Dracunculiasis in the United Republic Ov Cameroon Ii
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Page 1 C H a D N I G E R N I G E R I a G a B O N CENTRAL AFRICAN
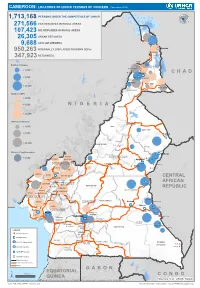
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (November 2019) 1,713,168 PERSONS UNDER THE COMPETENCENIGER OF UNHCR 271,566 CAR REFUGEES IN RURAL AREAS 107,423 NIG REFUGEES IN RURAL AREAS 26,305 URBAN REFUGEES 9,688 ASYLUM SEEKERS 950,263 INTERNALLY DISPLACED PERSONS (IDPs) Kousseri LOGONE 347,923 RETURNEES ET CHARI Waza Limani Magdeme Number of refugees EXTRÊME-NORD MAYO SAVA < 3,000 Mora Mokolo Maroua CHAD > 5,000 Minawao DIAMARÉ MAYO TSANAGA MAYO KANI > 20,000 MAYO DANAY MAYO LOUTI Number of IDPs < 2,000 > 5,000 NIGERIA BÉNOUÉ > 20,000 Number of returnees NORD < 2,000 FARO MAYO REY > 5,000 Touboro > 20,000 FARO ET DÉO Beke chantier Ndip Beka VINA Number of asylum seekers Djohong DONGA < 5,000 ADAMAOUA Borgop MENCHUM MANTUNG Meiganga Ngam NORD-OUEST MAYO BANYO DJEREM Alhamdou MBÉRÉ BOYO Gbatoua BUI Kounde MEZAM MANYU MOMO NGO KETUNJIA CENTRAL Bamenda NOUN BAMBOUTOS AFRICAN LEBIALEM OUEST Gado Badzere MIFI MBAM ET KIM MENOUA KOUNG KHI REPUBLIC LOM ET DJEREM KOUPÉ HAUTS PLATEAUX NDIAN MANENGOUBA HAUT NKAM SUD-OUEST NDÉ Timangolo MOUNGO MBAM ET HAUTE SANAGA MEME Bertoua Mbombe Pana INOUBOU CENTRE Batouri NKAM Sandji Mbile Buéa LITTORAL KADEY Douala LEKIÉ MEFOU ET Lolo FAKO AFAMBA YAOUNDE Mbombate Yola SANAGA WOURI NYONG ET MARITIME MFOUMOU MFOUNDI NYONG EST Ngarissingo ET KÉLLÉ MEFOU ET HAUT NYONG AKONO Mboy LEGEND Refugee location NYONG ET SO’O Refugee Camp OCÉAN MVILA UNHCR Representation DJA ET LOBO BOUMBA Bela SUD ET NGOKO Libongo UNHCR Sub-Office VALLÉE DU NTEM UNHCR Field Office UNHCR Field Unit Region boundary Departement boundary Roads GABON EQUATORIAL 100 Km CONGO ± GUINEA The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Sources: Esri, USGS, NOAA Source: IOM, OCHA, UNHCR – Novembre 2019 Pour plus d’information, veuillez contacter Jean Luc KRAMO ([email protected]). -

Characterisation of Fungi of Stored Common Bean Cultivars Grown in Menoua Division, Cameroon
bioRxiv preprint doi: https://doi.org/10.1101/2020.10.31.363184; this version posted November 1, 2020. The copyright holder has placed this preprint (which was not certified by peer review) in the Public Domain. It is no longer restricted by copyright. Anyone can legally share, reuse, remix, or adapt this material for any purpose without crediting the original authors. CHARACTERISATION OF FUNGI OF STORED COMMON BEAN CULTIVARS GROWN IN MENOUA DIVISION, CAMEROON TEH EXODUS AKWA*1, JOHN M MAINGI1, JONAH K. BIRGEN2 *Corresponding author: TEH EXODUS AKWA 1Department of Biochemistry, Microbiology and Biotechnology, Kenyatta University, Nairobi, Kenya 2Department of Plant Sciences, Kenyatta University, Nairobi, Kenya *Corresponding author: [email protected]; Tel.: +254 792 775729; Medical Microbiology, Department of Biochemistry, Microbiology and Biotechnology, Kenyatta University, Nairobi, Kenya, P.O BOX 43844-00100-NAIROBI 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.10.31.363184; this version posted November 1, 2020. The copyright holder has placed this preprint (which was not certified by peer review) in the Public Domain. It is no longer restricted by copyright. Anyone can legally share, reuse, remix, or adapt this material for any purpose without crediting the original authors. CHARACTERISATION OF FUNGI OF STORED COMMON BEAN CULTIVARS GROWN IN MENOUA DIVISION, CAMEROON. Abstract Common bean is a legume grown globally especially in developing countries including Cameroon for human consumption. In Cameroon it is grown in a wide variety of agro ecological zones in quantities enough to last through the off growing season after harvest. Stored common bean after harvest in Cameroon are prone to fungal spoilage which contributes to post harvest losses. -

