1-Upper Limb.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Four Unusual Cases of Congenital Forelimb Malformations in Dogs
animals Article Four Unusual Cases of Congenital Forelimb Malformations in Dogs Simona Di Pietro 1 , Giuseppe Santi Rapisarda 2, Luca Cicero 3,* , Vito Angileri 4, Simona Morabito 5, Giovanni Cassata 3 and Francesco Macrì 1 1 Department of Veterinary Sciences, University of Messina, Viale Palatucci, 98168 Messina, Italy; [email protected] (S.D.P.); [email protected] (F.M.) 2 Department of Veterinary Prevention, Provincial Health Authority of Catania, 95030 Gravina di Catania, Italy; [email protected] 3 Institute Zooprofilattico Sperimentale of Sicily, Via G. Marinuzzi, 3, 90129 Palermo, Italy; [email protected] 4 Veterinary Practitioner, 91025 Marsala, Italy; [email protected] 5 Ospedale Veterinario I Portoni Rossi, Via Roma, 57/a, 40069 Zola Predosa (BO), Italy; [email protected] * Correspondence: [email protected] Simple Summary: Congenital limb defects are sporadically encountered in dogs during normal clinical practice. Literature concerning their diagnosis and management in canine species is poor. Sometimes, the diagnosis and description of congenital limb abnormalities are complicated by the concurrent presence of different malformations in the same limb and the lack of widely accepted classification schemes. In order to improve the knowledge about congenital limb anomalies in dogs, this report describes the clinical and radiographic findings in four dogs affected by unusual congenital forelimb defects, underlying also the importance of reviewing current terminology. Citation: Di Pietro, S.; Rapisarda, G.S.; Cicero, L.; Angileri, V.; Morabito, Abstract: Four dogs were presented with thoracic limb deformity. After clinical and radiographic S.; Cassata, G.; Macrì, F. Four Unusual examinations, a diagnosis of congenital malformations was performed for each of them. -

Shoulder Shoulder
SHOULDER SHOULDER ⦿ Connects arm to thorax ⦿ 3 joints ◼ Glenohumeral joint ◼ Acromioclavicular joint ◼ Sternoclavicular joint ⦿ https://www.youtube.com/watch?v=rRIz6oO A0Vs ⦿ Functional Areas ◼ scapulothoracic ◼ scapulohumeral SHOULDER MOVEMENTS ⦿ Global Shoulder ⦿ Arm (Shoulder Movement Joint) ◼ Elevation ◼ Flexion ◼ Depression ◼ Extension ◼ Abduction ◼ Abduction ◼ Adduction ◼ Adduction ◼ Medial Rotation ◼ Medial Rotation ◼ Lateral Rotation ◼ Lateral Rotation SHOULDER MOVEMENTS ⦿ Movement of shoulder can affect spine and rib cage ◼ Flexion of arm Extension of spine ◼ Extension of arm Flexion of spine ◼ Adduction of arm Ipsilateral sidebending of spine ◼ Abduction of arm Contralateral sidebending of spine ◼ Medial rotation of arm Rotation of spine ◼ Lateral rotation of arm Rotation of spine SHOULDER GIRDLE ⦿ Scapulae ⦿ Clavicles ⦿ Sternum ⦿ Provides mobile base for movement of arms CLAVICLE ⦿ Collarbone ⦿ Elongated S shaped bone ⦿ Articulates with Sternum through Manubrium ⦿ Articulates with Scapula through Acromion STERNOCLAVICULAR JOINT STERNOCLAVICULAR JOINT ⦿ Saddle Joint ◼ Between Manubrium and Clavicle ⦿ Movement ◼ Flexion - move forward ◼ Extension - move backward ◼ Elevation - move upward ◼ Depression - move downward ◼ Rotation ⦿ Usually movement happens with scapula Scapula Scapula ● Flat triangular bone ● 3 borders ○ Superior, Medial, Lateral ● 3 angles ○ Superior, Inferior, Lateral ● Processes and Spine ○ Acromion Process, Coracoid Process, Spine of Scapula ● Fossa ○ Supraspinous, Infraspinous, Subscapularis, Glenoid SCAPULA -

The Ossification of the Metacarpal and Phalangeal Bones in Human Foetuses
