District Health Plan : 2015-2016 : Umzinyathi
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

250 CHAPTER 8 MARTIAL LAW, the LINGERING WAR, and ITS SOCIO-POLITICAL IMPACT on NATAL AFRIKANERS Martial Law Was Declared In
University of Pretoria etd – Wassermann, J M (2005) 250 CHAPTER 8 MARTIAL LAW, THE LINGERING WAR, AND ITS SOCIO-POLITICAL IMPACT ON NATAL AFRIKANERS Martial Law was declared in all of Natal on 23 October 18991 to act as Athe public law of self- defence (and) the right to use military means to preserve the peace against public enemies within.@2 The military commander of each area was responsible for the administration thereof. Martial Law gave the military authorities the power to use extreme measures to maintain safety and security. To achieve this movements were restricted, passes were issued,3 people were arrested and removed from their farms, and property was commandeered.4 Like most instances of Martial Law, the populace found the conditions deplorable and oppressive, and as the war dragged on beyond June1900, the relentless pressure on Natal Afrikaners made it difficult for them to manoeuver under the jingoistic wartime conditions. In Natal Martial Law was initially upheld by the Indemnity Bill published on 5 June 1900 to protect Athe Governor of the Colony, and the Officer Commanding her Majesty=s Forces in Natal, and all persons acting under their authority and in good faith in regard to acts during the existence of Martial Law.@5 This bill was subsequently updated by other Indemnity Bills as circumstances changed.6 The community of Natal Afrikaners received the bill with mixed emotions. On the one hand people such as Ds HF Schoon argued that it would sanction all kinds of abuses by the authorities,7 while the Afrikaner politician, CJ Labuschagne, who himself was innocently imprisoned under Martial Law, voted in favour of the Indemnity Bill.8 In the light of the above the emphasis in this chapter will be twofold. -

Eliminating the Scourge of Illegal Termination of Pregnancy – a Call to Action
SPONSORED SUPPLEMENT CAMPAIGN ON ILLEGAL TERMINATION OF PREGNANCY #StopIllegalAbortionDeaths Eliminating the scourge of illegal termination of pregnancy – a call to action Information containing warnings on the danger of illegal termination of pregnancy providers and where safe termination of pregnancy services are offered have been distributed during awareness marches held throughout the province. Pictured at one of these events, KZN Health MEC Dr Sibongiseni Dhlomo helps remove posters advertising illegal termination of pregnancy services. N November 17, the KwaZulu- “The product, illegal termination of pregnancy, is skillfully marketed and sold to the affordable,” continued Dhlomo.“And Natal Health MEC, Dr women must have an emotionally safe OSibongiseni Dhlomo launched woman at the crisis time in her life. She buys the product, finds it defective and wants space in which to make their decision.” the province’s Campaign on illegal to return it for a refund. But, it’s too late.”– KZN Health MEC, Dr Sibongiseni Dhlomo “Unsafe termination of pregnancy Termination of Pregnancy.The have eaten into our society, gradually initiative is an urgent call for action Africa still remains a place where ranks and shopping centres, makes of pregnancy are undergone by young destroying the lives of young women, against illegal termination of women choose backstreet providers many women believe they are people between the ages of 13 and 19 as people have closed their eyes to pregnancy and aims to highlight the against the widespread available accessing a legitimate service.” years, and that these take place the issue, hoping it would disappear.” dangers of illegal termination of government-sanctioned centres. -