Cameroun-Tchad-Projet De Pont Sur Le Logone-Resume EIES 07 2017.Docx
AFRICAN DEVELOPMENT BANK GROUP PROJECT: LAKE CHAD BASIN REGIONAL INTEGRATIVE ROAD NETWORK PROJECT - CONSTRUCTION OF A BRIDGE OVER RIVER LOGONE BETWEEN YAGOUA IN CAMEROON AND BONGOR IN CHAD COUNTRY: MULTINATIONAL-CAMEROON/CHAD ENVIRONMENTAL AND SOCIAL IMPACT ASSESSMENT (ESIA) SUMMARY J.K. NGUESSAN, Chief Transport Team Leader PICU.1/COCM 6830 Engineer Jean P. MEGNE, Transport Economist PICU.1/COCD 6368 P. MORE NDONG, Principal Transport PICU.1/COMA 7331 Engineer P. HORUGAVYE, Chief Socio-Economist SNSC 2543 Team Members C. DJEUFO, Procurement Officer SNFI.1/COCM 6809 Project Team M. KINANE, Principal Environmentalist SNSC 2233 D. TILENGAR, Procurement Officer SNFI.1/COTD 6207 Sector Division Mr. Jean Kizito KABANGUKA PICU.1 2143 Manager Sector Director Mr. Amadou OUMAROU PICU 3075 Director General Mr. Ousmane DORE RDGC 2251 ENVIRONMENTAL AND SOCIAL IMPACT ASSESSMENT (ESIA) SUMMARY Project Name: Lake Chad Basin Regional Integrative Road Network Project Code SAP : P-Z1- - Construction of a Bridge over River Logone between Yagoua in Cameroon DB0-181 and Bongor in Chad Country : Multinational Cameroon-Chad Category 1 Department : OITC Division: OITC-1 1. INTRODUCTION This document is the Environmental and Social Impact Assessment (ESIA) Summary of the Lake Chad Basin Regional Integrative Road Network Project - construction of the bridge over River Logone between Yagoua, Cameroon and Bongor, Chad. This ESIA covers the road and ancillary works except the Yagoua bypass. It has been prepared in accordance with AfDB environmental and social assessment -
CAMEROON Situation Report Last Updated: 8 Oct 2020
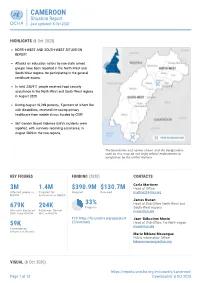
CAMEROON Situation Report Last updated: 8 Oct 2020 HIGHLIGHTS (8 Oct 2020) NORTH-WEST AND SOUTH-WEST SITUATION REPORT Attacks on education actors by non-state armed groups have been reported in the North-West and South-West regions for participating in the general certificate exams. In total 245,911 people received food security assistance in the North-West and South-West regions in August 2020. During August 10,249 patients, 5 percent of whom live with disabilities, received life-saving primary healthcare from mobile clinics funded by CERF. 567 Gender Based Violence (GBV) incidents were reported, with survivors receiving assistance, in August 2020 in the two regions. The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations. KEY FIGURES FUNDING (2020) CONTACTS Carla Martinez 3M 1.4M $390.9M $130.7M Head of Office Affected people in Targeted for Required Received [email protected] NWSW assistance in NWSW ! j e r d n , A y James Nunan r r o S 33% Head of Sub-Office North-West and 679K 204K Progress South-West regions Internally displaced Returnees (former [email protected] (IDP) from NWSW IDP) in NWSW FTS: https://fts.unocha.org/appeals/9 Jean-Sébastien Munie 27/summary Head of Sub-Office, Far-North region 59K [email protected] Cameroonian refugees in Nigeria Marie Bibiane Mouangue Public information Officer [email protected] VISUAL (8 Oct 2020) https://reports.unocha.org/en/country/cameroon/ Page 1 of 13 Downloaded: 8 Oct 2020 CAMEROON Situation Report Last updated: 8 Oct 2020 Map of IDP, Returnees and Refugees from the North-West and South-West Regions of Cameroon Source: OCHA, UNHCR, IOM The boundaries and names shown, and the designations used on this map do not imply official endorsement or acceptance by the United Nations. -