Folia Morphol. Vol. 63, No. 3, pp. 329–332 Copyright © 2004 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl The ossification of the metacarpal and phalangeal bones in human foetuses Florian Czerwiński1, Ewa Tomasik1, Małgorzata Tomasik2, Aldona Mahaczek-Kordowska1 1Department of Anatomy, Pomeranian Academy of Medicine, Szczecin, Poland 2Department of General Dentistry, Pomeranian Academy of Medicine, Szczecin, Poland [Received 4 November 2002; Revised 17 February 2004; Accepted 17 February 2004] An evaluation was made of the ossification level of the metacarpal and pha- langeal bones in human foetuses of both sexes from the 4th to the 9th month of gestation. Our results indicate that ossification of phalangeal bones 1 to 5 al- ways started at the distal end of the phalanx and endochondral ossification prevailed in the proximal phalanx of the thumb. Key words: human foetus, metacarpal bones, phalangeal bones, ossification INTRODUCTION Most human skeletal bones are ossified on a car- tilaginous base [5, 14]. This is a complex process pro- gressing dynamically in time and ossification consti- tutes the final phase of this complex process [3]. Thorough observation of the ossification of the foe- tal skeleton is made possible by means of the radio- logical method and evaluation of histological speci- mens [9]. This study presents the ossification of the metacarpal and phalangeal bones in human foetus- es at different stages of gestation. MATERIAL AND METHOD Eighty-six hands were examined taken from hu- man foetuses of both sexes aged from 4 to 9 months of gestation. -

Lecture 6 Comparative Anatomy of the Elbow and Forearm Functions Of
Lecture 6 Comparative anatomy of the Elbow and Forearm Functions of the Elbow in humans The set if the elbow allows for the hand to be placed in a position that makes it ideal for manipulation • Mostly non-weight supporting, and very important in throwing Bones Distal humerus- articulating parts Capitulum - Articulates with radial head - Almost half a sphere Trochlea - Like a pulleu - Articulates with trochlea notch of the ulna Distal humerus – non articulating parts Medial epicondyle - Blunt medial projection - Anterior surface has attachment for fore arm flexors Lateral epicondyle - Lateral non-articulating part - Attachment for forearm extensors on lateral part Distal humerus – fossae Olecranon fossa On posterior surface contains the olecranon of the ulna Coronoid fossa Anterior surface contains ulna coronoid process Radial fossa Shallow fossa anteriorly, contains the radius in flexion. Radius Proximal end Lateral bone in the forearm - Proximal end includes a head, neck and radial tuberosity - Head discoid and like a shallow cup, articulates with the capitulum - Neck is a constriction blew the head Distal end - Interosseous border for attachment of interosseous membrane - Styloid process sharp projection on lateral side of distal radius - Dorsal tubercle a large tuberosity on the posterior surface of the distal end. Ulna Proximal end - Olecranon hook like projection which enters the humeral olecranon fossa - Trochlea notch for articulation with the trochlea od the humerous - Coronoid process projects anteriorly distal to the olecranon - Radial notch – small oval depression on lateral side of coronoid process Distal end - Shaft sharp lateral border attachement foe Interosseous membrane - Styloid process on the distal end - Radial articulation distal rounded articulation that conforms to the ulna notch of the radius. -

Metacarpal Fractures: Practical Methods for Measurement of Shortening, Angulation, and Malrotation
