Post-Streptococcal Acute Glomerulonephritis in Children: Clinical Features and Pathogenesis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Renal Biopsy in Children with Nephrotic Syndrome at Tripoli Children Hospital
RESULTS OF RENAL BIOPSY IN CHILDREN WITH NEPHROTIC SYNDROME AT TRIPOLI CHILDREN HOSPITAL Naziha R. Rhuma1, Mabruka Ahmed Zletni1, Mohamed Turki1, Omar Ahmed Fituri1, Awatif. El Boeshi2 1- Faculty of medicine, University of Tripoli, Libya. 2- Nephrology Unit, Children Hospital of Tripoli, Libya. ABSTRACT Nephrotic syndrome is an important renal disorder in children. The role of renal biopsy in children with nephrotic syndrome is controversial, especially in children with frequent relapses or steroid-dependent nephrotic syndrome. The aims of this study are to verify indications of renal biopsy in children with nephrotic syndrome, to identify pat- terns of glomerular disease and its corresponding outcomes. This is a descriptive study reviewed retrospectively a 25 renal biopsies from children with nephrotic syndrome who followed up in nephrology unit at Tripoli Children Hos- pital from Jun. 1995 to Jan. 2006. Children with either steroid resistant or steroid dependent who underwent renal biopsy were included. Twenty five of children (14 male and 11 female) with nephrotic syndrome were included. The mean age 5.2±4.6years (range was from 1-14 years). 14(56%) children were steroid resistant and 11(44%) children were steroid dependent. Minimal-change disease (MCD) accounted for 12(48%) children, focal and segmental scle- rosis (FSGS) was accounted for 10(40%) children and 3(12%) children accounted for other histopathological types. 7(87.5%) of children with FSGS had progressed to end stage renal disease. Steroid resistant was the main indication for renal biopsy in children with nephrotic syndrome. There was increased frequency of FSGS nephrotic syndrome among children with steroid resistant type with poor outcomes. -

Glomerulonephritis Management in General Practice
Renal disease • THEME Glomerulonephritis Management in general practice Nicole M Isbel MBBS, FRACP, is Consultant Nephrologist, Princess Alexandra lomerular disease remains an important cause Hospital, Brisbane, BACKGROUND Glomerulonephritis (GN) is an G and Senior Lecturer in important cause of both acute and chronic kidney of renal impairment (and is the commonest cause Medicine, University disease, however the diagnosis can be difficult of end stage kidney disease [ESKD] in Australia).1 of Queensland. nikky_ due to the variability of presenting features. Early diagnosis is essential as intervention can make [email protected] a significant impact on improving patient outcomes. OBJECTIVE This article aims to develop However, presentation can be variable – from indolent a structured approach to the investigation of patients with markers of kidney disease, and and asymptomatic to explosive with rapid loss of kidney promote the recognition of patients who need function. Pathology may be localised to the kidney or further assessment. Consideration is given to the part of a systemic illness. Therefore diagnosis involves importance of general measures required in the a systematic approach using a combination of clinical care of patients with GN. features, directed laboratory and radiological testing, DISCUSSION Glomerulonephritis is not an and in many (but not all) cases, a kidney biopsy to everyday presentation, however recognition establish the histological diagnosis. Management of and appropriate management is important to glomerulonephritis (GN) involves specific therapies prevent loss of kidney function. Disease specific directed at the underlying, often immunological cause treatment of GN may require specialist care, of the disease and more general strategies aimed at however much of the management involves delaying progression of kidney impairment. -