Onchocerciasis Prevalence and Transmission Potential of Simulium Spp
Diseas al es ic & OPEN ACCESS Freely available online p P ro u T b l f i c o H l a e n a r Journal of Tropical Diseases and Public l t u h o J ISSN: 2329-891X Health Research Article Onchocerciasis Prevalence and Transmission Potential of Simulium spp. in Three Areas of the Northern Regions of Cameroonl Sanda Amadou1, Djafsia Boursou2, Pierre Saotoing3, Dieudonné Ndjonka1* 1Department of Biological Sciences, University of Ngaoundere, Ngaoundere, Cameroon; 2Department of Fundamental Sciences, University of Ngaoundere, Garoua, Cameroon; 3Department of Life and Earth Sciences of Higher Teachers’ Training College, University of Maroua, Cameroon ABSTRACT Background: Onchocerciasis is an infection caused by Onchocerca volvulus: A filarial nematode transmitted by Simulium spp. More than 99% of infected people live in 30 countries in sub-Saharan Africa, 37 million people are carriers of Onchocerca volvulus in Central and East Africa, and 800,000 blinds people are recorded. Villages in northern Cameroon had more than 80% microfilaria index in 1991 with bilateral blindness rates 1.7% to 4.0%. Methods: Three villages have been selected to study: Lagaye in the district of Touboro, Mandjiri in the department of Vina (Adamawa), and Mayo-Salah in Mayo Rey Department. Concerning the parasitological research, the persons to be examined have been gathered by sex (female and male) and age group. Three age groups were concerned: 5 to 9 years, 10 to 15 years, and beyond 16 years. Using a vaccine style and a razor blade, a 2 mm fragment of skin was removed from the scapula, iliac crest, and calf. -

Boko Haram Beyond the Headlines: Analyses of Africa’S Enduring Insurgency
Boko Haram Beyond the Headlines: Analyses of Africa’s Enduring Insurgency Editor: Jacob Zenn Boko Haram Beyond the Headlines: Analyses of Africa’s Enduring Insurgency Jacob Zenn (Editor) Abdulbasit Kassim Elizabeth Pearson Atta Barkindo Idayat Hassan Zacharias Pieri Omar Mahmoud Combating Terrorism Center at West Point United States Military Academy www.ctc.usma.edu The views expressed in this report are the authors’ and do not necessarily reflect those of the Combating Terrorism Center, United States Military Academy, Department of Defense, or U.S. Government. May 2018 Cover Photo: A group of Boko Haram fighters line up in this still taken from a propaganda video dated March 31, 2016. COMBATING TERRORISM CENTER ACKNOWLEDGMENTS Director The editor thanks colleagues at the Combating Terrorism Center at West Point (CTC), all of whom supported this endeavor by proposing the idea to carry out a LTC Bryan Price, Ph.D. report on Boko Haram and working with the editor and contributors to see the Deputy Director project to its rightful end. In this regard, I thank especially Brian Dodwell, Dan- iel Milton, Jason Warner, Kristina Hummel, and Larisa Baste, who all directly Brian Dodwell collaborated on the report. I also thank the two peer reviewers, Brandon Kend- hammer and Matthew Page, for their input and valuable feedback without which Research Director we could not have completed this project up to such a high standard. There were Dr. Daniel Milton numerous other leaders and experts at the CTC who assisted with this project behind-the-scenes, and I thank them, too. Distinguished Chair Most importantly, we would like to dedicate this volume to all those whose lives LTG (Ret) Dell Dailey have been afected by conflict and to those who have devoted their lives to seeking Class of 1987 Senior Fellow peace and justice. -

