Lecture 6 Comparative Anatomy of the Elbow and Forearm Functions Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Shoulder Shoulder
SHOULDER SHOULDER ⦿ Connects arm to thorax ⦿ 3 joints ◼ Glenohumeral joint ◼ Acromioclavicular joint ◼ Sternoclavicular joint ⦿ https://www.youtube.com/watch?v=rRIz6oO A0Vs ⦿ Functional Areas ◼ scapulothoracic ◼ scapulohumeral SHOULDER MOVEMENTS ⦿ Global Shoulder ⦿ Arm (Shoulder Movement Joint) ◼ Elevation ◼ Flexion ◼ Depression ◼ Extension ◼ Abduction ◼ Abduction ◼ Adduction ◼ Adduction ◼ Medial Rotation ◼ Medial Rotation ◼ Lateral Rotation ◼ Lateral Rotation SHOULDER MOVEMENTS ⦿ Movement of shoulder can affect spine and rib cage ◼ Flexion of arm Extension of spine ◼ Extension of arm Flexion of spine ◼ Adduction of arm Ipsilateral sidebending of spine ◼ Abduction of arm Contralateral sidebending of spine ◼ Medial rotation of arm Rotation of spine ◼ Lateral rotation of arm Rotation of spine SHOULDER GIRDLE ⦿ Scapulae ⦿ Clavicles ⦿ Sternum ⦿ Provides mobile base for movement of arms CLAVICLE ⦿ Collarbone ⦿ Elongated S shaped bone ⦿ Articulates with Sternum through Manubrium ⦿ Articulates with Scapula through Acromion STERNOCLAVICULAR JOINT STERNOCLAVICULAR JOINT ⦿ Saddle Joint ◼ Between Manubrium and Clavicle ⦿ Movement ◼ Flexion - move forward ◼ Extension - move backward ◼ Elevation - move upward ◼ Depression - move downward ◼ Rotation ⦿ Usually movement happens with scapula Scapula Scapula ● Flat triangular bone ● 3 borders ○ Superior, Medial, Lateral ● 3 angles ○ Superior, Inferior, Lateral ● Processes and Spine ○ Acromion Process, Coracoid Process, Spine of Scapula ● Fossa ○ Supraspinous, Infraspinous, Subscapularis, Glenoid SCAPULA -

A STUDY of MORPHOLOGY and MORPHOMETRY of PROXIMAL END of DRY RADIUS BONES with ITS CLINICAL IMPLICATIONS Suraj Ethiraj 1, Jyothi K C *2, Shailaja Shetty 3
International Journal of Anatomy and Research, Int J Anat Res 2019, Vol 7(3.1):6712-16. ISSN 2321-4287 Original Research Article DOI: https://dx.doi.org/10.16965/ijar.2019.203 A STUDY OF MORPHOLOGY AND MORPHOMETRY OF PROXIMAL END OF DRY RADIUS BONES WITH ITS CLINICAL IMPLICATIONS Suraj Ethiraj 1, Jyothi K C *2, Shailaja Shetty 3. 1 Final year MBBS, M S Ramaiah Medical College, Bangalore, Karnataka, India. 2 Assistant Professor, Department of Anatomy, M S Ramaiah Medical College, Bangalore, Karnataka, India. 3 Professor & HOD, Department of Anatomy, M S Ramaiah Medical College, Bangalore, Karnataka, India. ABSTRACT Background: Fracture of the radial head constitute 1/3rd of all the elbow fractures. It occurs as a result of a fall on an outstretched hand or a direct blow to the lateral aspect of elbow joint. This is now becoming more common due to pre existing co-morbidities like osteoporosis and chronic osteoarthritis. Surgical correction of the comminuted fractures of radial head involves reconstruction or replacement with artificial radial head prosthesis in cases where reconstruction is not possible. Aims and Objectives: To analyze the morphometric details of proximal end of radius and to describe the morphological features of head and bicipital tuberosity of the radius. Materials & Methodology: Sixty dry human adult radius bones of unknown age and sex were assessed for morphometric and morphological characters. Vernier caliper was used to measure the various parameters on the proximal ends of radius bones. The data was tabulated and analyzed using SPSS software. Results: The mean length of radius was found to be 23.98 cm. -

Arm and Cubital Fossa
