OYO AFIJIO F BIOLOGY EDUCATION SHORTLISTED ABOSEDE FAITH OLAJIRE 15 015YY OYO AKINYELE F MATHEMATICS/GEOGRAPHY SHORTLISTED OMOWUMI TITILOPE AREMU 16 016YY OYO AKINYELE F FINE ART SHORTLISTED ADEBISI RAFIAT COMPUTER 17 017YY SALAWUDEEN OYO AKINYELE F SHORTLISTED SCIENCE/MATHEMA ADENIKE GAFAR KOLAPO ENGLISH LANGUAGE AND 18 018YY OYO AKINYELE M SHORTLISTED ABIODUN YORUBA TEJUMADE 19 019YY -

(GIS) in Oyo State, Nigeria
Journal of Geography, Environment and Earth Science International 11(1): 1-15, 2017; Article no.JGEESI.34634 ISSN: 2454-7352 Mapping Groundwater Quality Parameters Using Geographic Information System (GIS) in Oyo State, Nigeria T. O. Ogunbode 1* and I. P. Ifabiyi 2 1Faculty of Basic Medical and Health Sciences, Bowen University, Iwo, Nigeria. 2Department of Geography and Environmental Management, University of Ilorin, Nigeria. Authors’ contributions This work was carried out in collaboration between both authors. Both authors read and approved the final manuscript. Article Information DOI: 10.9734/JGEESI/2017/34634 Editor(s): (1) Wen-Cheng Liu, Department of Civil and Disaster Prevention Engineering, National United University, Taiwan and Taiwan Typhoon and Flood Research Institute, National United University, Taipei, Taiwan. Reviewers: (1) H. O. Nwankwoala, University of Port Harcourt, Nigeria. (2) Dorota Porowska, University of Warsaw, Poland. Complete Peer review History: http://www.sciencedomain.org/review-history/20122 Received 2nd June 2017 th Original Research Article Accepted 9 July 2017 Published 19 th July 2017 ABSTRACT The knowledge of spatial pattern of groundwater quality is important to ensure a holistic approach to the management of the resource quality status in space and time. Thus a sample each of underground water was collected from each of the selected 5 rural communities in each of the selected 25 out of the 33 LGAs in Oyo State for the purpose of quality assessments. Eleven (11) + parameters namely water temperature (°C), pH, electr ical conductivity (EC), Sodium (Na ), SO 4, + Potassium (K ), Nitrate (NO 3), Phosphate (PO 3), coli-form count, Oxidation Redox Potential (ORP) and Total Dissolved Solids (TDS) were subjected to standard laboratory analysis. -

The Election Management System (Ems) Project Report
THE ELECTION MANAGEMENT SYSTEM (EMS) PROJECT REPORT Independent National Electoral Commission, Abuja ©2015 Table of Contents Table of Contents .................................................................................................................................... 2 Abbreviations .......................................................................................................................................... 3 Foreword ................................................................................................................................................. 4 Acknowledgments ................................................................................................................................... 5 List of Figures and Tables ........................................................................................................................ 6 Executive Summary ................................................................................................................................. 8 1.0 Background to the EMS Project ................................................................................................ 11 1.1 Establishment of the EMS Project Committee ......................................................................... 15 1.2 Membership .............................................................................................................................. 16 1.3 Terms of Reference .................................................................................................................. -
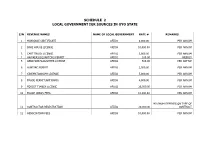
Schedule 2 Local Government Igr Sources in Oyo State