Cameroon Watershed
Journal(of(Materials(and(( J. Mater. Environ. Sci., 2018, Volume 9, Issue 11, Page 3094-2104 Environmental(Sciences( ISSN(:(2028;2508( CODEN(:(JMESCN( http://www.jmaterenvironsci.com! Copyright(©(2018,( University(of(Mohammed(Premier(((((( (Oujda(Morocco( A typological study of the physicochemical quality of water in the Menoua- Cameroon watershed Santsa Nguefack Charles Vital1*, Ndjouenkeu Robert1, Ngassoum Martin Benoit2 , 1Laboratory of Food Physicochemistry, Department of Food Science and Nutrition National Advanced School of Agro- Industrial Sciences, University of Ngaoundéré, PO BOX 455,Ngaoundéré, Cameroon. 2Department of Industrial Chemistry and Environment, National Advanced School of Agro-Industrial Sciences, University of Ngaoundéré, PO BOX 455, Ngaoundéré, Cameroon. Received 29 Oct 2017 Abstract Revised 25 Dec 2018 Cameroon, a country in Central Africa with an outlet to the Atlantic Ocean in the Gulf Accepted 28 Dec 2018 of Guinea, holds enormous potentialities of water resources. These resources used for the supply of water for human consumption, etc., would be polluted by the Keywords intensification of anthropogenic activities, of which the most important recorded in the !!physicochemical, Menoua watershedof West Cameroon are agriculture and breeding. The objective of this !!pollution, work was to study the spatiotemporal parameters of the physicochemical quality !!Menoua watershed, parameters (temperature, pH, electrical conductivity, Turbidity, Nitrates, Ortho !!Anthropogenic Phosphates, Sulphates, Chloride, Potassium and Calcium) the Menoua activities, watershedthrough a main Principal Component Analysis (ACP). The results obtained showed that the pH, turbidity and orthophosphate have levels which are in contradiction !!Water for human consumption. with WHO standards. The physicochemical parameters of this water showed significant spatial and seasonal variations, the causes of which probably related to the human activities generating pollutants. -

CAMEROON: LOCATIONS of UNHCR PERSONS of CONCERN (January 2021)
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (January 2021) ! Maïné-Soroa DIFFA LAC KANEM BARH EL Magaria ZINDER ! PERSONS OF CONCERN GHAZEL e Gashua gu Yob ! 1,960,832 ! omadu K Geidam KATSINA Guri CAR REFUGEES IN! CAMEROON WATER BODY 316,017 HADJER-LAMIS NIG REFUGHEaEdeSji aIN CAMEROON ! YOBE Jakusko 117,826 ! C OTHER NATIONALITIES ha JIGAWA ri 2,466 Kousseri N'Djamena a Kano i ! j e ASYLUM SEEKERS d Maiduguri a LOGONE 7H ,545 Damaturu ET CHARI INTERNALLY DISPLACED PERSOPoNtisSk u(mIDPs) * 1,032,942 ! BORNO C h KANO a r RETURNEES * Waza i 465,757 Waza a g CHARI-BAGUIRMI CAMERuOn ONIAN REFUGEES Limani Magdeme RETURBNED FORM NIGERIA* 18,279 MAYO SAVA ola Gong Mora Number of refugees EXTRÊME-NORD < 10,000 ! Mokolo DIAMARÉ Biu BAUCHI ! Maroua MAYO-KEBBI < 50,000 GOMBE Minawao MAYO EST ! TSANAGA Yagoua Bauchi ! Gombe ! !Mubi Deba MAYO KANI MAYO DANAY > 75000 ! KADUNA Kaele MAYO LOUTI Jos Guider !! Number of IDPs Lo go Lafia Ləre ne N I G E R I A ! ! < 10,000 ADAMAWA ! TANDJILÉ B Yola é n MAYO-KEBBI < 50,000 o u ! BÉNOUÉ é OUEST C H A D PLATEAU Jalingo > 75000 LOGONE NORD OCCIDENTAL ! e u ! Number of returnees en Moundou !Lafia B Poli Tchollire NASSARAWA< 10,000 ! FARO LOGONE MAYO REY < 50,000 ORIENTAL Gondje ! Wukari Amboko ! Touboro TARABA Dosseye !Makurdi Beke Chantier > 75000 Vina FARO ET DÉO Tingere ! Beka Number of asylum seekers BENUE Paoua Ndip ! < 10,000 VINA !Bocaranga Number of refugees returned Borgop OUHAM Djohong < 10,000 Banyo ADAMAOUA OUHAM-PENDÉ ! Nkambe Ngam NORD-OUEST Kounde MENCHUM DJEREM Meiganga DONGA MANTUNG Tibati -