Two Minute History M1 - Anatomy Dissection: • 300 B.C Arm and Cubital Alexandrian Egypt: King Ptolemy I, its ok Fossa to dissect cadavers of executed, mummies etc… •Herophilus “Father of Anatomy” accused by a rival of DG Simpson, Ph.D. dissecting 600 criminals…..live criminals VCU Department of Anatomy •1300 AD Europe Pope Boniface VIII edict to stop dissection to reduce the flow of bodies “parted out and boiled” from the crusades. Unclear if this is broad ban or very narrow. 1 2 Dissection: Dissection: •1540 parliament passes “The United Company of Barbers and •1700’s with the expansion of medical Surgeons, dissect 4-6 executed schools cadavers are used as tuition criminals/yr (not enough even then) •Competition is very high and medical •1600’s Britain. The executed are schools actively advertise that training includes dissections etc.. dissected in public as punishment • 1628 William Harvey •1828 London had 10 full time (cardiovascular fame). Autopsy & 200 part time body snatchers (“seasonal work” at 312 bodies/yr) of live and dead…. Medicine expands and shortages develop •Inventions to foil grave robbers Harvey dissects father and sister •1828 Robert Knox….and the rest • 1740’s Lots of private medical is amazing history. schools competing for students, William Hogarth The Reward of Cruelty 3 4 market forces develop 1750-1751 Dissection: •Burke was hanged: 25,000 watched. Hare was granted immunity as crowd called “Burke Hare” •1828, knock on the •Burke dissected: 30,000 came to see the open lab door, Knox’s assistant purchases a cadaver -
Bones of Upper Limb
BONES OF THE UPPER LIMB Dr. Jamila El-Medany OBJECTIVES At the end of the lecture, students should be able to: List the different bones of the UL. List the characteristic features of each bone. Differentiate between the bones of the right and left sides. List the articulations between the different bones. The Bones of UL are: Pectoral Girdle. Arm : Humerus. Forearm : Radius & Ulna. Wrist : Carpal bones Hand: Metacarpals & Phalanges Pectoral Girdle Formed of Two Bones: Clavicle (anteriorly) and Scapula (posteriorly). It is very light and allows the upper limb to have exceptionally free movement. Clavicle It is a doubly curved long bone lying horizontally across the root of the neck It is subcutaneous throughout its length. Functions: 1. It serves as a rigid support from which the scapula and free upper limb are suspended & keep them away from the trunk so that the arm has maximum freedom of movement. 2. Transmits forces from the upper limb to the axial skeleton. 3. Provides attachment for muscles. 4. It forms a boundary of the Cervicoaxillary canal for protection of the neurovascular bundle of the UL. Clavicle It is a long bone with no medullary cavity. It has the appearance of an elongated letter Capital (S) lying on one side. It has Two Ends: Medial (Sternal) : enlarged & triangular. Lateral (Acromial) : flattened. Body (shaft): Its medial 2/3 is convex forward. Its lateral 1/3 is concave forward. Surfaces: Superior : smooth as it lies just deep to the skin. Inferior : rough because strong ligaments bind it to the 1st rib. Articulations of Clavicle Medially with the manubrium at the Sternoclavicular joint . -

Anatomical Features of Some Bones of the Forelimbs of Lions (Panthera Leo)
Int. J. Morphol., 39(2):378-385, 2021. Anatomical Features of Some Bones of the Forelimbs of Lions (Panthera leo) Características Anatómicas de Algunos Huesos de los Miembros Torácicos de Leones (Panthera leo) Md. Shahriar Hasan Sohel1; Kh. Nurul Islam2 & Mohammad Lutfur Rahman2 SOHEL, M. S. H.; ISLAM, K. N. & RAHMAN, M. L. Anatomical features of some bones of the forelimbs of lions (Panthera leo). Int. J. Morphol., 39(2):378-385, 2021. SUMMARY: We studied the bones of forelimb of four adult lions (Panthera leo) of both sexes to record the gross anatomical and morphometrical features of the scapula, humerus, radius and ulna. We observed some unique anatomical features that will be helpful for radiographic interpretation and forensic investigations. The lateral surface of scapula was unequally divided into supraspinous (fossa supraspinata) and infraspinous fossa (fossa infraspinata) by a well developed spine (spina scapulae). The acromion process was subdivided into suprahamate process (processus