Doctors, Torture, and the Canadian Armed Forces
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Day Two of Military Judge Questioning 9/11 Accused About Self-Representation
Public amnesty international USA Guantánamo: Day two of military judge questioning 9/11 accused about self-representation 11 July 2008 AI Index: AMR 51/077/2008 On 10 July 2008, military commission judge US Marine Colonel Ralph Kohlmann held further proceedings to question the men accused of orchestrating the attacks of 11 September 2001 about their decision to represent themselves at their forthcoming death penalty trial in the US Naval Base in Guantánamo Bay, Cuba. Amnesty International had an observer at the proceedings. The primary purpose of the hearings was to inquire of each of the accused individually about whether they had been intimidated before or during their arraignment on 5 June 2008 into making a choice to represent themselves, or whether this decision had been made knowingly and voluntarily. Judge Kohlmann had questioned two of the accused, ‘Ali ‘Abd al-‘Aziz ‘Ali (‘Ammar al Baluchi) and Mustafa al Hawsawi at individual sessions held on 9 July (see http://www.amnesty.org/en/library/info/AMR51/076/2008/en). He had scheduled sessions for the other three men, Khalid Sheikh Mohammed, Walid bin Attash and Ramzi bin al-Shibh on 10 July. In the event, Ramzi bin al-Shibh refused to come to his session. It seems unlikely that the military judge will question him again on the matter of legal representation until the issue of Ramzi bin al-Shibh’s mental competency is addressed at a hearing scheduled to take place next month (see http://www.amnesty.org/en/library/info/AMR51/074/2008/en). Both Khalid Sheikh Mohammed and Walid bin Attash denied that they had been intimidated or that any intimidation had taken place. -

The Oath a Film by Laura Poitras
The Oath A film by Laura Poitras POV www.pbs.org/pov DISCUSSION GUIDe The Oath POV Letter frOm the fiLmmakers New YorK , 2010 I was first interested in making a film about Guantanamo in 2003, when I was also beginning a film about the war in Iraq. I never imagined Guantanamo would still be open when I finished that film, but sadly it was — and still is today. originally, my idea for the Oath was to make a film about some - one released from Guantanamo and returning home. In May 2007, I traveled to Yemen looking to find that story and that’s when I met Abu Jandal, osama bin Laden’s former bodyguard, driving a taxicab in Sana’a, the capital of Yemen. I wasn’t look - ing to make a film about Al-Qaeda, but that changed when I met Abu Jandal. Themes of betrayal, guilt, loyalty, family and absence are not typically things that come to mind when we imagine a film about Al-Qaeda and Guantanamo. Despite the dangers of telling this story, it compelled me. Born in Saudi Arabia of Yemeni parents, Abu Jandal left home in 1993 to fight jihad in Bosnia. In 1996 he recruited Salim Ham - dan to join him for jihad in Tajikistan. while traveling through Laura Poitras, filmmaker of the Oath . Afghanistan, they were recruited by osama bin Laden. Abu Jan - Photo by Khalid Al Mahdi dal became bin Laden's personal bodyguard and “emir of Hos - pitality.” Salim Hamdan became bin Laden’s driver. Abu Jandal ends up driving a taxi and Hamdan ends up at Guantanamo. -

Print: Bush's Plan to Erode Our Liberties
Print: Bush's Plan to Erode Our Liberties http://www.thenation.com/doc/20070625/huq/print Bush's Plan to Erode Our Liberties by AZIZ HUQ June 8, 2007 Early this week, judge advocates halted two prosecutions in the Guantánamo military commissions established under the 2006 Military Commissions Act (MCA). This is not the first setback the Administration's second-tier court system has hit; the Supreme Court invalidated an earlier iteration of the commissions in 2006. And it won't be the last. But while this week's setback likely will be speedily surmounted, it casts an unexpected light on the MCA's real purposes, and what's at stake when the Bush Administration plays politics with national security. Understanding the significance of this week's ruling means delving into a bit of procedural arcana. The devil in the MCA is, almost literally, in the details--and