Community-Directed Interventions for Priority Health Problems in Africa: Results of a Multicountry Study the CDI Study Groupa
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

AFRREV STECH, Vol. 3(2) May, 2014
AFRREV STECH, Vol. 3(2) May, 2014 AFRREV STECH An International Journal of Science and Technology Bahir Dar, Ethiopia Vol. 3 (2), S/No 7, May, 2014: 51-65 ISSN 2225-8612 (Print) ISSN 2227-5444 (Online) http://dx.doi.org/10.4314/stech.v3i2.4 THE USE OF COMPOSITE WATER POVERTY INDEX IN ASSESSING WATER SCARCITY IN THE RURAL AREAS OF OYO STATE, NIGERIA IFABIYI, IFATOKUN PAUL Department of Geography and Environmental Management, Faculty of Social Sciences University of Ilorin; Ilorin, Kwara State, Nigeria E-mail: 234 8033231626 & OGUNBODE, TIMOTHY OYEBAMIJI Faculty of Law Bowen University, Iwo Osun State, Nigeria Abstract Physical availability of water resources is beneficial to man when it is readily accessible. Oyo State is noted for abundant surface water and appreciable groundwater resources in its pockets of regolith aquifers; as it has about eight months of rainy season and a relatively deep weathered regolith. In spite of this, cases of water associated diseases Copyright© IAARR 2014: www.afrrevjo.net 51 Indexed and Listed in AJOL, ARRONET AFRREV STECH, Vol. 3(2) May, 2014 and deaths have been reported in the rural areas of the state. This study attempts to conduct an investigation into accessibility to potable water in the rural areas of Oyo State, Nigeria via the component approach of water poverty index (WPI). Multistage method of sampling was applied to select 5 rural communities from 25 rural LGAs out of the 33 LGAs in the State. Data were collected through the administration of 1,250 copies of questionnaire across 125 rural communities. Component Index method as developed by Sullivan, et al (2003) was modified and used in this study. -
OYO STATE UNIVERSAL BASIC EDUCATION BOARD (OYO SUBEB) P.M. B. 5150, SECRETARIAT, IBADAN E-Mail: [email protected] INVITATION
OYO STATE UNIVERSAL BASIC EDUCATION BOARD (OYO SUBEB) P.M. B. 5150, SECRETARIAT, IBADAN E-mail: [email protected] INVITATION TO TENDER OYO STATE UNIVERSAL BASIC EDUCATION BOARD The Oyo State Universal Basic Education Board (OYO SUBEB) intends to apply the 2014, 2015, 2016 & 2017 FGN-UBEC/OYOSUBEB Intervention Funds for the following facilities to be provided in the Public Primary and Junior Secondary Schools. Applications are therefore invited from competent companies to bid for the various works. (2) TENDER QUALIFICATION Each tender should be accompanied with the following: (a) Evidence of Company’s Certificate of Registration with Corporate Affairs Commission (CAC) (b) Evidence of Company’s tax clearance certificate (3 years) with Federal Inland Revenue Services. (FIRS). (c) Evidence of company’s registration with Oyo State Bureau of Public Procurement (d) Evidence of veritable previously executed jobs with certificate of practical completion (Contractors with history of abandoned projects or poorly executed projects will not be considered). (e) Company profile with list of relevant professionals. (f) Evidence of Registration of Business Premises with Oyo State Government. (g) Tax Clearance Certificate of at least 2 Directors (Limited Liability Company) or the Proprietor/Partner (Enterprise) for the last three (3) years. (h) Evidence of payment of Tender Fee for each LOT. (i) A sworn affidavit in line with the provision of part IV, section22 (6a, b, c, e & f) of the Oyo State Public Procurement Law 2010 stating that none of the persons connected with the bid process in the procuring entity or bureau has any pecuniary interest and that the company is not in receivership of any form of insolvency, bankrupt nor debarment and that the company nor any of the directors) of the company has been convicted of financial crimes. -