Childhood Nephrotic Syndrome -A Single Centre Experience in Althawra Central Hospital, Albaida- Libya During 2005-2016
MOJ Surgery Case Report Open Access Childhood nephrotic syndrome -a single centre experience in Althawra central hospital, Albaida- Libya during 2005-2016 Abstract Volume 6 Issue 6 - 2018 The aim of this study is to determine response to treatment in terms of remission Mabrouka A M Bofarraj,1 Fatma S Ben and relapse, related risk factors, type of management and complications of nephrotic 2 1 syndrome among studied patients. Khaial, Najwa H Abduljawad, Rima Alshowbki1 Design: Retrospective, analytical study. 1Department of Pediatric Medicine, Al Thawra Central Teaching Hospital, Libya Setting: Pediatric nephrology clinic at Althawra Central Teaching Hospital-Albida, 2Department of Family and Community Medicine, Faculty of Participants/patients: All patients with idiopathic nephrotic syndrome (INS) were Medicine, Benghazi University, Libya evaluated during 2005- 2016. Patients divided into two groups, group I 46 (39%) is non-relapse and group II 72 (62.7%) is relapse group. Group II are sub divided into Correspondence: Mabrouka A M Bofarraj, Department of group A: frequent relapse steroid dependent (FRNS/SDNS) and group B: infrequent Pediatric Medicine, Al Thawra Central Teaching Hospital, Faculty relapse nephrotic syndrome (IRNS). of medicine, Omar Al Moukhtar University, Albaida-Libya, Tel 00218927445625, Email Results: Records of 118 children with INS were studied and 74 (62.7%) were boys, male to female ratio 1.7:1. There was no significance difference between group I and Received: October 24, 2018 | Published: November 23, 2018 group II in the following parameters; age group, sex, family history, initial hypertension and hematuria (p value = >0.05). Mean proteinuria was significantly higher in group II (p=0.001), while mean S. -

Diffuse Proliferative Glomerulonephritis and Acute Renal Failure Associated with Acute Staphylococcal Osteomyelitis
Diffuse Proliferative Glomerulonephritis and Acute Renal Failure Associated with Acute Staphylococcal Osteomyelitis MATTHEW D. GRIFFIN,* JOHANNES BJORNSSON,t and STEPHEN B. ERICKSON* *Department of Internal Medicine, Division of Nephrology, and tDepartment of Pathology, Mayo Clinic and Mayo Foundation, Rochester, Minnesota. Abstract. A 72-year-old man developed acute renal failure after peated surgical debridement. Spontaneous recovery of renal coronary bypass surgery that had been complicated by sternal function occurred after eradication of infection and final sur- osteomyelitis caused by the Staphylococcus aureus bacterium. gical wound repair. The relationship between acute bacterial Bacteremia and sepsis were not present. Renal biopsy demon- infections and glomerulonephritis and, in particular, the causal strated a florid, diffuse, proliferative glomerulonephritis with role of staphylococcal antigens in the pathogenesis of such glomerular immune complex deposition. Management in- lesions is discussed. (J Am Soc Nephrol 8: 1633-1639, 1997) cluded hemodialysis, prolonged antibiotic therapy, and re- Coagulase-positive staphylococcus (Staphylococcus aureus) is mg/dl]) and in the immediate postoperative period. Over the the most common causative organism in acute osteomyelitis following days, the patient’s serum creatinine concentration (1). Along with coagulase-negative staphylococcal species, it increased progressively, and hemodialysis was instituted on has also been implicated in the pathogenesis of immune com- day 23 after CABG. There was no past or family history of plex (IC)-mediated diffuse proliferative glomerulonephritis renal disease and no known drug allergies. Prior medical (DPGN) in a variety of infections. These include bacterial history had included degenerative disc disease, stable abdom- endocarditis, ventriculoatrial shunt infections, pneumonia, and inal aortic aneurysm, stable benign prostatic hyperplasia, and visceral abscesses with or without septicemia (2-6). -

ICD-10 International Statistical Classification of Diseases and Related Health Problems
ICD-10 International Statistical Classification of Diseases and Related Health Problems 10th Revision Volume 2 Instruction manual 2010 Edition WHO Library Cataloguing-in-Publication Data International statistical classification of diseases and related health problems. - 10th revision, edition 2010. 3 v. Contents: v. 1. Tabular list – v. 2. Instruction manual – v. 3. Alphabetical index. 1.Diseases - classification. 2.Classification. 3.Manuals. I.World Health Organization. II.ICD-10. ISBN 978 92 4 154834 2 (NLM classification: WB 15) © World Health Organization 2011 All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO web site (http://www.who.int/about/licensing/copyright_form). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. -