unless we attend closely to the rococo details of the statute, we'll miss the ways in which the Administration intends to slowly erode our liberties. At the beginning of this week, the military commissions' two judges--Army Col. Peter Brownback and Navy Capt. Keith Allred--dismissed charges filed against Omar Khadr and Salim Hamdan. The rulings focused on a question of categorization--basically, the judges found that Khadr and Hamdan had been wrongly classified. But how did this happen? The MCA, which created the military commissions, states that only an alien who is an "unlawful enemy combatant" can be tried in a military commission. It also defines "unlawful enemy combatants" in tremendously sweeping terms to include anyone who has "materially supported hostilities." Many civil libertarians, including myself, expressed grave concerns about the scope of this provision. -
No Torture. No Exceptions
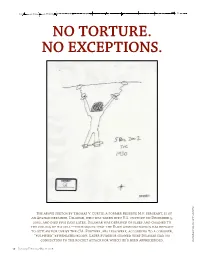
NO TORTURE. NO EXCEPTIONS. The above sketch by Thomas V. Curtis, a former Reserve M.P. sergeant, is of New York Times an Afghan detainee, Dilawar, who was taken into U.S. custody on December 5, 2002, and died five days later. Dilawar was deprived of sleep and chained to the ceiling of his cell—techniques that the Bush administration has refused to outlaw for use by the CIA. Further, his legs were, according to a coroner, “pulpified” by repeated blows. Later evidence showed that Dilawar had no connection to the rocket attack for which he’d been apprehended. A sketch by Thomas Curtis, V. a Reserve M.P./The 16 January/February/March 2008 Introduction n most issues of the Washington Monthly, we favor ar- long-term psychological effects also haunt patients—panic ticles that we hope will launch a debate. In this issue attacks, depression, and symptoms of post-traumatic-stress Iwe seek to end one. The unifying message of the ar- disorder. It has long been prosecuted as a crime of war. In our ticles that follow is, simply, Stop. In the wake of Septem- view, it still should be. ber 11, the United States became a nation that practiced Ideally, the election in November would put an end to torture. Astonishingly—despite the repudiation of tor- this debate, but we fear it won’t. John McCain, who for so ture by experts and the revelations of Guantanamo and long was one of the leading Republican opponents of the Abu Ghraib—we remain one. As we go to press, President White House’s policy on torture, voted in February against George W. -

The Value of Claiming Torture: an Analysis of Al-Qaeda's Tactical Lawfare Strategy and Efforts to Fight Back, 43 Case W
Case Western Reserve Journal of International Law Volume 43 | Issue 1 2010 The alueV of Claiming Torture: An Analysis of Al- Qaeda's Tactical Lawfare Strategy and Efforts to Fight Back Michael J. Lebowitz Follow this and additional works at: https://scholarlycommons.law.case.edu/jil Part of the International Law Commons Recommended Citation Michael J. Lebowitz, The Value of Claiming Torture: An Analysis of Al-Qaeda's Tactical Lawfare Strategy and Efforts to Fight Back, 43 Case W. Res. J. Int'l L. 357 (2010) Available at: https://scholarlycommons.law.case.edu/jil/vol43/iss1/22 This Article is brought to you for free and open access by the Student Journals at Case Western Reserve University School of Law Scholarly Commons. It has been accepted for inclusion in Case Western Reserve Journal of International Law by an authorized administrator of Case Western Reserve University School of Law Scholarly Commons. File: Lebowitz 2 Created on: 1/9/2011 9:48:00 PM Last Printed: 4/5/2011 8:09:00 PM THE VALUE OF CLAIMING TORTURE: AN ANALYSIS OF AL-QAEDA’S TACTICAL LAWFARE STRATEGY AND EFFORTS TO FIGHT BACK Michael J. Lebowitz* I. INTRODUCTION ..................................................................................... 357 II. CLAIMING TORTURE TO SHAPE THE BATTLEFIELD .............................. 361 A. Tactical Lawfare ........................................................................... 362 B. Faux Torture ................................................................................. 364 C. The Torture Benchmark ............................................................... -