Kwa-Zulu Natal No Fee Schools 2017
KWA-ZULU NATAL NO FEE SCHOOLS 2017 NATIONAL EMIS NAME OF SCHOOL SCHOOL PHASE ADDRESS OF SCHOOL EDUCATION DISTRICT QUINTILE LEARNER NUMBER 2017 NUMBERS 2017 500101195 A.M. MOOLLA SECONDARY SCHOOL S KWASHANGASE TRIBAL AUTHORITY ILEMBE 1 169 500100270 ABAQULUSI HIGH SCHOOL S Bhadeni Area ZULULAND 1 583 500100307 ABATHWA PRIMARY SCHOOL P Ogazini Area UMZINYATHI 1 253 500101010 ALPHA PRIMARY SCHOOL P KROMMELENBOOG FARM ZULULAND 1 14 500101121 ALVA PRIMARY SCHOOL C FREIBERG FARM UMZINYATHI 1 207 500101528 AMAHOBE PRIMARY SCHOOL P AMAJUBA FOREST AMAJUBA 1 134 500493654 AMAKHUZE SECONDARY SCHOOL S Makhongwana Location HARRY GWALA 1 399 500101713 AMAKHWATHA PRIMARY SCHOOL C 55I STRETCH CRESCENT ROAD ZULULAND 1 886 500101861 AMANDLAKAPHELI PRIMARY SCHOOL P Kwalembe Tribal Authority UGU 1 128 500342509 AMANDLAKHE PRIMARY SCHOOL P Care of kwa-Qumbu UMGUNGUNDLOVU 1 150 500308062 AMANDLALATHI PRIMARY SCHOOL P VULAMEHLO MUNICIPALITY UGU 1 261 500102416 AMAPHUPHESIZWE HIGH SCHOOL S Umphumulo Mission ILEMBE 1 553 500102453 AMAPHUTHU HIGH SCHOOL S Thulani area KING CETSHWAYO 1 243 500102527 AMAQHAWE PRIMARY SCHOOL P MAKWAKWA AREA UMKHANYAKUDE 1 819 500102786 AMATIMOFU PRIMARY SCHOOL P EMPAPHALA RESERVE KING CETSHWAYO 1 110 500102897 AMAYESE PRIMARY SCHOOL P Ngono Tribal Authority, Mfongosi Area, Amayese road KING CETSHWAYO 1 87 500308876 AMAZONDI SECONDARY SCHOOL S Mpotholo Area Kwazondi tribal authority KING CETSHWAYO 1 384 500423613 ANTIOCH JUNIOR SECONDARY SCHOOL P ANTIOCH LOCATION HARRY GWALA 1 265 500103489 ARDEN PRIMARY SCHOOL P D 158 UMGUNGUNDLOVU -

Draft 2019/20 IDP Prepared by Umzinyathi District Municipality 1 29 March 2019
Table of Contents SECTION A: EXECUTIVE SUMMARY ................................................................................................................ 11 1 WHO ARE WE ............................................................................................................................................... 11 1.1 SPATIAL LOCATION WITHIN KZN PROVINCE .......................................................................................................... 11 1.1.1 Demographics Trends and Characteristics .......................................................................................... 15 1.2 INFRASTRUCTGURE ANALYSIS ............................................................................................................................. 16 1.2.1 Water .................................................................................................................................................. 16 1.2.2 Sanitation ............................................................................................................................................ 17 1.3 LONG TERM VISION ......................................................................................................................................... 18 1.3.1 IDP Development Process, Phases And Key Timeframes .................................................................... 18 1.4 KEY DEVELOPMENTAL CHALLENGES FACING THE MUNICIPALITY AND PROPOSED INTERVENTIONS ................................... 25 1.5 HIGH LEVEL MUNICIPAL PROGRAMMES AND MONITORING -

Umzinyathi District Profile