Pathogenesis of Human Systemic Lupus Erythematosus: a Cellular Perspective Vaishali R
Feature Review Pathogenesis of Human Systemic Lupus Erythematosus: A Cellular Perspective Vaishali R. Moulton,1,* Abel Suarez-Fueyo,1 Esra Meidan,1,2 Hao Li,1 Masayuki Mizui,3 and George C. Tsokos1,* Systemic lupus erythematosus (SLE) is a chronic autoimmune disease affecting Trends multiple organs. A complex interaction of genetics, environment, and hormones Recent work has identified patterns of leads to immune dysregulation and breakdown of tolerance to self-antigens, altered gene expression denoting resulting in autoantibody production, inflammation, and destruction of end- molecular pathways operating in organs. Emerging evidence on the role of these factors has increased our groups of SLE patients. knowledge of this complex disease, guiding therapeutic strategies and identi- Studies have identified local, organ- fying putative biomarkers. Recent findings include the characterization of specific factors enabling or ameliorat- ing SLE tissue damage, thereby dis- genetic/epigenetic factors linked to SLE, as well as cellular effectors. Novel sociating autoimmunity and end-organ observations have provided an improved understanding of the contribution of damage. tissue-specific factors and associated damage, T and B lymphocytes, as well Novel subsets of adaptive immune as innate immune cell subsets and their corresponding abnormalities. The effectors, and the contributions of intricate web of involved factors and pathways dictates the adoption of tailored innate immune cells including platelets therapeutic approaches to conquer this disease. and neutrophils, are being increasingly recognized in lupus pathogenesis. Studies have revealed metabolic cellu- SLE, a Devastating Disease for Young Women lar aberrations, which underwrite cell SLE afflicts mostly women [1] in which the autoimmune response is directed against practically and organ injury, as important contri- all organs, leading to protean clinical manifestations including arthritis, skin disease, blood cell butors to lupus disease. -

Glomerulonephritis
Adolesc Med 16 (2005) 67–85 Glomerulonephritis Keith K. Lau, MDa,b, Robert J. Wyatt, MD, MSa,b,* aDivision of Pediatric Nephrology, Department of Pediatrics, University of Tennessee Health Sciences Center, Room 301, WPT, 50 North Dunlap, Memphis, TN 38103, USA bChildren’s Foundation Research Center at the Le Bonheur Children’s Medical Center, Room 301, WPT, 50 North Dunlap, Memphis, TN 38103, USA Early diagnosis of glomerulonephritis (GN) in the adolescent is important in initiating appropriate treatment and controlling chronic glomerular injury that may eventually lead to end-stage renal disease (ESRD). The spectrum of GN in adolescents is more similar to that seen in young and middle-aged adults than to that observed in prepubertal children. In this article, the authors discuss the clinical features associated with GN and the diagnostic evaluation required to determine the specific type of GN. With the exception of hereditary nephritis (Alport’s disease), virtually all types of GN are immunologically mediated with glomerular deposition of immunoglobulins and complement proteins. The inflammatory events leading to GN may be triggered by a number of factors. Most commonly, immune complexes deposit in the glomeruli or are formed in situ with the antigen as a structural component of the glomerulus. The immune complexes then initiate the production of proinflammatory mediators, such as complement proteins and cytokines. Subsequently, the processes of sclerosis within the glomeruli and fibrosis in the tubulointerstitial cells lead to chronic or even irreversible renal injury [1]. Less commonly, these processes occur without involvement of immune complexes—so-called ‘‘pauci-immune GN.’’ * Corresponding author. -