True and False Confessions: the Efficacy of Torture and Brutal
Chapter 7 True and False Confessions The Efficacy of Torture and Brutal Interrogations Central to the debate on the use of “enhanced” interrogation techniques is the question of whether those techniques are effective in gaining intelligence. If the techniques are the only way to get actionable intelligence that prevents terrorist attacks, their use presents a moral dilemma for some. On the other hand, if brutality does not produce useful intelligence — that is, it is not better at getting information than other methods — the debate is moot. This chapter focuses on the effectiveness of the CIA’s enhanced interrogation technique program. There are far fewer people who defend brutal interrogations by the military. Most of the military’s mistreatment of captives was not authorized in detail at high levels, and some was entirely unauthorized. Many military captives were either foot soldiers or were entirely innocent, and had no valuable intelligence to reveal. Many of the perpetrators of abuse in the military were young interrogators with limited training and experience, or were not interrogators at all. The officials who authorized the CIA’s interrogation program have consistently maintained that it produced useful intelligence, led to the capture of terrorist suspects, disrupted terrorist attacks, and saved American lives. Vice President Dick Cheney, in a 2009 speech, stated that the enhanced interrogation of captives “prevented the violent death of thousands, if not hundreds of thousands, of innocent people.” President George W. Bush similarly stated in his memoirs that “[t]he CIA interrogation program saved lives,” and “helped break up plots to attack military and diplomatic facilities abroad, Heathrow Airport and Canary Wharf in London, and multiple targets in the United States.” John Brennan, President Obama’s recent nominee for CIA director, said, of the CIA’s program in a televised interview in 2007, “[t]here [has] been a lot of information that has come out from these interrogation procedures. -

Waterboarding: Political and Sacred Torture Stephen F
chapter 9 Waterboarding: Political and Sacred Torture Stephen F. Eisenman The Scene of Politics After the release of photographs of tortured prisoners at Abu Ghraib prison in Iraq in May 2003, a Gallup Poll indicated that 54 percent of Americans were “bothered a great deal” by the revelations. A year later the number had declined to 40 percent. In December 2005 an AP/IPSOS poll revealed that 61 percent of Americans agreed that torture was justifi ed, at least on some occasions.1 A May 2006 report by the UN High Commission for Human Rights about US torture at Guantánamo Bay was widely reported in newspapers, radio, and television, but produced no major outcries, public protests, or congressional investigations. Soon thereafter, President Bush— invoking the fi ctional “ticking bomb” scenario—successfully argued to Congress that the CIA should be allowed to use so-called “alternative interrogation procedures” and be given immunity from criminal prosecu- tion for prisoner abuse and war crimes. Despite the efforts of a few sena- tors, notably Patrick Leahy of Vermont, Sheldon Whitehouse of Rhode Island, and Joe Biden of Delaware, that immunity was granted. The US public and its representatives, it would seem, were not bothered by the fact 129 This content downloaded from 198.91.37.2 on Thu, 30 Jun 2016 01:27:50 UTC All use subject to http://about.jstor.org/terms CCarlson-Partarlson-Part IIII.inddII.indd 112929 77/2/2012/2/2012 44:54:33:54:33 PPMM 130 Stephen F. Eisenman that the US government permitted and even encouraged its agents to torture people held in their custody. -

THE DEATH of BAHA MOUSA the Death of Baha Mousa GERRY SIMPSON*