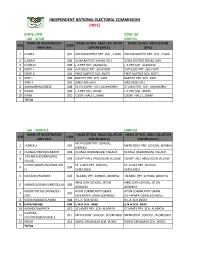
State: Oyo Code: 30 Lga : Afijio Code: 01 Name of Registration Name of Reg
INDEPENDENT NATIONAL ELECTORAL COMMISSION (INEC) STATE: OYO CODE: 30 LGA : AFIJIO CODE: 01 NAME OF REGISTRATION NAME OF REG. AREA COLLATION NAME OF REG. AREA CENTRE S/N CODE AREA (RA) CENTRE (RACC) (RAC) 1 ILORA I 001 OKEDIJI BAPTIST PRY. SCH., ILORA OKEDIJI BAPTIST PRY. SCH., ILORA 2 ILORA II 002 ILORA BAPTIST GRAM. SCH. ILORA BAPTIST GRAM. SCH. 3 ILORA III 003 L.A PRY SCH. ALAWUSA. L.A PRY SCH. ALAWUSA. 4 FIDITI I 004 CATHOLIC PRY. SCH FIDITI CATHOLIC PRY. SCH FIDITI 5 FIDITI II 005 FIRST BAPTIST SCH. FIDITI FIRST BAPTIST SCH. FIDITI 6 AWE I 006 BAPTIST PRY. SCH. AWE BAPTIST PRY. SCH. AWE 7 AWE II 007 AWE HIGH SCH. AWE HIGH SCH. 8 AKINMORIN/JOBELE 008 ST.JOHN PRY. SCH. AKINMORIN ST.JOHN PRY. SCH. AKINMORIN 9 IWARE 009 L.A PRY SCH. IWARE. L.A PRY SCH. IWARE. 10 IMINI 010 COURT HALL 1, IMINI COURT HALL 1, IMINI TOTAL LGA : AKINYELE CODE: 02 NAME OF REGISTRATION NAME OF REG. AREA COLLATION NAME OF REG. AREA COLLATION S/N CODE AREA (RA) CENTRE (RACC) CENTRE (RACC) METHODIST PRY. SCHOOL, 1 IKEREKU 001 METHODIST PRY. SCHOOL, IKEREKU IKEREKU 2 OLANLA/OBODA/LABODE 002 OLANLA (OGBANGAN) VILLAGE OLANLA (OGBANGAN) VILLAGE EOLANLA (OGBANGAN) 3 003 COURT HALL ARULOGUN VILLAGE COURT HALL ARULOGUN VILLAGE VILLAG OLODE/AMOSUN/ONIDUND ST. LUKES PRY. SCHOOL, ST. LUKES PRY. SCHOOL, 4 004 U ONIDUNDU ONIDUNDU 5 OJO-EMO/MONIYA 005 ISLAMIC PRY. SCHOOL, MONIYA ISLAMIC PRY. SCHOOL, MONIYA ANGLICAN SCHOOL, OTUN ANGLICAN SCHOOL, OTUN 6 AKINYELE/ISABIYI/IREPODUN 006 AGBAKIN AGBAKIN IWOKOTO/TALONTAN/IDI- AYUN COMMUNITY GRAM. -

Oyo State Ubec Fts Shortlist
UNIVERSAL BASIC EDUCATION COMMISSION (UBEC) FEDERAL TEACHERS’ SCHEME (FTS) SHORTLISTED CANDIDATES OYO STATE EXAM S/NO NAME STATE LGA SEX COURSE OF STUDY STATUS NO AMINAT ODEDELE 1 001YY OYO AFIJIO F PHYSICS/MATHEMATICS SHORTLISTED OMOLOLA ABOSEDE 2 002YY AKINRINOLA OYO AFIJIO F BIOLOGY EDUCATION SHORTLISTED DEBORAH ESTHER 3 003YY FEYISETAN OYO AFIJIO F EDUCATION/ENGLISH SHORTLISTED OLUWAFERANMI OLUWATOYIN INTEGRATED 4 004YY OLAGBAMI OYO AFIJIO F SHORTLISTED SCIENCE/BIOLOGY IFEOLUWA SUNDAY 5 005YY ADEKANBI OYO AFIJIO M MATHEMATICS SHORTLISTED OLANREWAJU OLUWATOSIN 6 006YY OYO AFIJIO M EDUCATION/MATHEMATICS SHORTLISTED AKANO JOHN BLESSING 7 007YY ADEBOWALE OYO AFIJIO F BIOLOGY /CHEMISTRY SHORTLISTED OPEYEMI ADEBUNMI OJO 8 008YY OYO AFIJIO F HOME ECONOMICS SHORTLISTED NIKE IFETAYO DAIRO 9 009YY OYO AFIJIO M HUMAN KINETICS SHORTLISTED ELIJAH ADEOLU ADELEYE 10 010YY OYO AFIJIO M SPECIAL EDUCATION/MATHE SHORTLISTED AKINTUNDE REUBEN 11 011YY FUNMILAYO OYO AFIJIO M YORUBA SHORTLISTED ADEGOKE TOHEEB AJAO SPECIAL 12 012YY OYO AFIJIO M SHORTLISTED OPEYEMI EDUCATION/MATHEM ABOSEDE 13 013YY OGUNTUNJI OYO AFIJIO F BIOLOGY SHORTLISTED REBECCA OMOLOLA 14 014YY OGUNKUNLE OYO AFIJIO F BIOLOGY EDUCATION SHORTLISTED ABOSEDE FAITH OLAJIRE 15 015YY OYO AKINYELE F MATHEMATICS/GEOGRAPHY SHORTLISTED OMOWUMI TITILOPE AREMU 16 016YY OYO AKINYELE F FINE ART SHORTLISTED ADEBISI RAFIAT COMPUTER 17 017YY SALAWUDEEN OYO AKINYELE F SHORTLISTED SCIENCE/MATHEMA ADENIKE GAFAR KOLAPO ENGLISH LANGUAGE AND 18 018YY OYO AKINYELE M SHORTLISTED ABIODUN YORUBA TEJUMADE 19 019YY -

Attitude and Practice of Males Towards Antenatal Care in Saki West Local Government Area of Oyo State, Nigeria