2 PROFILE: UMZINYATHI DISTRICT PROFILE PROFILE: UMZINYATHI DISTRICT PROFILE 3 CONTENT 1. Executive Summary ....................................................................................................... 6 2. Brief overview ................................................................................................................ 7 2.1. Location .................................................................................................................. 7 3. Social Development ....................................................................................................... 9 3.1. Key Demographics .................................................................................................. 9 3.1.1. Population and Household Profile ........................................................................ 9 3.1.2. Age and Gender Profile ...................................................................................... 10 3.2. Health .................................................................................................................... 10 3.3. Covid-19 ................................................................................................................ 12 3.4. Poverty and Inequality ........................................................................................... 12 3.6. Education .............................................................................................................. 13 4. Economic Drivers ........................................................................................................ -
Internal Migration and Poverty in Kwazulu-Natal: Findings from Censuses, Labour Force Surveys and Panel Data
Southern Africa Labour and Development Research Unit Internal Migration and Poverty in KwaZulu-Natal: Findings from Censuses, Labour Force Surveys and Panel Data by Michael Rogan, Likani Lebani, and Nompumelelo Nzimande WORKING PAPER SERIES Number 30 About the Author(s) and Acknowledgments Funding for this research was generously provided by the Andrew W. Mellon Foundation- Poverty and Inequality Node and the Southern Africa Labour and Development Research Unit (SALDRU) at the University of Cape Town Recommended citation Rogan N., Lebani L., and Nzimande M. (2009) Internal Migration and Poverty in KwaZulu-Natal: Findings from Censuses, Labour Force Surveys and Panel Data. A Southern Africa Labour and Devel- opment Research Unit Working Paper Number 30. Cape Town: SALDRU, University of Cape Town ISBN: 978-0-9814304-1-6 © Southern Africa Labour and Development Research Unit, UCT, 2009 Working Papers can be downloaded in Adobe Acrobat format from www.saldru.uct.ac.za. Printed copies of Working Papers are available for R15.00 each plus vat and postage charges. Orders may be directed to: The Administrative Officer, SALDRU, University of Cape Town, Private Bag, Rondebosch, 7701, Tel: (021) 650 5696, Fax: (021) 650 5697, Email: [email protected] Internal Migration and Poverty in KwaZulu-Natal: Findings from Censuses, Labour Force Surveys and Panel Data Michael Rogan, Likani Lebani, and Nompumelelo Nzimande1 January 10, 2008 Provincial Poverty and Migration Report submitted to the Southern Africa Labour and Development Research Unit (SALDRU) at the University of Cape 2 Town. 1 Researcher- School of Development Studies; Researcher- School of Development Studies; Lecturer- School of Development Studies. -
1. Introduction
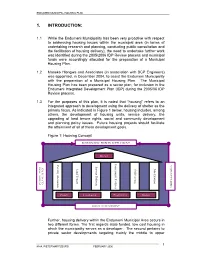