J Orthop Spine Trauma. 2020 March; 6(1): 9-13. DOI: http://dx.doi.org/10.18502/jost.v6i1.4535 Educational Corner Metacarpal Fractures: Practical Methods for Measurement of Shortening, Angulation, and Malrotation Rohollah Khajeh 1, Behzad Enayati1, Farzad Vosughi2, Seyed Mohammad Javad Mortazavi 3,* 1 Fellowship of Hand Surgery, Joint Reconstruction Research Center, Tehran University of Medical Sciences, Tehran, Iran 2 Resident, Department of Orthopedics, Joint Reconstruction Research Center, Tehran University of Medical Sciences, Tehran, Iran 3 Professor, Department of Orthopedic Surgery, Joint Reconstruction Research Center, Tehran University of Medical Sciences, Tehran, Iran *Corresponding author: Seyed Mohammad Javad Mortazavi; Department of Orthopedic Surgery, Joint Reconstruction Research Center, Tehran University of Medical Sciences, Tehran, Iran. Tel: +98-2161192767, Email: [email protected] Received: 09 October 2019; Revised: 15 December 2019; Accepted: 17 January 2020 Keywords: Metacarpus; Fractures, Bone; Hand Deformities, Acquired Citation: Khajeh R, Enayati B, Vosughi F, Mortazavi SMJ. Metacarpal Fractures: Practical Methods for Measurement of Shortening, Angulation, and Malrotation. J Orthop Spine Trauma 2020; 6(1): 9-13. Background different metacarpal fractures. Articular fractures involving less than 20% of the joint Phalangeal, distal radius, and metacarpal fractures are surface and nondisplaced or minimally displaced shaft the most frequent upper limb fractures, respectively (1). fractures, without significant angulation, malrotation, or The incidence of metacarpal fractures in the United States shortening are treated with immobilization in the of America (USA) is 13.6 among every 100000 population intrinsic plus position (6). Bony apposition of at least 50% annually (2). Metacarpal fractures compose 30-40 percent and maximal bone shortening of 5 mm is acceptable. -

Arm and Cubital Fossa
Two Minute History M1 - Anatomy Dissection: • 300 B.C Arm and Cubital Alexandrian Egypt: King Ptolemy I, its ok Fossa to dissect cadavers of executed, mummies etc… •Herophilus “Father of Anatomy” accused by a rival of DG Simpson, Ph.D. dissecting 600 criminals…..live criminals VCU Department of Anatomy •1300 AD Europe Pope Boniface VIII edict to stop dissection to reduce the flow of bodies “parted out and boiled” from the crusades. Unclear if this is broad ban or very narrow. 1 2 Dissection: Dissection: •1540 parliament passes “The United Company of Barbers and •1700’s with the expansion of medical Surgeons, dissect 4-6 executed schools cadavers are used as tuition criminals/yr (not enough even then) •Competition is very high and medical •1600’s Britain. The executed are schools actively advertise that training includes dissections etc.. dissected in public as punishment • 1628 William Harvey •1828 London had 10 full time (cardiovascular fame). Autopsy & 200 part time body snatchers (“seasonal work” at 312 bodies/yr) of live and dead…. Medicine expands and shortages develop •Inventions to foil grave robbers Harvey dissects father and sister •1828 Robert Knox….and the rest • 1740’s Lots of private medical is amazing history. schools competing for students, William Hogarth The Reward of Cruelty 3 4 market forces develop 1750-1751 Dissection: •Burke was hanged: 25,000 watched. Hare was granted immunity as crowd called “Burke Hare” •1828, knock on the •Burke dissected: 30,000 came to see the open lab door, Knox’s assistant purchases a cadaver -
Bones of Upper Limb
BONES OF THE UPPER LIMB Dr. Jamila El-Medany OBJECTIVES At the end of the lecture, students should be able to: List the different bones of the UL. List the characteristic features of each bone. Differentiate between the bones of the right and left sides. List the articulations between the different bones. The Bones of UL are: Pectoral Girdle. Arm : Humerus. Forearm : Radius & Ulna. Wrist : Carpal bones Hand: Metacarpals & Phalanges Pectoral Girdle Formed of Two Bones: Clavicle (anteriorly) and Scapula (posteriorly). It is very light and allows the upper limb to have exceptionally free movement. Clavicle It is a doubly curved long bone lying horizontally across the root of the neck It is subcutaneous throughout its length. Functions: 1. It serves as a rigid support from which the scapula and free upper limb are suspended & keep them away from the trunk so that the arm has maximum freedom of movement. 