SCHEDULE 2 LOCAL GOVERNMENT IGR SOURCES IN OYO STATE S/N REVENUE NAMES NAME OF LOCAL GOVERNMENT RATE # REMARKS 1 MARRIAGE CERTIFICATE AFIJIO 8,000.00 PER ANNUM 2 BAKE HOUSE LICENSE AFIJIO 10,000.00 PER ANNUM 3 CART TRUCK LICENSE AFIJIO 3,000.00 PER ANNUM 4 HAWKERS/SQUARTORS PERMIT AFIJIO 100.00 WEEKLY 5 ABBATOIR/SLAUGHTER LICENSE AFIJIO 500.00 PER CATTLE 6 HUNTING PERMIT AFIJIO 2,500.00 PER ANNUM 7 CINEMATOGRAPH LICENSE AFIJIO 5,000.00 PER ANNUM 8 TRADE PERMIT(ARTISANS) AFIJIO 4,000.00 PER ANNUM 9 FOREST TIMBER LICENSE AFIJIO 25,000.00 PER ANNUM 10 TRADE UNION FEES AFIJIO 10,000.00 PER ANNUM MINIMUM DEPENDS ON TYPE OF 11 CONTRACTOR REGISTRATION AFIJIO 20,000.00 CONTRACT 12 ASSOCIATION FEES AFIJIO 10,000.00 PER ANNUM MINIMUM DEPENDS ON NATURE 13 TENDERS FEES AFIJIO 30,000.00 OF CONTRACT 14 DEATH REGISTRATION CERTIFICATE AFIJIO 2,500.00 PER CHILD 15 DEVELOPMENT LEVIES AFIJIO 200.00 PER ANNUM 16 PARKING FEES AFIJIO 200.00 DAILY 17 LOCAL GOVERNMENT IDENTIFICATION AFIJIO 2,500.00 18 PROCEED FROM SALES OF GOODS/FARM PRODUCES AFIJIO VARIES 19 SALES OF SCRAPS AFIJIO VARIES 20 EARNING FROM COMMERCIAL ACTIVITIES AFIJIO VARIES 21 EARNING FROM PARK AND GARDEN AFIJIO 500.00 PER PERSON 22 EARNING FROM GUEST HOUSE AFIJIO 10,000.00 PER ANNUM 23 POLLS TAX AFIJIO 1,000.00 PER ANNUM MINIMUN. DEPENDS ON 24 LIVESTOCK AFIJIO 1,000.00 PRODUCT 25 TENAMENT RATES AFIJIO 2,300.00 MINIMUN. DEPEND ONSIZE 26 BULL PERMIT AFIJIO 5,000.00 PER ANNUM 27 WHEEL BARROW FEES AFIJIO 50.00 DAILY 28 SHOP AND KIOSK FEES AFIJIO 200.00 PER MONTH 29 MARKET SQUATER AFIJIO 50.00 PER -

Khalil Samihah a Case Study of Service Delivery by Local
CIEA7 #38: DILEMMAS OF AFRICAN MODERNITY AND THEIR THEORETICAL CHALLENGES. Khalil Samihah [email protected] Salihu Abdulwaheed Adelabu [email protected] A Case study of Service Delivery by Local Government Councils in Oyo state in relation to Fund and Constitutional Issues Purpose - The purpose of the paper is to review the performance of Local government councils in Oyo state of Nigeria from two major view lens viz-a-viz Constitutional and Fund/Statutory allocation perspectives in relation to service delivery. Design/methodology/approach – The research adopts quantitative and qualitative approach. Correlation between service delivery and fund/statutory allocation is established in order to assess the solvency of fund flow in the Local Government Councils. Findings – Contrary to the findings of previous studies that fund is always insufficient, the result shows that fund flow in Nigerian Local government councils is regular and sufficient to provide basic essential services. Research limitations/implications – This paper covers only 33 out of 774 Local government councils in Nigeria. Originality/value –The policy-makers can use the findings of this study to help inform future decisions with respect to service delivery in Nigeria. Service Delivery, Constitution, Fund/ Resource Allocation. Universiti Utara Malaysia. Universiti Utara Malaysia. 7.º CONGRESSO IBÉRICO DE ESTUDOS AFRICANOS | 7.º CONGRESO DE ESTUDIOS AFRICANOS | 7TH CONGRESS OF AFRICAN STUDIES LISBOA 2010 Khalil Samihah & Salihu Abdulwaheed Adelabu 2 INTRODUCTION Development is synonymous to freedom in any society. If a society is developed, the people in that society is always said to be free from diseases, hunger, poverty, illness, illiteracy, ignorance, and insecurity. -
New Projects Inserted by Nass