suprahamatus)and hamate process (processus hamatus); the later one was over hanged the glenoid cavity (cavitas glenoidalis), but the supraglenoid tubercle (tuberculum supraglenoidalis) was absent. The shaft (diaphysis) of humerus was compressed craniocaudally in proximal part, rounded to oval in middle part and compressed mediolaterally in distal part. A long, narrow supracondyloid foramen was found at distal limb just above the medial epicondyle (epicondylus medialis) which didn’t connect the radial fossa (fossa radialis) with the olecranon fossa (fossa olecrani). The radius and ulna were twin bones where radius was articulated craniolateral to the ulna proximally and craniomedial to the ulna distally. However, the ulna was the longest bone in the forelimb of lion. -

The Ulna Humerus and Ulna: Landmarks and Articulations
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. The Ulna o the ulna is a medial long bone, the longer of the two in the forearm. Proximally, it articulates with the capitulum and trochlea of the humerus; . At the radial notch, it articulates with the head of radius o It stabilizes the forearm o The HEAD LIES DISTALLY. The Olecranon The Trochlear Notch The Coronoid Process The Radial Notch where the head of the radius goes The Tuberosity of the Ulna is where the Brachialis attaches The deep part of Supinator fossa the supinator Supinator crest attaches here Bony features include: - Olecranon - Trochlear notch - Coronoid process - Radial notch - Tuberosity of ulna - Supinator fosa - Supinator crest - Head of ulna - Ulnar styloid process The head of ulna The ulnar styloid process Humerus and ulna: landmarks and articulations o the humerus is a long bone, the largest in the upper limb o it articulates proximally with the scapula at the scapulohumeral (glenohumeral) joint o it articulates distally with the ulna at the elbow joint o the ulna and humerus articulate at the elbow joint o the articulations include: . articulation between the trochlea of the humerus and the trochlear notch of the ulna . articulation of the olecranon process and the olecranon fossa during extension . articulation of the coronoid process and the coronoid fossa during flexion o the surface landmarks include . the medial and lateral epicondyle . the olecranon . the posterior border of the ulna . -
Lab Manual Appendicular Skele
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the appendicular skeleton, which is formed from the pectoral and pelvic girdles and the upper and lower limbs. View Module 7.2 Axial and Appendicular Skeleton to highlight the bones of the appendicular skeleton and compare them to those of the axial skeleton. Examine Module 11.1 Appendicular Skeleton to view only the bones of the appendicular skeleton. In addition to learning about all the bones of the appendicular skeleton, it is also important to identify some significant bone markings. Bone markings can have many shapes, including holes, round or sharp projections, and shallow or deep valleys, among others. These markings on the bones serve many purposes, including forming attachments to other bones or muscles and allowing passage of a blood vessel or nerve. It is helpful to understand the meanings of some of the more common bone marking terms. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure: Foramen: (see Module 10.18 Foramina of Skull) Fossa: Margin: Process: Proximal: Trochanter: Tubercle: Tuberosity: Throughout this exercise, you will notice bold terms. This is meant to focus your attention on these important words. Make sure you pay attention to any bold words and know how to explain their definitions and/or where they are located. Use the following modules to guide your exploration of the appendicular skeleton. As you explore these bones in Visible Body’s app, also locate the bones and bone markings on any available charts, models, or specimens. -
Bones of the Upper Limb