2. Transmits forces from the upper limb to the axial skeleton. 3. Provides attachment for muscles. 4. It forms a boundary of the Cervicoaxillary canal for protection of the neurovascular bundle of the UL. Clavicle It is a long bone with no medullary cavity. It has the appearance of an elongated letter Capital (S) lying on one side. It has Two Ends: Medial (Sternal) : enlarged & triangular. Lateral (Acromial) : flattened. Body (shaft): Its medial 2/3 is convex forward. Its lateral 1/3 is concave forward. Surfaces: Superior : smooth as it lies just deep to the skin. Inferior : rough because strong ligaments bind it to the 1st rib. Articulations of Clavicle Medially with the manubrium at the Sternoclavicular joint . -

Macroanatomy of the Bones of Thoracic Limb of an Asian Elephant (Elephas Maximus)
Int. J. Morphol., 34(3):909-917, 2016. Macroanatomy of the Bones of Thoracic Limb of an Asian Elephant (Elephas maximus) Macroanatomía de los Huesos del Miembro Torácico de un Elefante Asiático (Elephas maximus) A. S. M. Lutful Ahasan*; Md. Abul Quasem*; Mohammad Lutfur Rahman*; Rubyath Binte Hasan*; A. S. M. Golam Kibria* & Subrata Kumar Shil* AHASAN, A. M. S. L.; QUASEM, M. A.; RAHMAN, M. L.; HASAN, R. B.; KIBRIA, A. S. M. G. & SHIL, S. K. Macroanatomy of the bones of thoracic limb of an Asian Elephant (Elephas maximus). Int. J. Morphol., 34(3):909-917, 2016. SUMMARY: Bones of forelimb were studied from a prepared skeleton of an adult female Asian elephant (Elephas maximus) in Anatomy Museum of Chittagong Veterinary and Animal Sciences University to understand the morphological form and structure of Asian elephant forelimb. The angle was approximately 123º between caudal border of scapula and caudal border of humerus. The scapula, humerus and bones of the antebrachium (particularly the ulna) were massive bones. The bones of manus were the short and relatively small. The dorsal border of scapula extended from the level of proximal extremity of first rib to the middle of the 6th rib. Ventral angle of scapula articulated with humerus by elongated shaped glenoid cavity (cavitas glenoidalis) of scapula and head of humerus (caput humeri). The major tubercle (tuberculum majus) of humerus was situated laterally to the head, which had smaller cranial part with large caudal part and extended cranially to the head. The crest of minor tubercle (tuberculum minus) was present as the rough line on the mediocaudal surface of humerus that ends in a slight depressed or elevated area, known as teres major tuberosity (tuberositas teres major). -
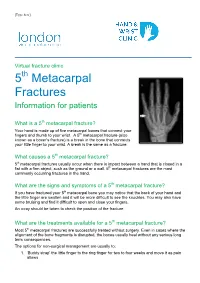
5Th Metacarpal Fractures Information for Patients
[Type here] Virtual fracture clinic 5th Metacarpal Fractures Information for patients What is a 5th metacarpal fracture? Your hand is made up of five metacarpal bones that connect your fingers and thumb to your wrist. A 5th metacarpal fracture (also known as a boxer’s fracture) is a break in the bone that connects your little finger to your wrist. A break is the same as a fracture. What causes a 5th metacarpal fracture? 5th metacarpal fractures usually occur when there is impact between a hand that is closed in a fist with a firm object, such as the ground or a wall. 5th metacarpal fractures are the most commonly occurring fractures in the hand. What are the signs and symptoms of a 5th metacarpal fracture? If you have fractured your 5th metacarpal bone you may notice that the back of your hand and the little finger are swollen and it will be more difficult to see the knuckles. You may also have some bruising and find it difficult to open and close your fingers. An x-ray should be taken to check the position of the fracture. What are the treatments available for a 5th metacarpal fracture? Most 5th metacarpal fractures are successfully treated without surgery. Even in cases where the alignment of the bone fragments is disrupted, the bones usually heal without any serious long term consequences. The options for non-surgical management are usually to: 1. ‘Buddy strap’ the little finger to the ring finger for two to four weeks and move it as pain allows 2. -