NEW PROJECTS INSERTED BY NASS CODE MDA/PROJECT 2018 Proposed Budget 2018 Approved Budget FEDERAL MINISTRY OF AGRICULTURE AND RURAL SUPPLYFEDERAL AND MINISTRY INSTALLATION OF AGRICULTURE OF LIGHT AND UP COMMUNITYRURAL DEVELOPMENT (ALL-IN- ONE) HQTRS SOLAR 1 ERGP4145301 STREET LIGHTS WITH LITHIUM BATTERY 3000/5000 LUMENS WITH PIR FOR 0 100,000,000 2 ERGP4145302 PROVISIONCONSTRUCTION OF SOLAR AND INSTALLATION POWERED BOREHOLES OF SOLAR IN BORHEOLEOYO EAST HOSPITALFOR KOGI STATEROAD, 0 100,000,000 3 ERGP4145303 OYOCONSTRUCTION STATE OF 1.3KM ROAD, TOYIN SURVEYO B/SHOP, GBONGUDU, AKOBO 0 50,000,000 4 ERGP4145304 IBADAN,CONSTRUCTION OYO STATE OF BAGUDU WAZIRI ROAD (1.5KM) AND EFU MADAMI ROAD 0 50,000,000 5 ERGP4145305 CONSTRUCTION(1.7KM), NIGER STATEAND PROVISION OF BOREHOLES IN IDEATO NORTH/SOUTH 0 100,000,000 6 ERGP445000690 SUPPLYFEDERAL AND CONSTITUENCY, INSTALLATION IMO OF STATE SOLAR STREET LIGHTS IN NNEWI SOUTH LGA 0 30,000,000 7 ERGP445000691 TOPROVISION THE FOLLOWING OF SOLAR LOCATIONS: STREET LIGHTS ODIKPI IN GARKUWARI,(100M), AMAKOM SABON (100M), GARIN OKOFIAKANURI 0 400,000,000 8 ERGP21500101 SUPPLYNGURU, YOBEAND INSTALLATION STATE (UNDER OF RURAL SOLAR ACCESS STREET MOBILITY LIGHTS INPROJECT NNEWI (RAMP)SOUTH LGA 0 30,000,000 9 ERGP445000692 TOSUPPLY THE FOLLOWINGAND INSTALLATION LOCATIONS: OF SOLAR AKABO STREET (100M), LIGHTS UHUEBE IN AKOWAVILLAGE, (100M) UTUH 0 500,000,000 10 ERGP445000693 ANDEROSION ARONDIZUOGU CONTROL IN(100M), AMOSO IDEATO - NCHARA NORTH ROAD, LGA, ETITI IMO EDDA, STATE AKIPO SOUTH LGA 0 200,000,000 11 ERGP445000694 -

Radiation Mapping of Oyo State, Southwestern Nigeria
RADIATION MAPPING OF OYO STATE, SOUTHWESTERN NIGERIA BY OLATUNJI, ADEMOLA SUNDAY PHY/13/6011 A THESIS IN THE DEPARTMENT OF PHYSICS SUBMITTED TO THE SCHOOL OF POSTGRADUATE STUDIES, FEDERAL UNIVERSITY OF TECHNOLOGY, AKURE, ONDO STATE, NIGERIA. IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF THE DEGREE OF MASTER OF TECHNOLOGY (M.TECH) IN PHYSICS (RADIATION AND HEALTH PHYSICS OPTION). MAY, 2016. ABSTRACT Exposure of human beings to radiation cannot be measured or quantified by human senses. These radiations differ in their hardness and ability to penetrate materials. The implications of radiation on human body include biological, acute, generic and somatic effects. The studies comprehensively determine ambient ionizing radiation and also took inventory of the spatial distribution of ambient ionizing radiation in Oyo State. Exposure rate was measured at 1m above the ground level with the use of a Geiger-Müller-counter, at positions measured by Global Positioning System (GPS). About one hundred and twenty (120) towns and villages were visited taking from three to five towns in each of the thirty-three local government areas of the state. The collected data was super-imposed on a digital map of Oyo State to produce the isodose map, elevation map, and the mean dose map to identify areas of elevated risks of ambient ionizing radiation in the study using ARCGISTM & SURFERTM software. Results indicate that areas like Saki East and West, Irepo, Orelope, Olorunsogo and Ori Ire local governments had higher exposure rate with dose range of 0.34-0.38 µSv/hr while areas like Oluyole, Iddo, Iseyin, Ona Ara, Lagelu, Itesiwaju, Oyo East and West local governments and all the local governments in Ibadan axes had lower exposure rate with dose range of 0.12-0.20 µSv/hr. -

States and Lcdas Codes.Cdr
PFA CODES 28 UKANEFUN KPK AK 6 CHIBOK CBK BO 8 ETSAKO-EAST AGD ED 20 ONUIMO KWE IM 32 RIMIN-GADO RMG KN KWARA 9 IJEBU-NORTH JGB OG 30 OYO-EAST YYY OY YOBE 1 Stanbic IBTC Pension Managers Limited 0021 29 URU OFFONG ORUKO UFG AK 7 DAMBOA DAM BO 9 ETSAKO-WEST AUC ED 21 ORLU RLU IM 33 ROGO RGG KN S/N LGA NAME LGA STATE 10 IJEBU-NORTH-EAST JNE OG 31 SAKI-EAST GMD OY S/N LGA NAME LGA STATE 2 Premium Pension Limited 0022 30 URUAN DUU AK 8 DIKWA DKW BO 10 IGUEBEN GUE ED 22 ORSU AWT IM 34 SHANONO SNN KN CODE CODE 11 IJEBU-ODE JBD OG 32 SAKI-WEST SHK OY CODE CODE 3 Leadway Pensure PFA Limited 0023 31 UYO UYY AK 9 GUBIO GUB BO 11 IKPOBA-OKHA DGE ED 23 ORU-EAST MMA IM 35 SUMAILA SML KN 1 ASA AFN KW 12 IKENNE KNN OG 33 SURULERE RSD OY 1 BADE GSH YB 4 Sigma Pensions Limited 0024 10 GUZAMALA GZM BO 12 OREDO BEN ED 24 ORU-WEST NGB IM 36 TAKAI TAK KN 2 BARUTEN KSB KW 13 IMEKO-AFON MEK OG 2 BOSARI DPH YB 5 Pensions Alliance Limited 0025 ANAMBRA 11 GWOZA GZA BO 13 ORHIONMWON ABD ED 25 OWERRI-MUNICIPAL WER IM 37 TARAUNI TRN KN 3 EDU LAF KW 14 IPOKIA PKA OG PLATEAU 3 DAMATURU DTR YB 6 ARM Pension Managers Limited 0026 S/N LGA NAME LGA STATE 12 HAWUL HWL BO 14 OVIA-NORTH-EAST AKA ED 26 26 OWERRI-NORTH RRT IM 38 TOFA TEA KN 4 EKITI ARP KW 15 OBAFEMI OWODE WDE OG S/N LGA NAME LGA STATE 4 FIKA FKA YB 7 Trustfund Pensions Plc 0028 CODE CODE 13 JERE JRE BO 15 OVIA-SOUTH-WEST GBZ ED 27 27 OWERRI-WEST UMG IM 39 TSANYAWA TYW KN 5 IFELODUN SHA KW 16 ODEDAH DED OG CODE CODE 5 FUNE FUN YB 8 First Guarantee Pension Limited 0029 1 AGUATA AGU AN 14 KAGA KGG BO 16 OWAN-EAST -