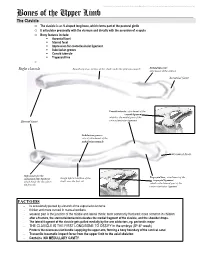
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. Bones of the Upper Limb The Clavicle o The clavicle is an S-shaped long bone, which forms part of the pectoral girdle o It articulates proximally with the sternum and distally with the acromion of scapula o Bony features include: . Acromial facet . Sternal facet . Impression for costoclavicular ligament . Subclavian groove . Conoid tubercle . Trapezoid line o Right clavicle Smooth superior surface of the shaft, under the platysma muscle Deltoid tubercle: attachment of the deltoid Acromial facet Conoid tubercle, attachment of the conoid ligament which is the medial part of the Sternal facet coracoclavicular ligament Subclavian groove: site of attachment of the subclavius muscle Acromial facet Impression for the Trapezoid line, attachment of the costoclavicular ligament Rough inferior surface of the trapezoid ligament which binds the clavicle to shaft, over the first rib which is the lateral part of the the first rib coracoclavicular ligament FACTOIDS - Its occasionally pierced by a branch of the supraclavicular nerve - thicker and more curved in manual workers - weakest part is the junction of the middle and lateral thirds: most commonly fractured; more common in children - after a fracture, the sternocleidomastoid elevates the medial fragment of the clavicle, and the shoulder drops. - The lateral fragment of the clavicle gets pulled medially by the arm adductors, eg. pectoralis major - THE CLAVICLE IS THE FIRST LONG BONE TO OSSIFY in the embryo (5th-6th week) - Protects the neurovascular bundle supplying the upper arm, forming a bony boundary of the cervical canal - Transmits traumatic impact force from the upper limb to the axial skeleton - Contains NO MEDULLARY CAVITY - This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. -

Lecture (7) Arm and Elbow.Pdf
Arm and elbow Musculoskeletal block- Anatomy-lecture 7 Editing file Color guide : Objectives Only in boys slides in Blue Only in girls slides in Purple ✓ Describe the attachments, actions and innervations of: important in Red a. Biceps brachii Doctor note in Green b. Coracobrachialis Extra information in Grey c. Brachialis d. Triceps brachii ✓ Define the boundaries of the cubital fossa and enumerate its contents. ✓ Demonstrate the following features of the elbow joint: a. Articulating bones b. Capsule c. Lateral & medial collateral ligaments d. Synovial membrane ✓ Demonstrate the movements; flexion and extension of the elbow. ✓ List the main muscles producing the above movements. ✓ Define the boundaries of the cubital fossa and enumerate its contents. Shoulder THE ARM: Posterior Anterior An aponeurotic sheet separating various view muscles of the upper limbs, including lateral A R M R A view and medial humeral septa. Elbow - The lateral and medial intermuscular septa Arm Humerus divide the distal part of the arm into two compartments Lateral Medial intermuscular intermuscular septum septum Neurovascular skin Anterior Posterior bundle (flexor compartment) (extensor compartment) Fascia Humerus 1-Anterior Fascial Compartment: Note: the radial and ulnar nerves begin in the anterior compartment then pierce the intermuscular septum and enter the posterior compartment Radial Brachialis Ulnar Median Biceps Basilic vein brachii Brachial Musculocutaneous artery Coracobrachialis 2. Blood 3. Nerves 1. muscles vessels Muscles Of Anterior Compartment Muscles Biceps Brachii Coracobrachialis Brachialis -Long Head (lateral head) from supraglenoid tubercle of Tip of the coracoid Origin scapula (intracapsular) process of scapula (with Front of the lower half -Short Head from the tip of coracoid process of scapula short head of biceps of humerus -The two heads join in the middle of the arm brachii) -Into the posterior part of the radial tuberosity. -

Radial Head Dislocation and Subluxation in Osteogenesis Imperfecta