THE DEATH OF BAHA MOUSA The Death of Baha Mousa GERRY SIMPSON* [Between March 2003 and September 2004, 100 000 Iraqis are believed to have died as a consequence of the invasion of Iraq on 20 March 2003. Baha Mousa, an Iraqi hotel clerk was one of them. Mr Mousa died in Basra on or around 15 September 2003, after sustaining 93 separate injuries while in the custody of British soldiers belonging to the Duke of Lancaster’s Regiment. This think piece is about the law produced and invoked by his death.] CONTENTS I Introduction II Unlawful Conditioning III Common Law Crime IV War Crime V Human Rights Violation VI Baha Mousa How violent Schultz had sounded over the telephone. ‘I want justice,’ he had said. I wonder how many murders have been committed, and how many wars have been fought with that as a slogan … Justice is a thing that is better to give than to receive, but I am sick of giving it … I think it should be a prerogative of the gods.1 I INTRODUCTION On 14 September 2003, in Basra, southern Iraq, a hotel receptionist named Baha Mousa2 was detained by soldiers of the British Army’s Duke of Lancaster’s Regiment. Mousa and several other Iraqis were brought to a detention facility operated by the United Kingdom Armed Forces, and formerly run by Saddam Hussein’s cousin, Ali Hassann al-Majid, better known as ‘Chemical Ali’. Thirty-six hours later, Mr Mousa’s family were informed that Mr Mousa had died during detention. A subsequent post-mortem revealed that he had received 93 separate injuries, including a broken nose and fractured ribs — other prisoners suffered serious kidney damage.3 The reaction (on the part of the military, the legal profession, the media and the British establishment) to this incident tells us a little about the way * Gerry Simpson is a Professor of International Law at the London School of Economics. -
Human Rights Watch All Rights Reserved
HUMAN RIGHTS Delivered Into Enemy Hands US-Led Abuse and Rendition of Opponents to Gaddafi’s Libya WATCH Delivered Into Enemy Hands US-Led Abuse and Rendition of Opponents to Gaddafi’s Libya Copyright © 2012 Human Rights Watch All rights reserved. Printed in the United States of America ISBN: 1-56432-940-2 Cover design by Rafael Jimenez Human Rights Watch is dedicated to protecting the human rights of people around the world. We stand with victims and activists to prevent discrimination, to uphold political freedom, to protect people from inhumane conduct in wartime, and to bring offenders to justice. We investigate and expose human rights violations and hold abusers accountable. We challenge governments and those who hold power to end abusive practices and respect international human rights law. We enlist the public and the international community to support the cause of human rights for all. Human Rights Watch is an international organization with staff in more than 40 countries, and offices in Amsterdam, Beirut, Berlin, Brussels, Chicago, Geneva, Goma, Johannesburg, London, Los Angeles, Moscow, Nairobi, New York, Paris, San Francisco, Tokyo, Toronto, Tunis, Washington DC, and Zurich. For more information, please visit our website: http://www.hrw.org SEPTEMBER 2012 ISBN: 1-56432-940-2 Delivered Into Enemy Hands US-Led Abuse and Rendition of Opponents to Gaddafi’s Libya Summary ........................................................................................................................................... 1 Key Recommendations.................................................................................................................... -
Terrorism, Counter- Terrorism and Torture
TERRORISM, COUNTER- TERRORISM AND TORTURE INTERNATIONAL LAW IN THE FIGHT AGAINST TERRORISM JULY 2004 REALISED WITH FINANCIAL SUPPORT FROM THE EUROPEAN INITIATIVE FOR DEMOCRACY AND HUMAN RIGHTS The Redress Trust 87 Vauxhall Walk, 3rd Floor London, SE11 5HJ Tel: +44 (0)207 793 1777 Fax: +44(0)207 793 1719 Website: www.redress.org ACKNOWLEDGMENTS This report was written by Gabriela Echeverria, Legal Advisor (International), and edited by Carla Ferstman, Legal Director. REDRESS would like to express it sincere appreciation to Evelyn Sook May Yuen for her assistance in the research and preparation of this report and to Kevin Laue and Clementine Olivier for their many helpful comments on the draft of this report. CONTENTS INTRODUCTION ................................ ................................ ................................ .................. 1 PART 1. THE DISCOURSE................................ ................................ ................................ .. 3 1.1. DEFINITION/NON-DEFINITION OF TERRORISM..................................................................................3 1.1.1. Defining the ‘Crime’ of Terrorism in Domestic Law .......................................................................................................4 1.1.2. Vague and Overbroad Definitions of Terrorism.............................................................................................................5 1.1.3. Defining the Crime of Terrorism: Some Principles and Guidelines of International Law ..............................................7 -