Advances in Life Science and Technology www.iiste.org ISSN 2224-7181 (Paper) ISSN 2225-062X (Online) Vol.22, 2014 Attitude and Practice of Males towards Antenatal Care in Saki West Local Government Area of Oyo State, Nigeria Akintaro Opeyemi Akinpelu 1* Olabisi Isaiah Oluwaseyi 2 1. Department of Human Kinetics and Health Education, Faculty of Education, University of Ibadan, Ibadan, Nigeria. 2. Department of Nursing, Faculty of Basic Medical Sciences, Obafemi Awolowo University, Ile-Ife, Nigeria * E-mail of corresponding author: [email protected] Abstract This study examined attitude and practice of males towards antenatal care in Saki West Local Government Area of Oyo State, Nigeria. Descriptive survey research design was used for this study and the instrument for data collection is self developed questionnaire in four-point Likert scale format with reliability coefficient of 0.76. Men of reproductive age in Saki metropolis formed the population for this study while the total sample for the study is one hundred and twenty (120) men of reproductive age. Three hypotheses were raised and tested at 0.05 alpha level using inferential statistics of Chi-Square. The result showed, among other findings, that there is significant relationship between men’s level of education and their participation in antenatal care. Consequent upon this, it was recommended that improved strategies hinged on enlightenment and orientation of men should be developed. Key words: antenatal care, male involvement, maternal health, Saki. Introduction Pregnancy and childbirth are privilege functions of women germane for the survival of our species but sometimes comes with potential risks that women should be protected from and this responsibility calls for collective support of the entire family, including the husband. -

(GIS) in Oyo State, Nigeria
Journal of Geography, Environment and Earth Science International 11(1): 1-15, 2017; Article no.JGEESI.34634 ISSN: 2454-7352 Mapping Groundwater Quality Parameters Using Geographic Information System (GIS) in Oyo State, Nigeria T. O. Ogunbode 1* and I. P. Ifabiyi 2 1Faculty of Basic Medical and Health Sciences, Bowen University, Iwo, Nigeria. 2Department of Geography and Environmental Management, University of Ilorin, Nigeria. Authors’ contributions This work was carried out in collaboration between both authors. Both authors read and approved the final manuscript. Article Information DOI: 10.9734/JGEESI/2017/34634 Editor(s): (1) Wen-Cheng Liu, Department of Civil and Disaster Prevention Engineering, National United University, Taiwan and Taiwan Typhoon and Flood Research Institute, National United University, Taipei, Taiwan. Reviewers: (1) H. O. Nwankwoala, University of Port Harcourt, Nigeria. (2) Dorota Porowska, University of Warsaw, Poland. Complete Peer review History: http://www.sciencedomain.org/review-history/20122 Received 2nd June 2017 th Original Research Article Accepted 9 July 2017 Published 19 th July 2017 ABSTRACT The knowledge of spatial pattern of groundwater quality is important to ensure a holistic approach to the management of the resource quality status in space and time. Thus a sample each of underground water was collected from each of the selected 5 rural communities in each of the selected 25 out of the 33 LGAs in Oyo State for the purpose of quality assessments. Eleven (11) + parameters namely water temperature (°C), pH, electr ical conductivity (EC), Sodium (Na ), SO 4, + Potassium (K ), Nitrate (NO 3), Phosphate (PO 3), coli-form count, Oxidation Redox Potential (ORP) and Total Dissolved Solids (TDS) were subjected to standard laboratory analysis. -

7.Results of Geophysical Survey
7.Results of Geophysical Survey 1. General 1-1 Purpose of Geophysical Survey The purpose of the geophysical survey is to find the promising communities with high potential ground water development. 