Glomerulonephritis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

This Thesis Has Been Submitted in Fulfilment of the Requirements for a Postgraduate Degree (E.G
This thesis has been submitted in fulfilment of the requirements for a postgraduate degree (e.g. PhD, MPhil, DClinPsychol) at the University of Edinburgh. Please note the following terms and conditions of use: This work is protected by copyright and other intellectual property rights, which are retained by the thesis author, unless otherwise stated. A copy can be downloaded for personal non-commercial research or study, without prior permission or charge. This thesis cannot be reproduced or quoted extensively from without first obtaining permission in writing from the author. The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the author. When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given. Endothelin‐1 antagonism in glomerulonephritis Elizabeth Louise Owen BSc. (Hons), MSc. A thesis submitted towards the degree of PhD The University of Edinburgh 2016 Declaration I declare that the work presented in this thesis is my own and has not previously been published or presented towards another higher degree except where clearly acknowledged as such in the text. ……………………………………… …………. Elizabeth Louise Owen Date Page | 2 Acknowledgements I would like to express my gratitude to my supervisor David Kluth for his support, guidance and efforts during my PhD; Bean, thankyou for your patience and input. Thankyou also to Jeremy Hughes and Simon Brown for your advice and input for the various aspects of labwork, presentations and general how to’s. Jason King, thanks for all your help in the lab, you were always my ‘go‐to‐guy’ for all things technical….and for your many cool pairs of trainers. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Glomerulonephritis Management in General Practice
Renal disease • THEME Glomerulonephritis Management in general practice Nicole M Isbel MBBS, FRACP, is Consultant Nephrologist, Princess Alexandra lomerular disease remains an important cause Hospital, Brisbane, BACKGROUND Glomerulonephritis (GN) is an G and Senior Lecturer in important cause of both acute and chronic kidney of renal impairment (and is the commonest cause Medicine, University disease, however the diagnosis can be difficult of end stage kidney disease [ESKD] in Australia).1 of Queensland. nikky_ due to the variability of presenting features. Early diagnosis is essential as intervention can make [email protected] a significant impact on improving patient outcomes. OBJECTIVE This article aims to develop However, presentation can be variable – from indolent a structured approach to the investigation of patients with markers of kidney disease, and and asymptomatic to explosive with rapid loss of kidney promote the recognition of patients who need function. Pathology may be localised to the kidney or further assessment. Consideration is given to the part of a systemic illness. Therefore diagnosis involves importance of general measures required in the a systematic approach using a combination of clinical care of patients with GN. features, directed laboratory and radiological testing, DISCUSSION Glomerulonephritis is not an and in many (but not all) cases, a kidney biopsy to everyday presentation, however recognition establish the histological diagnosis. Management of and appropriate management is important to glomerulonephritis (GN) involves specific therapies prevent loss of kidney function. Disease specific directed at the underlying, often immunological cause treatment of GN may require specialist care, of the disease and more general strategies aimed at however much of the management involves delaying progression of kidney impairment. -

Management of Anemia in Non-Dialysis Chronic Kidney Disease: Current Recommendations, Real-World Practice, and Patient Perspectives
Kidney360 Publish Ahead of Print, published on July 1, 2020 as doi:10.34067/KID.0001442020 Management of Anemia in Non-Dialysis Chronic Kidney Disease: Current recommendations, real-world practice, and patient perspectives Murilo Guedes1,2, Bruce M. Robinson1,3, Gregorio Obrador4, Allison Tong5,6, Ronald L. Pisoni1, Roberto Pecoits-Filho1,2 1Arbor Research Collaborative for Health, Ann Arbor, MI, USA 2School of Medicine, Pontifícia Universidade Católica do Paraná, Curitiba, Brazil 3University of Michigan, Department of Internal Medicine, Ann Arbor, MI, USA 4Universidad Panamericana - Campus México, DF, MX, Mexico 5 Sydney School of Public Health, University of Sydney, Sydney, Australia 6 Centre for Kidney Research, The Children’s Hospital at Westmead, Sydney, Australia Corresponding Author Roberto Pecoits-Filho Arbor Research Collaborative for Health 3700 Earhart Road Ann Arbor, MI 48105 [email protected] 1 Copyright 2020 by American Society of Nephrology. Abstract In non-dialysis chronic kidney disease (ND-CKD), anemia is a multi-factorial and complex condition in which several dysfunctions dynamically contribute to a reduction in circulating hemoglobin (Hb) levels in red blood cells. Anemia is common in CKD, and represents an important and modifiable risk factor for poor clinical outcomes. Importantly, symptoms related to anemia, including reduced physical functioning and fatigue, have been identified as high priorities by patients with CKD. The current management of anemia in ND-CKD, i.e., parameters to initiate treatment, Hb and iron indexes targets, choice of therapies, and impact of treatment on clinical and patient-reported outcomes, remains controversial. In this review article, we explore the epidemiology of anemia in NDD-CKD, and revise current recommendations and controversies in its management. -