ENDUMENI MUNICIPAL HOUSING PLAN 1. INTRODUCTION: 1.1 While the Endumeni Municipality has been very proactive with respect to addressing housing issues within the municipal area (in terms of undertaking research and planning, conducting public consultation and the facilitation of housing delivery), the need to undertake further work was identified during the 2005/2006 IDP Review process and municipal funds were accordingly allocated for the preparation of a Municipal Housing Plan. 1.2 Maseko Hlongwa and Associates (in association with BCP Engineers) was appointed, in December 2004, to assist the Endumeni Municipality with the preparation of a Municipal Housing Plan. The Municipal Housing Plan has been prepared as a sector plan, for inclusion in the Endumeni Integrated Development Plan (IDP) during the 2005/06 IDP Review process. 1.3 For the purposes of this plan, it is noted that “housing” refers to an integrated approach to development using the delivery of shelter as the primary focus. As indicated in Figure 1 below, housing includes, among others, the development of housing units, service delivery, the upgrading of land tenure rights, social and community development and planning policy issues. Future housing projects should facilitate the attainment of all of these development goals. Figure 1: Housing Concept SUSTAINABLE HUMAN SETTLEMENT Shelter Community Facilities Community Facilities Poverty Alleviation Poverty Alleviation NATION BUILDING NATION Service Delivery DEVELOPMENT INTEGRATED INTEGRATED Land Tenure J Self Esteem ob Creation Policy Legislation Programmes Budget SOCIAL DEVELOPMENT Further, housing delivery within the Endumeni Municipal Area occurs in two different forms. The first regards state funded, low cost housing in which the municipality serves as a developer. -

Msinga Municipality Spatial Development Framework 2020
MSINGA MUNICIPALITY SPATIAL DEVELOPMENT FRAMEWORK DRAFT STATUS QUO REPORT JUNE 2020 MSINGA MUNICIPALITY SPATIAL DEVELOPMENT FRAMEWORK 2020 Contents CHAPTER 1: BACKGROUND AND PURPOSE 1 1.1 INTRODUCTION 1 1.2 PURPOSE OF THE REPORT 1 1.3 WHAT IS A SPATIAL DEVELOPMENT FRAMEWORK 2 1.4 LEGAL AND POLICY IMPERATIVES 3 1.5 RELATIONSHIP WITH OTHER PLANS 4 1.6 DEFINING THE STUDY AREA 5 1.7 STRUCTURE OF THIS DOCUMENT 9 1.8 STUDY OBJECTIVES/ISSUES TO BE ADDRESSED 9 1.9 MUNICIPAL SPATIAL STRUCTURE AND DEVELOPMENT INFORMANTS 11 CHAPTER 2: STATUS QUO OF MSINGA MUNICIPALITY 12 2.1 LEGISLATIVE ENVIRONMENT 12 2.1.1 SOUTH AFRICAN CONSTITUTION AND PRINCIPLES OF SUSTAINABLE DEVELOPMENT (NO. 108 OF 1196) ..................................................................................................................................... 12 2.1.2 MUNICIPAL SYSTEMS ACT (NO. 32 OF 2000) ........................................................................... 12 2.1.3 NATIONAL ENVIRONMENTAL MANAGEMENT ACT (NO. 107 OF 1998) ................................... 14 2.1.4 SOCIAL HOUSING ACT (NO.16 OF 2008) .................................................................................. 14 2.1.5 THE KWAZULU-NATAL HERITAGE ACT (NO 4 OF 2008) ........................................................... 16 2.1.6 SPLUMA (NO 16 OF 2013) ........................................................................................................ 17 2.2 POLICY ENVIRONMENT 21 2.2.1 PROVINCIAL GROWTH AND DEVELOPMENT STRATEGY ......................................................... -
![[Endumeni Integrated Development Plan (Idp)]](https://docslib.b-cdn.net/cover/7710/endumeni-integrated-development-plan-idp-2257710.webp)
[Endumeni Integrated Development Plan (Idp)]