1-2 Contents of geophysical survey -1st Stage (BD1) The geophysical survey was conducted in 100 communities of high priority selected among 220 communities -2nd stage(BD2) 56 communities among 100 communities were analyzed as low potential water development in 1st stage. The geophysical re-survey conducted at these 56 communities and in the new 17 additional communities. Total of geophysical survey including re-survey is 117communities (173 sites). ① Electromagnetic Survey ・Method :Loop-Loop (Srigram) ・Line :more than200 m(5 m interval) ・Equipment :GEONICS EM34 ・Analysis :Horizontal Electric Conductivity Profiling ② Resistivity Survey ・Method :Schlumberger method ・Survey depth:a=100m ・Equipment :ABEM SAS300B ・Analysis :1dimention inversion 2. Result of survey 2-1 Potential of Ground Water Basement of survey area is composed with crystal formation (Granite, Gneiss) in Precambrian Period. Upper stratum is weathered. According to the situation of weathered zone, crack and fault in crystal rock (Granite, Gneiss), the formation of aquifer is not constant due to thickness of weathered zone and scale of crack etc. Formation of aquifer are as follow: ・ It is difficult to find aquifer in fissure zone ・ Main aquifer from the test boreholes are located in the boundary between weathered zone and basement. ・ The thickness of weathered zone needs to be more than 20m for high potential of water development ・ Based on the electric conductivity and existing data, the resistivity of weathered zone needs to be less than 130 ohm-m. -

The Election Management System (Ems) Project Report
THE ELECTION MANAGEMENT SYSTEM (EMS) PROJECT REPORT Independent National Electoral Commission, Abuja ©2015 Table of Contents Table of Contents .................................................................................................................................... 2 Abbreviations .......................................................................................................................................... 3 Foreword ................................................................................................................................................. 4 Acknowledgments ................................................................................................................................... 5 List of Figures and Tables ........................................................................................................................ 6 Executive Summary ................................................................................................................................. 8 1.0 Background to the EMS Project ................................................................................................ 11 1.1 Establishment of the EMS Project Committee ......................................................................... 15 1.2 Membership .............................................................................................................................. 16 1.3 Terms of Reference .................................................................................................................. -

Gamma Radioactivity Levels and Their Corresponding External Exposure of Soil Samples from Tantalite Mining Areas in Oke-Ogun, South-Western Nigeria
Radioprotection 2012 DOI: 10.1051/radiopro/2012003 Vol. 47, n° 2, pages 243 à 252 Article Gamma radioactivity levels and their corresponding external exposure of soil samples from tantalite mining areas in Oke-Ogun, South-Western Nigeria A.K. ADEMOLA1, R.I. OBED2 (Manuscript received 9 September 2011, accepted 16 January 2012) Abstract The radioactivity concentrations of 226Ra, 232Th and 40K were measured using gamma-ray spectroscopy with NaI (Tl) detectors in four tantalite mining sites in the Oke-Ogun area, South-Western Nigeria. The measured values of the activities of 40K, 226Ra and 232Th in the soil samples were found to lie in the ranges 123.7 ± 3.8 – 1372.3 ± 8.6, 16.8 ± 1.6 – 71.1 ± 2.53 and 3.0 ± 0.7 – 31.9 ± 1.0 Bq kg–1, respectively. These samples were also found to have radium equivalent activity in the range 74.2–121.0 Bq kg-1. Values of 0.2–0.3 for the external and 0.3–0.4 for the internal hazard indices were estimated for the samples and the annual effective dose varied from 70.3 ± 13.5 to 100.8 ± 42.8 µSv with a mean of 87.5 ± 18.6 µSv y–1. The annual effective dose is higher than the world average. Keywords: Oke-Ogun / radionuclide / tantalite / natural radioactivity / effective dose 1. Introduction Human beings are exposed to background radiation that stems from both natural and man-made sources. Natural background radiation, which is equivalent to 2.4 mSv per person, makes up approximately 80% of the total radiation to which a person is exposed during one year (IAEA, 1996). -