Supplemental Guide: Nephrology
Supplemental Guide for Nephrology Supplemental Guide: Nephrology March 2020 1 Supplemental Guide for Nephrology TABLE OF CONTENTS INTRODUCTION ............................................................................................................................. 3 PATIENT CARE .............................................................................................................................. 4 Acute Kidney Injury ...................................................................................................................... 4 Chronic Dialysis Therapy ............................................................................................................. 6 Chronic Kidney Disease ............................................................................................................... 8 Transplant .................................................................................................................................. 10 Fluid and Electrolytes ................................................................................................................. 12 Hypertension .............................................................................................................................. 13 Competence in Procedures ........................................................................................................ 15 MEDICAL KNOWLEDGE .............................................................................................................. 17 Physiology and Pathophysiology .............................................................................................. -

Diffuse Proliferative Glomerulonephritis and Acute Renal Failure Associated with Acute Staphylococcal Osteomyelitis
Diffuse Proliferative Glomerulonephritis and Acute Renal Failure Associated with Acute Staphylococcal Osteomyelitis MATTHEW D. GRIFFIN,* JOHANNES BJORNSSON,t and STEPHEN B. ERICKSON* *Department of Internal Medicine, Division of Nephrology, and tDepartment of Pathology, Mayo Clinic and Mayo Foundation, Rochester, Minnesota. Abstract. A 72-year-old man developed acute renal failure after peated surgical debridement. Spontaneous recovery of renal coronary bypass surgery that had been complicated by sternal function occurred after eradication of infection and final sur- osteomyelitis caused by the Staphylococcus aureus bacterium. gical wound repair. The relationship between acute bacterial Bacteremia and sepsis were not present. Renal biopsy demon- infections and glomerulonephritis and, in particular, the causal strated a florid, diffuse, proliferative glomerulonephritis with role of staphylococcal antigens in the pathogenesis of such glomerular immune complex deposition. Management in- lesions is discussed. (J Am Soc Nephrol 8: 1633-1639, 1997) cluded hemodialysis, prolonged antibiotic therapy, and re- Coagulase-positive staphylococcus (Staphylococcus aureus) is mg/dl]) and in the immediate postoperative period. Over the the most common causative organism in acute osteomyelitis following days, the patient’s serum creatinine concentration (1). Along with coagulase-negative staphylococcal species, it increased progressively, and hemodialysis was instituted on has also been implicated in the pathogenesis of immune com- day 23 after CABG. There was no past or family history of plex (IC)-mediated diffuse proliferative glomerulonephritis renal disease and no known drug allergies. Prior medical (DPGN) in a variety of infections. These include bacterial history had included degenerative disc disease, stable abdom- endocarditis, ventriculoatrial shunt infections, pneumonia, and inal aortic aneurysm, stable benign prostatic hyperplasia, and visceral abscesses with or without septicemia (2-6). -
2012 CKD Guideline
OFFICIAL JOURNAL OF THE INTERNATIONAL SOCIETY OF NEPHROLOGY KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease VOLUME 3 | ISSUE 1 | JANUARY 2013 http://www.kidney-international.org KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease KDIGO gratefully acknowledges the following consortium of sponsors that make our initiatives possible: Abbott, Amgen, Bayer Schering Pharma, Belo Foundation, Bristol-Myers Squibb, Chugai Pharmaceutical, Coca-Cola Company, Dole Food Company, Fresenius Medical Care, Genzyme, Hoffmann-LaRoche, JC Penney, Kyowa Hakko Kirin, NATCO—The Organization for Transplant Professionals, NKF-Board of Directors, Novartis, Pharmacosmos, PUMC Pharmaceutical, Robert and Jane Cizik Foundation, Shire, Takeda Pharmaceutical, Transwestern Commercial Services, Vifor Pharma, and Wyeth. Sponsorship Statement: KDIGO is supported by a consortium of sponsors and no funding is accepted for the development of specific guidelines. http://www.kidney-international.org contents & 2013 KDIGO VOL 3 | ISSUE 1 | JANUARY (1) 2013 KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease v Tables and Figures vii KDIGO Board Members viii Reference Keys x CKD Nomenclature xi Conversion Factors & HbA1c Conversion xii Abbreviations and Acronyms 1 Notice 2 Foreword 3 Work Group Membership 4 Abstract 5 Summary of Recommendation Statements 15 Introduction: The case for updating and context 19 Chapter 1: Definition, and classification -