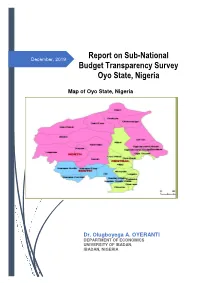
Final Revised Oyo State Report Dec 23
Report on Sub-National December, 2019 Budget Transparency Survey Oyo State, Nigeria Map of Oyo State, Nigeria Dr. Olugboyega A. OYERANTI DEPARTMENT OF ECONOMICS UNIVERSITY OF IBADAN, IBADAN, NIGERIA Executive Summary This report presents the outcomes of the performance of Oyo State in 2018 in respect of four major indexes captured in the Budget Transparency Survey. The indexes are State Budget Transparency Index (SBTI), State Budget Document Availability Index (SBDAI), State Public Participation Index (SPPI) and State Procurement Process Index (SPrPI). The 2018 Sub-National Budget Transparency Survey was the second following similar survey in 2015. Oyo State was involved in the two exercises and this has allowed for a comparative analysis that exposed how the State responded to the outcome of the 2015 survey as seen in the outcome for 2018. The scores of the State for the four indexes showed 7 for State Budget Transparency Index (SBTI), 11 for State Budget Document Availability Index (SBDAI), 0 for State Public Participation Index (SPPI) and 20 for State Procurement Process Index (SPrPI). The scores for 2015 were 7, 8, 0, and 10, respectively. Each of the scores wwas benchmarked to a maximum value of 100. The performance of the State in 2018 leaves so much to be desired, particularly for the new administration that has just come on board in the State. Obviously, all hands must be on deck to bring about improved and better performance as far as budget process matters are concerned in the State. There is no evidence to suggest the dearth of manpower required to change the current image of budget process in the State. -

(Title of the Thesis)*
The Role of Social capital in Community-Based Urban Solid Waste Management: Case Studies from Ibadan Metropolis, Nigeria by Samuel Wahab A thesis presented to the University of Waterloo in fulfillment of the thesis requirement for the degree of Doctor of Philosophy in Planning Waterloo, Ontario, Canada, 2012 © Samuel Wahab 2012 AUTHOR'S DECLARATION I hereby declare that I am the sole author of this thesis. This is a true copy of the thesis including any required final revisions, as accepted by my examiners. I understand that my thesis may be made available to the public. ii Abstract Urban solid waste management (USWM) problems facing cities in the developed and developing world are well documented; however, progress in tackling them is very slow in the latter. There are still many communities, neighbourhoods, and local markets where garbage is not collected for a considerable length of time. Many of the affected houses are situated in poor neighbourhoods on the edges and core areas of cities. In order to secure the future of urban environments in the developing world from continuous or perpetual decay, it is important to study the role of social capital in urban solid waste management. Toward this end, a case study research was carried out in Ibadan, Nigeria. For the purpose of the study, social capital was defined as the attributes of social organization, such as trust, cultural norms and social networks by which communities facilitate action. Emerging research suggests that social capital might have an important role to play in effective community-based urban solid waste management initiatives.