2694 COPYRIGHT Ó 2007 BY THE JOURNAL OF BONE AND JOINT SURGERY,INCORPORATED Radial Head Dislocation and Subluxation in Osteogenesis Imperfecta By Alice Marcdargent Fassier, MD, Frank Rauch, MD, Mehdi Aarabi, MD, Chantal Janelle, MD, FRCS, and Francxois Fassier, MD, FRCS Investigation performed at Shriners Hospital, Montreal, Quebec, Canada Background: Upper limb deformity in children with osteogenesis imperfecta may substantially impair function. The aims of this retrospective work were to study the prevalence of radial head malalignment (dislocation or subluxation) in different types of osteogenesis imperfecta and to identify factors linked to it. Methods: We assessed 489 upper limbs from 254 patients (with a mean age of 9.6 years and including 130 female patients) who had various types of osteogenesis imperfecta. Radiographs representing a single time-point for each patient were assessed for the presence and direction of radial head malalignment and associated abnormalities (dysplasia of the capitellum or of the radial head or neck, calcification of the interosseous mem- brane, or radioulnar synostosis). Deformations of the humerus, radius, and ulna were assessed with regard to location, direction, and magnitude. The forearm range of motion in pronation and supination and the hand grip force were measured in a subset of patients. Results: We observed radial head dislocation or subluxation in forty-four and thirty-nine upper extremities, respec- tively. The frequency of radial head malalignment was significantly higher in type-V osteogenesis imperfecta (86%) than in the other types (0% to 29%) (p < 0.001). Dysplasia of the humeral capitellum, radial head, or radial neck was associated with malalignment in all types of osteogenesis imperfecta, with the exception of capitellum dys- plasia in type V. -
Antebrachium, Hand, and Joints
LABORATORY Antebrachium, Hand, 5 and Joints ELBOW JOINT Classify the elbow joint according to structural and functional criteria – Hinge, synovial (diarthrotic) joint Identify the bony articulations. Humeroradial: (radial collateral) capitulum of humerus articulates with the head of the radius Humeroulnar: (ulnar collateral) trochlea of humerus articulates with the trochlear notch of the ulna olecranon process of the ulna articulates with the olecranon fossa of the humerus Proximal radioulnar: Head of radius articulates with the radial notch of the ulna Held in place by the annular ligament Identify the ligaments associated with the elbow joint. radial collateral ligament ulnar collateral ligament annular ligament Identify the primary sources of vascularization to the elbow joint. superior/inferior ulnar collateral arteries anterior/posterior interosseous arteries Identify the primary innervation sources to the elbow and radioulnar joints. Elbow – musculocutaneous, radial, ulnar nerves Radioulnar – musculocutaneous, median, radial nerves 28 Laboratory 5 • Antebrachium, Hand, and Joints Identify the structures associated with the cubital fossa. brachial artery median nerve median cubital vein biceps brachii tendon Discuss the venous return from the brachial region. cephalic vein basilic vein median cubital vein axillary vein RADIOULNAR JOINTS Proximal radioulnar: Head of radius articulates with the radial notch of the ulna Distal radioulnar: Head of the ulna articulates with the ulnar notch on the radius Allows radius to move anteriorly across the ulna during pronation Classify the radioulnar joints according to structural and functional criteria, and identify the associated ligaments. Proximal – pivot, synovial diarthrotic joint Distal – pivot, synovial diarthrotic joint annular ligament triangular ligament (articular disc) radial/ulnar collateral ligaments (fibrocartilage complex) radial/ulnar collateral ligaments WRIST JOINT Classify the wrist joint according to structural and functional criteria – diarthrotic, synovial condyloid.