Chapter 10: Radiation Nephropathy
Chapter 10: Radiation Nephropathy † Amaka Edeani, MBBS,* and Eric P. Cohen, MD *Kidney Diseases Branch, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland; and †Nephrology Division, Department of Medicine, University of Maryland School of Medicine, and Baltimore Veterans Affairs Medical Center, Baltimore, Maryland INTRODUCTION Classical radiation nephropathy occurred after external beam radiation for treatment of solid The occurrence of renal dysfunction as a consequence cancers such as seminomas (6); the incidence has of ionizing radiation has been known for more than declined with the advent of more effective chemo- 100 years (1,2). Initial reports termed this condition therapy. In recent years, radiation nephropathy has “radiation nephritis,” but that is a misnomer, because occurred due to TBI used as part of chemo-irradiation it is not an inflammatory condition. Renal radiation conditioning just before hematopoietic stem cell injury may be avoided by the exclusion of an ade- transplantation (HSCT) and also from targeted ra- quate volume of kidney exposure during radiation dionuclide therapy used for instance in the treatment therapy, but the kidneys’ central location can make of neuroendocrine malignancies. TBI may be myelo- this difficult to impossible when tumors of the abdo- ablative or nonmyeloablative, with myeloablative men or retroperitoneum are treated, or during total regimens using radiation doses of 10–12 Gy to de- body irradiation (TBI) (3). stroy or suppress the recipient’s bone marrow. These doses are given in a single fraction or in nine fractions over 3 days (4). In addition, TBI for bone marrow BACKGROUND/CLINICAL SIGNIFICANCE transplantation (BMT) is preceded or accompanied by cytotoxic chemotherapy, which potentiates the Radiation nephropathy is renal injury and loss of effects of ionizing radiation (7). -