Page | i EENNDDUUMMEENNII IINNTTEEGGRRAATTEEDD DDEEVVEELLOOPPMMEENNTT [ [ F PPLLAANN F I ((IIDDPP)) I N N A A L L ] ] [2014/ 2015] ENDUMENI MUNICIPALITY FINAL IDP 2014/15 Page | ii ENDUMENI MUNICIPALITY IDP 2014/2015 FOREWORD BY HIS WORSHIP THE MAYOR, CLLR T. M. MAHAYE It is my privilege to present the Final IDP for the 2014/2015 financial year. The IDP was compiled under challenging circumstances. Council was challenged with a very difficult period, where regular council meetings did not take place, vacancies in senior positions existed for the whole of the current financial year and important decisions were delayed. Against this background and a very challenging economic period, we still succeeded to deliver services at an acceptable level. We have also managed to obtain an unqualified audit report for the previous year. The draft IDP was tabled and available for comments and further input through a process of community consultation, before approval. While taking into account of the constrained fiscal environment, we continue to support Government’s commitment to broadening service delivery and expanding investment in infrastructure. There are certain challenges, but this IDP will take us forward and we will be comitted to address and resolve the major challenges such as meter-tampering and the community at large will have to co-operate in dealing with this challenge. Should we fail to stop these unlawful practices, it will result in cash flow problems with a detrimental effect on service delivery. Council will have to apply all efforts to resolve these challenges before much progress could be made in addressing other challenges like improved service delivery and meeting the needs of the community. -

KZN Administrative Boundaries Western Cape 29°0'0"E 30°0'0"E 31°0'0"E 32°0'0"E 33°0'0"E
cogta Department: Locality Map Cooperative Governance & Traditional Affairs Limpopo Mpumalanga North West Gauteng PROVINCE OF KWAZULU-NATAL Free State KwaZulu-Natal Northern Cape Eastern Cape KZN Administrative Boundaries Western Cape 29°0'0"E 30°0'0"E 31°0'0"E 32°0'0"E 33°0'0"E Mozambique Mboyi Swaziland 5! Kuhlehleni 5! Kosi Bay 5! Manyiseni MATENJWA 5! Ndumo MPUMALANGA T. C 5! KwaNgwanase Jozini Local 5! 5! Manguzi 27°0'0"S Nkunowini Boteler Point 27°0'0"S 5! Municipality 5! (KZN272) Sihangwane 5! Phelandaba 5! MNGOMEZULU T. C TEMBE Kwazamazam T. C 5! Dog Point Machobeni 5! 5! Ingwavuma 5! Mboza Umhlabuyalingana Local ! 5 Municipality (KZN271) NYAWO T. C Island Rock 5! Mpontshani 5! Hully Point Vusumuzi 5! 5! Braunschweig 5! Nhlazana Ngcaka Golela Ophondweni ! 5! Khiphunyawo Rosendale Zitende 5! 5! 5 5! 5! 5! KwaNduna Oranjedal 5! Tholulwazi 5! Mseleni MASHBANE Sibayi 5! NTSHANGASE Ncotshane 5! 5! T. C 5! T. C NTSHANGASE T. C SIQAKATA T. C Frischgewaagd 5! Athlone MASIDLA 5! DHLAMINI MSIBI Dumbe T. C SIMELANE 5! Pongola Charlestown 5! T. C T. C Kingholm 5! T. C Mvutshini 5! Othombothini 5! KwaDlangobe 5! 5! Gobey's Point Paulpietersburg Jozini 5! Simlangetsha Fundukzama 5! 5! ! 5! Tshongwe 5 ! MABASO Groenvlei Hartland 5 T. C Lang's Nek 5! eDumbe Local 5! NSINDE 5! ZIKHALI Municipality Opuzane Candover T. C 5! Majuba 5! 5! Mbazwana T. C Waterloo 5! (KZN261) MTETWA 5! T. C Itala Reserve Majozini 5! KwaNdongeni 5! 5! Rodekop Pivana 5! ! Emadlangeni Local ! 5! Magudu 5 5 Natal Spa Nkonkoni Jesser Point Boeshoek 5! 5!5! Municipality 5! Ubombo Sodwana Bay Louwsburg UPhongolo Local ! (KZN253) 5! 5 Municipality Umkhanyakude (KZN262) Mkhuze Khombe Swaartkop 5! 5! 5! District Madwaleni 5! Newcastle 5! Utrecht Coronation Local Municipality 5! 5! Municipality NGWENYA Liefeldt's (KZN252) Entendeka T. -

Umzinyathi District Municipality: Biodiversity Sector Plan