Shelter Cluster Dashboard NWSW052021
Shelter Cluster NW/SW Cameroon Key Figures Individuals Partners Subdivisions Cameroon 03 23,143 assisted 05 Individual Reached Trend Nigeria Furu Awa Ako Misaje Fungom DONGA MANTUNG MENCHUM Nkambe Bum NORD-OUEST Menchum Nwa Valley Wum Ndu Fundong Noni 11% BOYO Nkum Bafut Njinikom Oku Kumbo Belo BUI Mbven of yearly Target Njikwa Akwaya Jakiri MEZAM Babessi Tubah Reached MOMO Mbeggwi Ngie Bamenda 2 Bamenda 3 Ndop Widikum Bamenda 1 Menka NGO KETUNJIA Bali Balikumbat MANYU Santa Batibo Wabane Eyumodjock Upper Bayang LEBIALEM Mamfé Alou OUEST Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Fontem Nguti KOUPÉ HNO/HRP 2021 (NW/SW Regions) Toko MANENGOUBA Bangem Mundemba SUD-OUEST NDIAN Konye Tombel 1,351,318 Isangele Dikome value Kumba 2 Ekondo Titi Kombo Kombo PEOPLE OF CONCERN Abedimo Etindi MEME Number of PoC Reached per Subdivision Idabato Kumba 1 Bamuso 1 - 100 Kumba 3 101 - 2,000 LITTORAL 2,001 - 13,000 785,091 Mbongé Muyuka PEOPLE IN NEED West Coast Buéa FAKO Tiko Limbé 2 Limbé 1 221,642 Limbé 3 [ Kilometers PEOPLE TARGETED 0 15 30 *Note : Sources: HNO 2021 PiN includes IDP, Returnees and Host Communi�es The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Key Achievement Indicators PoC Reached - AGD Breakdouwn 296 # of Households assisted with Children 27% 26% emergency shelter 1,480 Adults 21% 22% # of households assisted with core 3,769 Elderly 2% 2% relief items including prevention of COVID-19 21,618 female male 41 # of households assisted with cash for rental subsidies 41 Households Reached Individuals Reached Cartegories of beneficiaries reported People Reached by region Distribution of Shelter NFI kits integrated with COVID 19 KITS in Matoh town. -

The Boko Haram Conflict in Cameroon Why Is Peace So Elusive? Pr
Secur nd ity a S e e c r i a e e s P FES Pr. Ntuda Ebode Joseph Vincent Pr. Mark Bolak Funteh Dr. Mbarkoutou Mahamat Henri Mr. Nkalwo Ngoula Joseph Léa THE BOKO HARAM CONFLICT IN CAMEROON Why is peace so elusive? Pr. Ntuda Ebode Joseph Vincent Pr. Mark Bolak Funteh Dr. Mbarkoutou Mahamat Henri Mr. Nkalwo Ngoula Joseph Léa THE BOKO HARAM CONFLICT IN CAMEROON Why is peace so elusive? Translated from the French by Diom Richard Ngong [email protected] © Friedrich Ebert Stiftung, Yaoundé (Cameroun), 2017. Tél. 00 237 222 21 29 96 / 00 237 222 21 52 92 B.P. 11 939 Yaoundé / Fax: 00 237 222 21 52 74 E-mail : [email protected] Site : www.fes-kamerun.org Réalisation éditoriale : PUA : www.aes-pua.com ISBN: 978-9956-532-05-3 Any commercial use of publications, brochures or other printed materials of the Friedrich Ebert Stiftung is strictly forbidden unless otherwise authorized in writing by the publisher This publication is not for sale All rights reserved No part of this book may be reproduced in any form, by print, photo print, microfilm, translation or other means without written permission from the publisher TABLE OF CONTENTS Acknowledgements ………………………………………………….....……………....................…………..................... 5 Abbreviations and acronyms ………………………………………...........…………………………….................... 6 Introduction ………………………………………………………………………....................………………....….................... 7 Chapter I – Background and context of the emergence of Boko Haram in Cameroon ……………………………………………………………………………………....................………….................... 8 A. Historical background to the crisis in the Far North region ……………..……….................... 8 B. Genesis of the Boko Haram conflict ………………………………………………..................................... 10 Chapter II - Actors, challenges and prospects of a complex conflict ……………....... 12 A. Actors and the challenges of the Boko Haram conflict …………………………….....................12 1. -