Acute Poststreptococcal Glomerulonephritis: Immune Deposit Disease
Acute poststreptococcal glomerulonephritis: immune deposit disease. A F Michael Jr, … , R A Good, R L Vernier J Clin Invest. 1966;45(2):237-248. https://doi.org/10.1172/JCI105336. Research Article Find the latest version: https://jci.me/105336/pdf Journal of Clinical Investigation Vol. 45, No. 2, 1966 Acute Poststreptococcal Glomerulonephritis: Immune Deposit Disease * ALFRED F. MICHAEL, JR.,t KEITH N. DRUMMOND,t ROBERT A. GOOD,§ AND ROBERT L. VERNIER || WITH THE TECHNICAL ASSISTANCE OF AGNES M. OPSTAD AND JOYCE E. LOUNBERG (From the Pediatric Research Laboratories of the Variety Club Heart Hospital and the Department of Pediatrics, University of Minnesota, Minneapolis, Minn.) The possible role of immunologic mechanisms in the kidney in acute glomerulonephritis have also acute poststreptococcal glomerulonephritis was revealed the presence of discrete electron dense suggested in 1908 by Schick (2), who compared masses adjacent to the epithelial surface of the the delay in appearance of serum sickness after glomerular basement membrane (11-18). injection of heterologous serum to the latent pe- The purpose of this paper is to describe immuno- riod between scarlet fever and onset of acute glo- fluorescent and electron microscopic observations merulonephritis. Evidence in support of this con- of the kidney in 16 children with acute poststrepto- cept is the depression of serum complement during coccal glomerulonephritis. This study demon- the early stages of the disease (3) and glomerular strates 1) the presence of discrete deposits of yG- localization of immunoglobulin. Immunofluores- and fl3c-globulins along the glomerular basement cent studies have revealed either no glomerular membrane and its epithelial surface that are similar deposition of a-globulin (4) or a diffuse involve- in size and location to the dense masses seen by ment of the capillary wall (5-9). -
Nephritis Fact Sheet
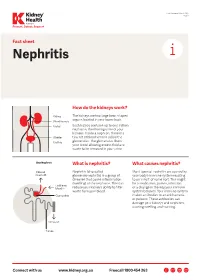
Last Reviewed March 2017 Page 1 Prevent, Detect, Support. Fact sheet Nephritis How do the kidneys work? The kidneys are two large bean-shaped organs located in your lower back. Each kidney contains up to one million nephrons, the filtering units of your kidneys. Inside a nephron, there is a tiny set of blood vessels called the glomerulus. The glomerulus filters your blood allowing excess fluid and waste to be removed in your urine. What is nephritis? What causes nephritis? Nephritis (also called Most types of nephritis are caused by glomerulonephritis) is a group of your body’s immune system reacting diseases that cause inflammation to an ‘insult’ of some sort. This might (swelling) of the nephrons. This can be a medication, poison, infection reduce your kidney’s ability to filter or a change in the way your immune waste from your blood. system behaves. Your immune system makes antibodies to attack bacteria or poisons. These antibodies can damage your kidneys and nephrons, causing swelling and scarring. Connect with us www.kidney.org.au Freecall 1800 454 363 Kidney Health Australia Nephritis Last Reviewed March 2017 Prevent, Detect, Support. Page 2 What are the different types of nephritis? There are many different types of Different types of nephritis include: Nephrotic syndrome: Damage to the nephritis. It can vary from a mild, nephrons causes them to leak large Focal nephritis: Less than a half of non-damaging condition to a serious amounts of protein into your urine your nephrons have scarring, and problem causing kidney failure. Some but little blood. Losing this protein blood and a small amount of protein types of nephritis appear mild at means your body does not have are found in your urine. -