uMzinyathi District Municipality: Biodiversity Sector Plan EZEMVELO KZN WILDLIF E Version: Version 1.0 BIODIVERSITY SECTOR PLA N Date: February 2014 i Biodiversity Sector Plan - uMzinyathi District Municipality 2014 Document Details Authored by: Ntando Ninela & Felicity Elliott Ezemvelo KZN Wildlife P.O. Box 13053 Cascades, 3202 Document is available from: Ezemvelo KZN Wildlife website, www.kznwildlife.com This guideline should be cited as: Ezemvelo KZN Wildlife (2014), uMzinyathi Biodiversity Sector Plan,V1.0, Unpublished Report of Ezemvelo KZN Wildlife, Biodiversity Conservation Planning Division, Ezemvelo KZN Wildlife, P. O. Box 13053, Cascades, Pietermaritzburg. RECOMMENDED Title Name Signature Date Chairperson: EKZNW , SOCC Chairperson: EKZNW , Operations Committee Chief Executive Officer EKZNW APPROVED Chairperson: KZN Nature Conservation Board F E B R UA R Y 2 0 1 4 - Ve rs i o n 1 .0 II Biodiversity Sector Plan - uMzinyathi District Municipality 2014 Acknowledgements Specialists involved in the development, consulting or review during production of the uMzinyathi District Biodiversity Sector Plan include the following key persons. Name Position Affiliation Dr Boyd Escott Manager: Biodiversity Spatial Planning & Information & Acting GIS Analysis Terrestrial Debbie Jewitt Biodiverty Research & Assessment Ezemvelo KZN Wildlife (Ecosystem ecologist) Felicity Elliott Biodiversity Spatial Planning& Information (Bioregional Planning) Heidi Snyman Biodiversity Spatial Planning& Information (Cartography) Bimal Naidoo Biodiversity Spatial -

Section B, Chapter 13
SectionSection B: B:Profile National KwaZulu-Natal and District Province Profiles 13 KwaZulu-Natal Province Ugu District Municipality (DC21) The Ugu District Municipalitya is a Category C municipality situated in the far south of KwaZulu-Natal. The district is made up of four local municipalities: uMdoni, uMzumbe, Ray Nkonyeni and uMuziwabantu. Cities/Towns: Harding, Hibberdene, Margate, Pennington, Port Edward, Port Shepstone, Scottburgh/Umzinto North, Southbroom Area: 4 791km² Population (2019)b: 796 446 DistrictDistrict % ppercentageopulation by ag epopulation-gender group cbyom page-genderared to South Af rgroupica compared to South Africa KZ, Ugu DM (DC21) 2000/01 2010/11 2020/21 South Africa % of total population [Male | Female] - lines South Africa % of total population [Male | Female] - lines South Africa % of total population [Male | Female] - lines AgeGrp 8% 6% 4% 2% 0% 2% 4% 6% 8% 8% 6% 4% 2% 0% 2% 4% 6% 8% 8% 6% 4% 2% 0% 2% 4% 6% 8% 65+ 2.1% 4.2% 1.8% 4.0% 3.5% 60-64 years 1.6% 1.7% 1.6% 55-59 years 1.8% 1.9% 1.9% 50-54 years 1.5% 2.3% 2.2% 1.9% 45-49 years 1.6% 2.3% 1.3% 2.5% 1.5% 2.2% 40-44 years 1.8% 2.8% 1.5% 2.5% 2.1% 2.6% 35-39 years 2.2% 3.4% 2.1% 2.8% 3.6% 3.7% 30-34 years 2.3% 3.2% 2.7% 3.1% 4.8% 4.5% 25-29 years 3.0% 3.8% 4.2% 4.3% 5.0% 4.6% 20-24 years 3.4% 3.9% 5.6% 5.5% 4.3% 4.1% 15-19 years 6.0% 6.2% 6.1% 6.0% 4.8% 4.7% 10-14 years 6.9% 7.0% 5.3% 5.3% 5.9% 5.8% 05-09 years 6.8% 6.8% 5.5% 5.5% 6.1% 5.8% 00-04 years 5.4% 5.4% 6.8% 6.7% 5.9% 5.7% 8% 6% 4% 2% 0% 2% 4% 6% 8% 8% 6% 4% 2% 0% 2% 4% 6% 8% 8% 6% 4% 2% 0% 2% 4% 6% 8% District % of total population [Male | Female] - bars District % of total population [Male | Female] - bars District % of total population [Male | Female] - bars Sex Gender (ZA) female female (ZA) male male (ZA) Burden of disease profile For the percentage of deaths by broad cause, deaths are classified into four groups, namely: (i) injuries; (ii) non- communicable diseases; (iii) HIV and TB; and (iv) communicable diseases together with maternal, perinatal and nutritional conditions.