N I G E R I a C H a D Central African Republic Congo
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (September 2020) ! PERSONNES RELEVANT DE Maïné-Soroa !Magaria LA COMPETENCE DU HCR (POCs) Geidam 1,951,731 Gashua ! ! CAR REFUGEES ING CurAi MEROON 306,113 ! LOGONE NIG REFUGEES IN CAMEROON ET CHARI !Hadejia 116,409 Jakusko ! U R B A N R E F U G E E S (CENTRAL AFRICAN REPUBLIC AND 27,173 NIGERIAN REFUGEE LIVING IN URBAN AREA ARE INCLUDED) Kousseri N'Djamena !Kano ASYLUM SEEKERS 9,332 Damaturu Maiduguri Potiskum 1,032,942 INTERNALLY DISPLACED PERSO! NS (IDPs) * RETURNEES * Waza 484,036 Waza Limani Magdeme Number of refugees MAYO SAVA Mora ! < 10,000 EXTRÊME-NORD Mokolo DIAMARÉ Biu < 50,000 ! Maroua ! Minawao MAYO Bauchi TSANAGA Yagoua ! Gom! be Mubi ! MAYO KANI !Deba MAYO DANAY < 75000 Kaele MAYO LOUTI !Jos Guider Number! of IDPs N I G E R I A Lafia !Ləre ! < 10,000 ! Yola < 50,000 ! BÉNOUÉ C H A D Jalingo > 75000 ! NORD Moundou Number of returnees ! !Lafia Poli Tchollire < 10,000 ! FARO MAYO REY < 50,000 Wukari ! ! Touboro !Makurdi Beke Chantier > 75000 FARO ET DÉO Tingere ! Beka Paoua Number of asylum seekers Ndip VINA < 10,000 Bocaranga ! ! Borgop Djohong Banyo ADAMAOUA Kounde NORD-OUEST Nkambe Ngam MENCHUM DJEREM Meiganga DONGA MANTUNG MAYO BANYO Tibati Gbatoua Wum BOYO MBÉRÉ Alhamdou !Bozoum Fundong Kumbo BUI CENTRAL Mbengwi MEZAM Ndop MOMO AFRICAN NGO Bamenda KETUNJIA OUEST MANYU Foumban REPUBLBICaoro BAMBOUTOS ! LEBIALEM Gado Mbouda NOUN Yoko Mamfe Dschang MIFI Bandjoun MBAM ET KIM LOM ET DJEREM Baham MENOUA KOUNG KHI KOUPÉ Bafang MANENGOUBA Bangangte Bangem HAUT NKAM Calabar NDÉ SUD-OUEST -
De 40 MINMAP Région Du Nord SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES
MINMAP Région du Nord SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES Nbre de N° Désignation des MO/MOD Montant des Marchés N° Page Marchés 1 Communauté Urbaine de Garoua 11 847 894 350 3 2 Services déconcentrés régionaux 20 528 977 000 4 Département de la Bénoué 3 Services déconcentrés départementaux 10 283 500 000 6 4 Commune de Barndaké 13 376 238 000 7 5 Commune de Bascheo 16 305 482 770 8 6 Commune de Garoua 1 11 201 187 000 9 7 Commune de Garoua 2 26 498 592 344 10 8 Commune de Garoua 3 22 735 201 727 12 9 Commune de Gashiga 21 353 419 404 14 10 Commune de Lagdo 21 2 026 560 930 16 11 Commune de Pitoa 18 360 777 700 18 12 Commune de Bibémi 18 371 277 700 20 13 Commune de Dembo 11 300 277 700 21 14 Commune de Ngong 12 235 778 000 22 15 Commune de Touroua 15 187 777 700 23 TOTAL 214 6 236 070 975 Département du Faro 16 Services déconcentrés 5 96 500 000 25 17 Commune de Beka 15 230 778 000 25 18 Commune de Poli 22 481 554 000 26 TOTAL 42 808 832 000 Département du Mayo-Louti 19 Services déconcentrés 6 196 000 000 28 20 Commune de Figuil 16 328 512 000 28 21 Commune de Guider 28 534 529 000 30 22 Commune de Mayo Oulo 24 331 278 000 32 TOTAL 74 1 390 319 000 MINMAP / DIVISION DE LA PROGRAMMATION ET DU SUIVI DES MARCHES PUBLICS Page 1 de 40 MINMAP Région du Nord SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES Nbre de N° Désignation des MO/MOD Montant des Marchés N° Page Marchés Département du Mayo-Rey 23 Services déconcentrés 7 152 900 000 35 24 Commune de Madingring 14 163 778 000 35 24 Commune de Rey Bouba