Submission to the Baha Mousa Inquiry
British Irish RIGHTS WATCH SUBMISSION TO THE BAHA MOUSA INQUIRY SEPTEMBER 2010 1 1 Introduction 1.1 British Irish RIGHTS WATCH (BIRW) is an independent non- governmental organisation that has been monitoring the human rights dimension of the conflict, and the peace process, in Northern Ireland since 1990. Our vision is of a Northern Ireland in which respect for human rights is integral to all its institutions and experienced by all who live there. Our mission is to secure respect for human rights in Northern Ireland and to disseminate the human rights lessons learned from the Northern Ireland conflict in order to promote peace, reconciliation and the prevention of conflict. BIRW’s services are available, free of charge, to anyone whose human rights have been violated because of the conflict, regardless of religious, political or community affiliations. BIRW take no position on the eventual constitutional outcome of the conflict. Our charitable ojects include the abolition of torture, extrajudicial execution, arbitrary arrest, detention and exile. 1.2 BIRW are responding to the invitation made by Sir William Gage to make submissions to the Baha Mousa Inquiry, which was instigated, as the Secretary of State for Defence has acknowledged1 not just because a man died in the custody of British soldiers but because an investigation by the Royal Military Police and a subsequent Court Martial highlighted further important questions that needed to be answered. 1.3 We are making submissions to the Baha Mousa Inquiry on the basis of our extensive experience of monitoring the human rights situation in Northern Ireland. We believe that we are in a position to offer valuable insights regarding the circumstances leading to the death of Baha Mousa and the aftermath of this tragedy given our extensive understanding of the historically analogous lessons from the conflict in Northern Ireland. -
Guantanamo Bay (Also GTMO Or Gitmo) Is a US Naval Base in Cuba Covering 45 Square Miles
Guantanamo Bay (also GTMO or Gitmo) is a US Naval base in Cuba covering 45 square miles. It contains several prison camps, the first of which was established by the Bush Administration in January 2002 to house enemy combatants captured in Afghanistan. The US Government committed to closing the prison by January 2010 however as of March 2011 there are 172 prisoners still housed with no immediate date for closure. This PDF is a text version of the interactive feature, How To Get Out Of Guantanamo. abc.net.au/innovation/gitmo PAGE 1/11 © ABC 2011 HOW TO GET OUT OF GUANTANAMO abc.net.au/innovation/gitmo 779 DETAINED SINCE 2002 The first 20 prisoners arrived at Guantanamo on Jan 11 2002 from Afghanistan. They were detained under a Military Order issued by President Bush after the 9/11 attacks allowing individuals to be held without charge indefinitely. On Feb 7 2002, Bush signed a memorandum excluding them from prisoner of war status (POW) and Article 3 of the Geneva Convention; Article 3 prohibits unfair trials, torture, cruelty and outrages on human dignity. On March 14, 2008, the last known prisoner arrived at Guantanamo Bay. At its peak capacity Guantanamo has housed about 660 pris- oners (November 2003). 12 of these prisoners have been children under the age of 16. Some inmates were transferred to the prison after being held for months or years in detention at so-called CIA 'black sites'. This included 14 men in 2006 described as 'high value detainees'. REFERENCES: Amnesty International, Guantanamo Timeline (2008) http://www.amnesty.org/en/library/asset/AMR51/148/2008/en/d620ceca-cde2-11dd-b0c5-1f8db3691f48/amr511482008en.html