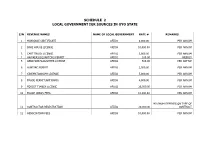
Schedule 2 Local Government Igr Sources in Oyo State
SCHEDULE 2 LOCAL GOVERNMENT IGR SOURCES IN OYO STATE S/N REVENUE NAMES NAME OF LOCAL GOVERNMENT RATE # REMARKS 1 MARRIAGE CERTIFICATE AFIJIO 8,000.00 PER ANNUM 2 BAKE HOUSE LICENSE AFIJIO 10,000.00 PER ANNUM 3 CART TRUCK LICENSE AFIJIO 3,000.00 PER ANNUM 4 HAWKERS/SQUARTORS PERMIT AFIJIO 100.00 WEEKLY 5 ABBATOIR/SLAUGHTER LICENSE AFIJIO 500.00 PER CATTLE 6 HUNTING PERMIT AFIJIO 2,500.00 PER ANNUM 7 CINEMATOGRAPH LICENSE AFIJIO 5,000.00 PER ANNUM 8 TRADE PERMIT(ARTISANS) AFIJIO 4,000.00 PER ANNUM 9 FOREST TIMBER LICENSE AFIJIO 25,000.00 PER ANNUM 10 TRADE UNION FEES AFIJIO 10,000.00 PER ANNUM MINIMUM DEPENDS ON TYPE OF 11 CONTRACTOR REGISTRATION AFIJIO 20,000.00 CONTRACT 12 ASSOCIATION FEES AFIJIO 10,000.00 PER ANNUM MINIMUM DEPENDS ON NATURE 13 TENDERS FEES AFIJIO 30,000.00 OF CONTRACT 14 DEATH REGISTRATION CERTIFICATE AFIJIO 2,500.00 PER CHILD 15 DEVELOPMENT LEVIES AFIJIO 200.00 PER ANNUM 16 PARKING FEES AFIJIO 200.00 DAILY 17 LOCAL GOVERNMENT IDENTIFICATION AFIJIO 2,500.00 18 PROCEED FROM SALES OF GOODS/FARM PRODUCES AFIJIO VARIES 19 SALES OF SCRAPS AFIJIO VARIES 20 EARNING FROM COMMERCIAL ACTIVITIES AFIJIO VARIES 21 EARNING FROM PARK AND GARDEN AFIJIO 500.00 PER PERSON 22 EARNING FROM GUEST HOUSE AFIJIO 10,000.00 PER ANNUM 23 POLLS TAX AFIJIO 1,000.00 PER ANNUM MINIMUN. DEPENDS ON 24 LIVESTOCK AFIJIO 1,000.00 PRODUCT 25 TENAMENT RATES AFIJIO 2,300.00 MINIMUN. DEPEND ONSIZE 26 BULL PERMIT AFIJIO 5,000.00 PER ANNUM 27 WHEEL BARROW FEES AFIJIO 50.00 DAILY 28 SHOP AND KIOSK FEES AFIJIO 200.00 PER MONTH 29 MARKET SQUATER AFIJIO 50.00 PER -

Report on Epidemiological Mapping of Schistosomiasis and Soil Transmitted Helminthiasis in 19 States and the FCT, Nigeria
Report on Epidemiological Mapping of Schistosomiasis and Soil Transmitted Helminthiasis in 19 States and the FCT, Nigeria. May, 2015 Report on Epidemiological Mapping of Schistosomiasis and Soil Transmitted Helminthiasis in 19 States and the FCT, Nigeria. ii TABLE OF CONTENTS LIST OF FIGURES ...................................................................................................................................... v LIST OF PLATES ...................................................................................................................................... vii FOREWORD .............................................................................................................................................. x EXECUTIVE SUMMARY ........................................................................................................................... xii 1.0 BACKGROUND ................................................................................................................................... 1 1.1 Introduction ................................................................................................................................... 1 1.2 Objectives of the Mapping Project ................................................................................................ 2 1.3 Justification for the Survey ............................................................................................................ 2 2.0. MAPPING METHODOLOGY ..............................................................................................................