Wing Injuries
Wing Injuries Kimberly A McMunn MS MPH DVM – Anatomy Review – Radiological Positioning – Patient Evaluation – Approaches to Fracture Management – Physical Therapy – Monitoring Healing – Complications – Treatments for Specific Injuries Anatomy of the Wing Proctor and Lynch 1993 Wing Musculature- Ventral Proctor and Lynch 1993 Wing Musculature- Dorsal Proctor and Lynch 1993 Wing Musculature- Flight Proctor and Lynch 1993 Flight bones Scott 2016 Wing Vasculature Proctor and Lynch 1993 Bird bones vs mammal bones – Bone cortices thin and brittle but very strong, with high calcium content – Any defect in wall greatly reduces their strength – Less holding power (compared to mammals) for fixation hardware – Limited soft tissue over many long bones, very thin skin, bone fragments exteriorize easily Bird bones vs mammal bones – Pneumatic bones- humerus, and ulna in some species (Pelicans and CA condors) – Majority of callus tissue in healing is derived from the periosteal surface, and blood supply to the periosteum from surrounding soft tissues is very important. The IM circulation appears to be of less significance in avian bone healing than in mammals Radiographic Positioning 2 Orthogonal Views!! Scott 2016 Evaluation of the Patient – Evaluate signalment, history, and physical and orthopedic exams – Hands-off observation for mentation, posture, respiration and general appearance – Consider anesthesia or sedation for exam – Consider co-morbidities, including eye, head or intracoelomic trauma in wild birds, or malnutrition and associated poor bone -

Anatomical Features of Some Bones of the Forelimbs of Lions (Panthera Leo)
Int. J. Morphol., 39(2):378-385, 2021. Anatomical Features of Some Bones of the Forelimbs of Lions (Panthera leo) Características Anatómicas de Algunos Huesos de los Miembros Torácicos de Leones (Panthera leo) Md. Shahriar Hasan Sohel1; Kh. Nurul Islam2 & Mohammad Lutfur Rahman2 SOHEL, M. S. H.; ISLAM, K. N. & RAHMAN, M. L. Anatomical features of some bones of the forelimbs of lions (Panthera leo). Int. J. Morphol., 39(2):378-385, 2021. SUMMARY: We studied the bones of forelimb of four adult lions (Panthera leo) of both sexes to record the gross anatomical and morphometrical features of the scapula, humerus, radius and ulna. We observed some unique anatomical features that will be helpful for radiographic interpretation and forensic investigations. The lateral surface of scapula was unequally divided into supraspinous (fossa supraspinata) and infraspinous fossa (fossa infraspinata) by a well developed spine (spina scapulae). The acromion process was subdivided into suprahamate process (processus suprahamatus)and hamate process (processus hamatus); the later one was over hanged the glenoid cavity (cavitas glenoidalis), but the supraglenoid tubercle (tuberculum supraglenoidalis) was absent. The shaft (diaphysis) of humerus was compressed craniocaudally in proximal part, rounded to oval in middle part and compressed mediolaterally in distal part. A long, narrow supracondyloid foramen was found at distal limb just above the medial epicondyle (epicondylus medialis) which didn’t connect the radial fossa (fossa radialis) with the olecranon fossa (fossa olecrani). The radius and ulna were twin bones where radius was articulated craniolateral to the ulna proximally and craniomedial to the ulna distally. However, the ulna was the longest bone in the forelimb of lion.