Fibrillary Glomerulonephritis and Immunotactoid Glomerulopathy
PATHOPHYSIOLOGY of the RENAL BIOPSY www.jasn.org Fibrillary Glomerulonephritis and Immunotactoid Glomerulopathy Charles E. Alpers and Jolanta Kowalewska Department of Pathology, University of Washington, Seattle, Washington ABSTRACT extracellular accumulation of haphaz- Fibrillary glomerulonephritis is a now widely recognized diagnostic entity, occur- ardly arranged fibrils measuring ap- ring in approximately 1% of native kidney biopsies in several large biopsy series proximately 16 nm in thickness. Podo- obtained from Western countries. The distinctive features are infiltration of glo- cyte foot processes were diffusely merular structures by randomly arranged fibrils similar in appearance but larger effaced. There was no evidence of than amyloid fibrils and the lack of staining with histochemical dyes typically fibrillary deposits in the tubular base- reactive with amyloid. It is widely but not universally recognized to be distinct from ment membranes or interstitium. The immunotactoid glomerulopathy, an entity characterized by glomerular deposits of diagnosis of fibrillary glomerulone- immunoglobulin with substructural organization as microtubules and with clinical phritis was established on the basis of associations with lymphoplasmacytic disorders. The pathophysiologic basis for the ultrastructural findings in conjunc- organization of the glomerular deposits as fibrils or microtubules in these entities tion with the negative Congo Red stain remains obscure. and typical histologic and immunohis- J Am Soc Nephrol 19: 34–37, 2008. doi: -
Minimal Change Glomerulonephritis (GN)
Patient information – Minimal Change Glomerulonephritis Minimal Change Glomerulonephritis (GN) What is it? Your kidney biopsy has shown that your swelling and protein leak (nephrotic syndrome) is caused by a condition called ‘Minimal Change Glomerulonephritis’. This is an inflammation in the glomeruli (the network of blood capillaries) of the kidney, which shows very little change looking down the ordinary microscope. More specialised tests (such as electron microscopy) on the biopsy show characteristic changes to make this diagnosis. It is the commonest cause of nephrotic syndrome in children and causes about a quarter of those in adults. While the symptoms can be quite unpleasant, it does not cause long- term damage to the kidney function. While many types of nephrotic syndrome cannot be treated, Minimal Change GN will respond to steroid treatment. Initial treatment This stops the protein leak in 94 –100% of cases. The main treatment is high dose Prednisolone (steroids) tablets for up to 16 weeks (although usually less time). You will be seen every two weeks, and once the urine is clear of protein, the dose will be gradually reduced over the following six months. Prednisolone 1mg/kg of body weight (max 80mg) daily Lansoprazole 30mg daily Alendronate 70mg weekly Nystatin 1ml four times a day Septrin 480mg daily As steroids may have many side effects, you will also be given additional medication to protect you from some of the more serious ones. Some possible side effects of the steroids · Infection: Steroids make you more prone to ‘opportunist infection’ (so-called, because they only affect vulnerable people). You will be given antibiotics (Septrin and Fluconazole), to protect against thrush and pneumonia. -

Nephrotic Syndrome in Outpatient Practice
МИНИСТЕРСТВО ЗДРАВООХРАНЕНИЯ РЕСПУБЛИКИ БЕЛАРУСЬ БЕЛОРУССКИЙ ГОСУДАРСТВЕННЫЙ МЕДИЦИНСКИЙ УНИВЕРСИТЕТ КАФЕДРА ПОЛИКЛИНИЧЕСКОЙ ТЕРАПИИ Е. С. АЛЕКСЕЕВА, В. В. ДРОЩЕНКО, Е. В. ЯКОВЛЕВА НЕФРОТИЧЕСКИЙ СИНДРОМ В АМБУЛАТОРНОЙ ПРАКТИКЕ NEPHROTIC SYNDROME IN OUTPATIENT PRACTICE Учебно-методическое пособие Минск БГМУ 2019 1 УДК 616.61-008.6-039.57(075.8)-054.6 ББК 56.9я73 А46 Рекомендовано Научно-методическим советом университета в качестве учебно-методического пособия 21.06.2019 г., протокол № 10 Р е ц е н з е н т ы: канд. мед. наук, доц. 2-й каф. внутренних болезней Белорусского государственного медицинского университета О. А. Паторская; канд. мед. наук, доц. зав. каф. общей врачебной практики Белорусской медицинской академии последипломного образования И. В. Патеюк Алексеева, Е. С. А46 Нефротический синдром в амбулаторной практике = Nephrotic syndrome in outpatient practice : учебно-методическое пособие / Е. С. Алексеева, В. В. Дрощенко, Е. В. Яковлева. – Минск : БГМУ, 2019. – 26 с. ISBN 978-985-21-0408-1. Представлены сведения о критериях и патофизиологии нефротического синдрома, рассмотрены вопросы дифференциальной диагностики и лечения. Предназначено для студентов 5-го и 6-го курсов и медицинского факультета иностранных уча- щихся, обучающихся на английском языке. УДК 616.6-008.6-039.57(075.8)-054.6 ББК 56.9я73 ISBN 978-985-21-0408-1 © Алексеева Е. С., Дрощенко В. В., Яковлева Е. В., 2019 © УО «Белорусский государственный медицинский университет», 2019 2 ABBREVIATIONS ACE — Angiotensin-converting enzyme ApoB — Apolipoprotein B ANA — Antinuclear