Solid Tumour and Glomerulopathy
QJ Med 1996; 89:361-367 Solid tumour and glomerulopathy P. PAI, J.M. BONE, I. McDICKEN and CM. BELL From the Regional Renal Unit, Royal Liverpool University Hospital, Liverpool, UK Received 11 October 1995 and in revised form 31 January 1996 Downloaded from https://academic.oup.com/qjmed/article/89/5/361/1578010 by guest on 01 October 2021 Summary We retrospectively examined the prevalence of solid centic GN and one case of focal segmental GN. tumours in patients with glomerulonephritis (GN) Bronchogenic (6) and gastrointestinal carcinoma followed in our regional renal unit between 1977 (CA) (5) were the commonest tumours encountered. and 1994. We identified 17 cases of what was Other tumours included breast CA (1), renal cell thought to be solid-tumour-related glomerulo- CA (1), prostatic CA (1), an epithelial thymoma and nephritis. Tumours and GN were diagnosed together a leiomyosarcoma of the lung. All MGN and mesang- in six cases, and within a year of each other in ial proliferative GN cases developed nephrotic range another four. In addition, there were seven other proteinuria, whereas all patients with rapidly pro- cases with a weaker temporal relationship (median gressive crescentic GN presented with acute renal duration between GN and cancer diagnosis, two failure. Four cases had received immunosuppressive and a half years) but which nonetheless could be therapy prior to tumour diagnosis. We discuss the tumour-related. In total, there were seven membran- validity of each case as tumour-related glomerulo- ous GN, four mesangial proliferative GN, five cres- nephritis. Introduction Since the first clinicopathological study to present an University Hospital serves a population of 2 million association between cancer and nephrotic syndrome people in the Mersey region of the Northwest of (NS) was suggested by Lee et a\.? the subject of England. -
IDF Guide for Nurses Imimmmunnoogglolboubliun Ltinhe Trahpeyr Faopr Y Fopr Rpirmimaarryy I Mimmumnoudneoficdieenfciyc Ideisnecasy Es Diseases IDF GUIDE for NURSES
IDF Guide for Nurses ImImmmunnoogglolboubliun lTinhe Trahpeyr faopr y foPr rPirmimaarryy I mImmumnoudneoficdieenfciyc iDeisnecasy es Diseases IDF GUIDE FOR NURSES IMMUNOGLOBULIN THERAPY FOR PRIMARY IMMUNODEFICIENCY DISEASES THIRD EDITION COPYRIGHTS 2004, 2007, 2012 IMMUNE DEFICIENCY FOUNDATION Copyright 2012 by the Immune Deficiency Foundation, USA. PRINT: 12/2013 Readers may redistribute this publication to other individuals for non-commercial use, provided that the text, html codes, and this notice remain intact and unaltered in any way. The IDF Guide for Nurses may not be resold, reprinted or redistributed for compensation of any kind without prior written permission from the Immune Deficiency Foundation. If you have any questions about permission, please contact: Immune Deficiency Foundation, 40 West Chesapeake Avenue, Suite 308, Towson, MD 21204, USA, or by telephone: 800.296.4433. This publication has been made possible through a generous grant from IDF Guide for Nurses Immunoglobulin Therapy for Primary Immunodeficiency Diseases Third Edition Immune Deficiency Foundation 40 West Chesapeake Avenue, Suite 308 Towson, MD 21204 800.296.4433 www.primaryimmune.org Editor: M. Elizabeth M. Younger CRNP, PhD Johns Hopkins, Baltimore, Maryland Vice Chair, Immune Deficiency Foundation Nurse Advisory Committee Associate Editors: Rebecca H. Buckley, MD Duke University School of Medicine, Durham, NC Chair, Immune Deficiency Foundation Medical Advisory Committee Christine M. Belser Immune Deficiency Foundation, Towson, Maryland Kara Moran Immune Deficiency -
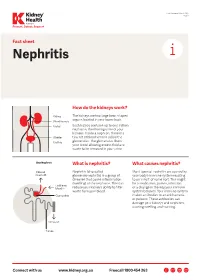
Nephritis Fact Sheet
Last Reviewed March 2017 Page 1 Prevent, Detect, Support. Fact sheet Nephritis How do the kidneys work? The kidneys are two large bean-shaped organs located in your lower back. Each kidney contains up to one million nephrons, the filtering units of your kidneys. Inside a nephron, there is a tiny set of blood vessels called the glomerulus. The glomerulus filters your blood allowing excess fluid and waste to be removed in your urine. What is nephritis? What causes nephritis? Nephritis (also called Most types of nephritis are caused by glomerulonephritis) is a group of your body’s immune system reacting diseases that cause inflammation to an ‘insult’ of some sort. This might (swelling) of the nephrons. This can be a medication, poison, infection reduce your kidney’s ability to filter or a change in the way your immune waste from your blood. system behaves. Your immune system makes antibodies to attack bacteria or poisons. These antibodies can damage your kidneys and nephrons, causing swelling and scarring. Connect with us www.kidney.org.au Freecall 1800 454 363 Kidney Health Australia Nephritis Last Reviewed March 2017 Prevent, Detect, Support. Page 2 What are the different types of nephritis? There are many different types of Different types of nephritis include: Nephrotic syndrome: Damage to the nephritis. It can vary from a mild, nephrons causes them to leak large Focal nephritis: Less than a half of non-damaging condition to a serious amounts of protein into your urine your nephrons have scarring, and problem causing kidney failure. Some but little blood. Losing this protein blood and a small amount of protein types of nephritis appear mild at means your body does not have are found in your urine. -

Fibrillary Glomerulonephritis and Immunotactoid Glomerulopathy
PATHOPHYSIOLOGY of the RENAL BIOPSY www.jasn.org Fibrillary Glomerulonephritis and Immunotactoid Glomerulopathy Charles E. Alpers and Jolanta Kowalewska Department of Pathology, University of Washington, Seattle, Washington ABSTRACT extracellular accumulation of haphaz- Fibrillary glomerulonephritis is a now widely recognized diagnostic entity, occur- ardly arranged fibrils measuring ap- ring in approximately 1% of native kidney biopsies in several large biopsy series proximately 16 nm in thickness. Podo- obtained from Western countries. The distinctive features are infiltration of glo- cyte foot processes were diffusely merular structures by randomly arranged fibrils similar in appearance but larger effaced. There was no evidence of than amyloid fibrils and the lack of staining with histochemical dyes typically fibrillary deposits in the tubular base- reactive with amyloid. It is widely but not universally recognized to be distinct from ment membranes or interstitium. The immunotactoid glomerulopathy, an entity characterized by glomerular deposits of diagnosis of fibrillary glomerulone- immunoglobulin with substructural organization as microtubules and with clinical phritis was established on the basis of associations with lymphoplasmacytic disorders. The pathophysiologic basis for the ultrastructural findings in conjunc- organization of the glomerular deposits as fibrils or microtubules in these entities tion with the negative Congo Red stain remains obscure. and typical histologic and immunohis- J Am Soc Nephrol 19: 34–37, 2008. doi: