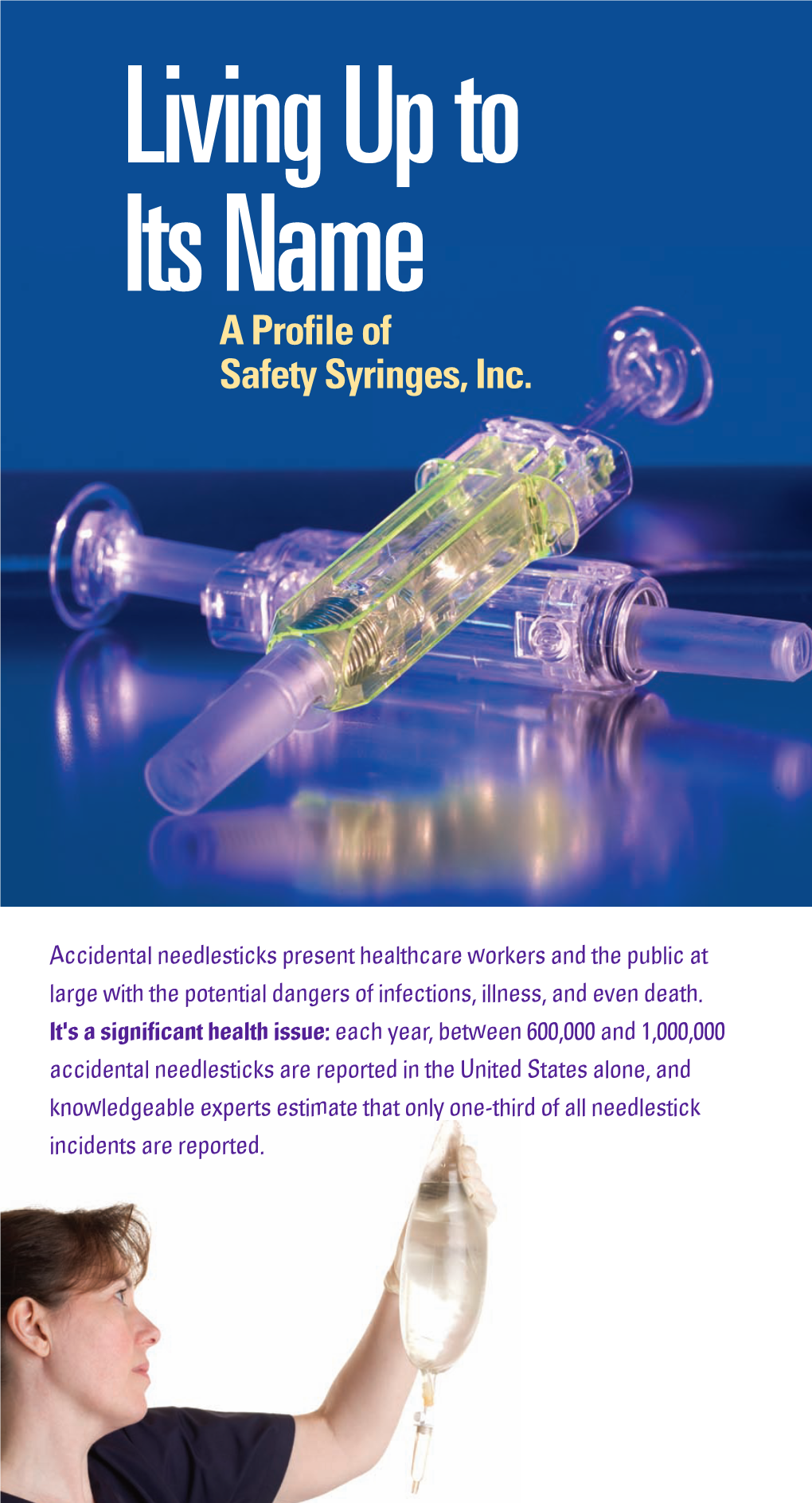
Safety Syringes Inc. Customer Story
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Healthy Action: an Activity Book for Teachers and Learners
Healthy Action: An Activity Book for Teachers and Learners Acknowledgements This Activity Book was written by Scott Pulizzi and Laurie Rosenblum of Education Development Center, Inc. (EDC), Health and Human Development Division (HHD). The authors worked in close partnership with the staff of the Solidarity and Development Unit coordinating the EFAIDS Programme at Education International (EI). The authors acknowledge the contribution of the World Health Organization (WHO). EI, EDC, and WHO would also like to acknowledge all the teachers’ unions affiliated to EI who have contributed to the EFAIDS Programme and thus to this Activity Book, specifically and the Zimbabwe Teachers’ Association. EI, EDC, and WHO are supported by the Dutch Ministry of Foreign Affairs’ Directorate- General for International Cooperation (DGIS) under the EFAIDS Programme. All photographs taken by Josephine Krikke. Acknowledgements 3 Table of Contents Introduction ................................................... 7 Tobacco Use and Prevention .......................... 11 Alcohol and Other Drugs................................ 27 Nutrition ......................................................... 37 Physical Activity ............................................. 55 Hygiene and Sanitation .................................. 69 Injury Prevention ........................................... 83 Violence Prevention ........................................ 95 Table of Contents 5 Introduction This toolkit is based on the premise that healthy students and teachers live better. -

PERSONAL and COMMUNITY HEALTH (PCH): 14 Days
MIDDLE SCHOOL (GRADE 7) HEALTH EDUCATION UNIT PLANNING GUIDE (revised 6/2009) Page 1 of 15 PERSONAL AND COMMUNITY HEALTH (PCH): 14 days Text Chapter 1, 2, 5 Chapters 12, 13 Chapter 15 Chapter 15 Sub-Unit: Personal Health Sub-Unit: Disease Prevention Sub-Unit: Environmental Health Sub-Unit: Community Health EC 1.1.P Describe the 1.3.P Identify Standard 1.9.P Identify ways that 1.11.P Describe global influences importance of health- (Universal) Precautions and why environmental factors, including on personal and community health. management strategies (e.g., they are important. (also IPS, air quality, affect our health. those involving adequate sleep, GDSH) 1.10.P Identify human activities ergonomics, sun safety, 1.4.P Examine the causes and that contribute to environmental hearing protection, and self symptoms of communicable and challenges (e.g., air, water an noise examination). non-communicable diseases. pollution). 1.2.P Identify the importance of age-appropriate medical services. 1.5.P Discuss the importance of effective personal and dental hygiene practices for preventing illness. 1.6.P Identify effective brushing and flossing techniques for oral care. 1.7.P Identify effective protection for teeth, eyes, head, and neck during sports and recreation activities. (also IPS) 1.8.P Identify ways to prevent vision or hearing damage. 1.12.P Identify ways to reduce exposure to the sun. AI 2.1.P Analyze a variety of 2.2.P Analyze how environmental influences that affect personal pollutants, including noise pollution, health practices. affect health. 2.4.P Analyze the influence of 2.3.P Analyze the relationship culture, media, and technology on between the health of a community health decisions. -

Federal Register / Vol. 62, No. 221 / Monday, November 17, 1997 / Notices Respondent Burden
61336 Federal Register / Vol. 62, No. 221 / Monday, November 17, 1997 / Notices respondent burden. The total annual burden hours are 500. No. of Avg. burden/ Project No. of responses/ response respondents respondent (in hrs.) QDRL Laboratory Interviews: (1) NHIS modules ................................................................................................................. 150 1 1.0 (2) Behavioral Risk Factors Survey ...................................................................................... 100 1 1.0 (3) Other Questionnaire Testing: .......................................................................................... 1998 ............................................................................................................................... 200 1 1.0 1999 ............................................................................................................................... 200 1 1.0 2000 ............................................................................................................................... 200 1 1.0 (4) Perceptions of Quality of Life Project .............................................................................. 100 1 1.0 (5) Perceptions of Confidentiality Project ............................................................................. 50 1 1.0 (6) Perception of Statistical Maps Project ............................................................................ 100 1 1.0 (7) General Methodological Research ................................................................................. -

The Opioid Epidemic & Workplace Injury Prevention
Subscribe to our newsletters at https://www.backsafe.com/contact-fit/ The Opioid Epidemic & Workplace Injury Prevention According to Consumer Reports over 50% of Americans are taking prescription medication in this country. Pharmaceuticals are a $450 billion industry. Medications do a lot of good for so many people, but most of us would agree that we are an over- prescribed nation. This is no more evident than with the national opioid epidemic. The US Centers for Disease Control and Prevention state that 91 people die every day from opioid overdose. This epidemic is a tragedy for so many people and their families. The stories are heart breaking, but not surprising. When a drug can mask pain with a false sensation of well-being, no wonder it is highly addictive. The opioid crisis is costing US companies over $500 billion per year in absenteeism and lost production according to marketwatch.com. What can employers do to counter this cultural pharmaceutical trend? Pain is the enemy of us all. I recently asked an audience at a National Safety Conference “Who here is experiencing pain or discomfort on any part of your body?” Almost 100% raised their hands. I asked “Why are you putting up with it?” I got an expected silence because most people inexplicably just live with it. Why is that? Why do we allow discomfort and pain to settle in on our bodies to affect our quality of life? Why do we let stiff muscles and joints insidiously restrict range of motion over time and make us feel old? We falsely assign this accumulation of “micro-trauma” to aging! FIT discovered during our initial research 25 years ago, one of society’s biggest oversights. -

Immunization of Adults and Children in the Emergency Department
POLICY STATEMENT Approved October 2020 Immunization of Adults and Children in the Emergency Department Revised October 2020, The American College of Emergency Physicians (ACEP) recognizes that June 2015 vaccine-preventable infectious diseases have a significant effect on the health Originally approved January of adults and children. The emergency department (ED) is used frequently for 2008, replacing health care by many inadequately vaccinated adults and children who are at “Immunizations in the risk for such diseases. EDs serve as a primary interface between hospitals and Emergency Department” the community at large and have been on the frontlines of infectious or (2002), “Immunization of biological threats. To promote the health and well-being of individual patients Pediatric Patients” (2000), and “Immunization of Adult and the population, ACEP thus supports the following principles: Patients” (2000) • Immunization against vaccine-preventable diseases, including the seasonal influenza vaccine, should be ensured for all physicians, nurses, and advanced practitioners in the absence of appropriate medical contraindications or exemptions. • ED physicians, nurses, and advanced practitioners should have current knowledge of, or access to, recommended vaccination administration schedules. Utilization of resources embedded within the electronic medical record or through web or app-based resources is encouraged.1 • Electronic vaccination records should be accessible to all emergency physicians. • EDs should establish relationships with public -

Injury Surveillance Guidelines
WHO/NMH/VIP/01.02 DISTR.: GENERAL ORIGINAL: ENGLISH INJURY SURVEILLANCE GUIDELINES Edited by: Y Holder, M Peden, E Krug, J Lund, G Gururaj, O Kobusingye Designed by: Health & Development Networks http://www.hdnet.org Published in conjunction with the Centers for Disease Control and Prevention, Atlanta, USA, by the World Health Organization 2001 Copies of this document are available from: Injuries and Violence Prevention Department Non-communicable Diseases and Mental Health Cluster World Health Organization 20 Avenue Appia 1211 Geneva 27 Switzerland Fax: 0041 22 791 4332 Email: [email protected] The content of this document is available on the Internet at: http://www.who.int/violence_injury_prevention/index.html Suggested citation: Holder Y, Peden M, Krug E et al (Eds). Injury surveillance guidelines. Geneva, World Health Organization, 2001. WHO/NMH/VIP/01.02 © World Health Organization 2001 This document is not a formal publication of the World Health Organization (WHO). All rights are reserved by the Organization. The document may be freely reviewed, abstracted, reproduced or translated, in part or in whole, but may not be sold or used for commercial purposes. The views expressed in documents by named authors are the responsibility of those authors. ii Contents Acronyms .......................................................................................................................... vii Foreword .......................................................................................................................... viii Editorial -

CDC Childhood Injury Report
CDC Childhood Injury Report: Patterns of Unintentional Injuries among 0-19 Year Olds in the United States, 2000-2006 US DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR DISEASE CONTROL AND PREVENTION Keeping our children safe and helping them live to their full potential 1 CDC Childhood Injury Report: Patterns of Unintentional Injuries among 0-19 Year Olds in the United States, 2000-2006 Nagesh N. Borse, Ph.D. M.S. Julie Gilchrist, MD Ann M. Dellinger, Ph.D. Rose A. Rudd, MSPH Michael F. Ballesteros, Ph.D. David A. Sleet, Ph.D. U. S. Department of Health and Human Services Centers for Disease Control and Prevention National Center for Injury Prevention and Control Division of Unintentional Injury Prevention Atlanta, GA December 2008 1 The CDC Childhood Injury Report: Patterns of Unintentional Injuries among 0-19 Year Olds in the United States, 2000-2006 is a publication of the National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Centers for Disease Control and Prevention Julie L. Gerberding, MD, MPH, Director Coordinating Center for Environmental Health and Injury Prevention Henry Falk, MD, MPH, Director National Center for Injury Prevention and Control Ileana Arias, PhD, Director Division of Unintentional Injury Prevention Grant Baldwin, PhD, MPH, Director Authors Nagesh N. Borse, Ph.D. M.S. Julie Gilchrist, MD Ann M. Dellinger, Ph.D. Rose A. Rudd, MSPH Michael F. Ballesteros, Ph.D. David A. Sleet, Ph.D. Acknowledgments The authors would like to acknowledge the contributions of the following individuals: Grant Baldwin, Laurie Beck, Rebecca Boyd, Shelley Hammond, Michele Huitric, Scott Kegler, Shelly Prescod, Chet Pogostin, Caryll Rinehart, Robert Thomas, Karen Thomas, James Tobias, Kevin Webb, Bethany West, and Dionne Williams Suggested Citation: Borse NN, Gilchrist J, Dellinger AM, Rudd RA, Ballesteros MF, Sleet DA. -

Chapter 5: Injury Prevention and Infection Control
Chapter 5 Injury Prevention & Infection Control Chapter 5: Injury Prevention and Infection Control Childhood Injury Prevention p. 149 Bicycle safety p. 150 Burn prevention p. 150 Choking hazard safety p. 151 Emergency preparedness p. 152 Emergency supplies list p. 154 - First aid kit list p. 154 Fall prevention p. 155 Infant safe sleep p. 156 Motor vehicle safety p. 158 - Car safety seats p. 158 - Kids in hot cars p. 159 Poison prevention p. 160 Suffocation & strangulation prevention p. 160 Sun safety p. 161 Water safety p. 161 Weapons and ammunition safety p. 162 Infection Control p. 163 Appropriate antibiotic use p. 164 Communicable disease p. 165 Cover Your Cough p. 165 Decrease the spread of disease p. 166 Outbreaks of illness p. 166 Proper diapering procedures p. 167 - Diaper rash p. 168 Proper hand washing procedures p. 169 Universal (Standard) precautions p. 169 Updated bleach /water concentration information p. 171 147 Good Health Handbook 2015 Chapter 5 Injury Prevention & Infection Control 148 Good Health Handbook 2015 Chapter 5 Injury Prevention & Infection Control Childhood Injury Prevention Injury prevention is the understanding that injuries are not random uncontrollable events, but preventable, with identifiable risk factors. Many injuries happen in predictable, preventable ways. As a child care provider, you are responsible for the health and safety of the children in your care. A healthy and safe environment for children means they can live and play in your facility or home free from harm. Keys to a SAFE environment Supervise – close supervision of children at all times. Anticipate – ask yourself “What are the possible hazards?” Formulate – make a plan by asking “What do I do if……..?” Educate – educate all providers and children of possible hazards in the environment. -

National Action Plan for Child Injury Prevention | 2012
NATIONAL ACTION PLAN for CHILD INJURY PREVENTION An Agenda to Prevent Injuries and Promote the Safety of Children and Adolescents in the United States The National Action Plan for Child Injury Prevention is a publication of the National Center for Injury Prevention and Control of the Centers for Disease Control and Prevention. Centers for Disease Control and Prevention Thomas R. Frieden, MD, MPH, Director National Center for Injury Prevention and Control Linda C. Degutis, DrPH, MSN, Director Division of Unintentional Injury Prevention Grant T. Baldwin, PhD, MPH, Director Suggested citation: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. National Action Plan for Child Injury Prevention. Atlanta (GA): CDC, NCIPC; 2012 NATIONAL ACTION PLAN for CHILD INJURY PREVENTION An Agenda to Prevent Injuries and Promote the Safety of Children and Adolescents in the United States 2012 U.S. Department of Health and Human Services Centers for Disease Control and Prevention National Center for Injury Prevention and Control very day in the United States, two dozen children die from an injury that was not intended. Such tragedy often leaves families broken apart and changes the lives of those left behind. Injury deaths, however, are only part of the picture. Each year, millions of children in the United States are injured and live with the Econsequences of those injuries. These children may face disability and chronic pain that limit their ability to perform age-appropriate everyday activities over their lifetime. These deaths and injuries need not occur because they often result from predictable events. The good news is that we have solutions that work to prevent child injury. -

AAP an Essential Force in Protecting Children from Injury, Gun Violence, Disease by Kyle E
News Articles, Letter from the President, Advocacy, Infectious Diseases, Injury, Violence & Poison Prevention, Vaccine/Immunization AAP an essential force in protecting children from injury, gun violence, disease by Kyle E. Yasuda M.D., FAAP, President, American Academy of Pediatrics Prevention is at the heart of pediatrics. During the first half of 2019, the Academy has worked overtime to promote health and protect children from infectious diseases, injury and gun violence. Protecting against global measles virus Last month, the United States reached a regrettable milestone when the number of measles cases reached its highest total in 25 years. When the first cases were announced, the AAP responded with a multipronged approach to quash measles outbreaks and contain the spread of the virus. We worked to strengthen parents' confidence in the safety and lifesaving power of vaccines through traditional and social media. And because many parents struggle with fear due to anti-vaccine content on social media and other online sources, we reached out to Google, Facebook and Pinterest and urged them to elevate evidence- based information on immunizations. Shortly after, we began working with Pinterest, and Facebook announced it will change its algorithm to make sure its users see credible, science-based information. In addition, we continue to urge state lawmakers to eliminate nonmedical exemptions to school vaccination requirements to make it harder for parents to opt out. We are consulting with the Centers for Disease Control and Prevention on a comprehensive strategy to increase parents' confidence in vaccines, address barriers to vaccination and improve access to vaccines in all communities. -

Injury Prevention
AMERICAN COLLEGE OF SURGEONS Committee on Trauma Injury Prevention Presented by the Subcommittee on Injury Prevention and Control AMERICAN COLLEGE OF SURGEONS Committee on Trauma Injury Prevention Presented by the Subcommittee on Injury Prevention and Control Slide 1: Title Injury Prevention Slide 2: The purpose of this presentation is to increase the awareness by the health care community of the disease Introduction and called “injury” and the concept of injury control. Purpose The objectives are to: • Characterize injury as a public health problem • Detail the impact of injury on American society • Identify control strategies and demonstrate how these can be applied to injury • Highlight the key elements of effective, community- based prevention projects • Address obstacles to prevention activities • Identify resources for developing and conducting prevention programs • Identify the role of the health care provider in prevention activities Slide 3: Injury can be described as physical damage produced by the transfer of energy, such as kinetic, thermal, Definition chemical, electrical, or radiant. It can also be due to the absence of oxygen or heat. The interval of time over which the energy transfer or the deprivation of physiologic essentials occurs is known as “exposure.” The exposure may be acute or chronic. 1 Slide 4: One of the most current information sources available on the health status of the nation is Health, United States, Frequency 1998.1 The information in this slide text is taken from that source and other comparable sources. Each year, 59 million Americans, (1 in every 4), sustain an injury. Not all injuries are fatal or serious enough to require inpatient care, but the total volume requires a tremendous allocation of health care resources. -

PREVENTING DISEASE THROUGH HEALTHY ENVIRONMENTS This Report Summarizes the Results Globally, by 14 Regions Worldwide, and Separately for Children
How much disease could be prevented through better management of our environment? The environment influences our health in many ways — through exposures to physical, chemical and biological risk factors, and through related changes in our behaviour in response to those factors. To answer this question, the available scientific evidence was summarized and more than 100 experts were consulted for their estimates of how much environmental risk factors contribute to the disease burden of 85 diseases. PREVENTING DISEASE THROUGH HEALTHY ENVIRONMENTS This report summarizes the results globally, by 14 regions worldwide, and separately for children. Towards an estimate of the environmental burden of disease The evidence shows that environmental risk factors play a role in more than 80% of the diseases regularly reported by the World Health Organization. Globally, nearly one quarter of all deaths and of the total disease burden can be attributed to the environment. In children, however, environmental risk factors can account for slightly more than one-third of the disease burden. These findings have important policy implications, because the environmental risk factors that were studied largely can be modified by established, cost-effective interventions. The interventions promote equity by benefiting everyone in the society, while addressing the needs of those most at risk. ISBN 92 4 159382 2 PREVENTING DISEASE THROUGH HEALTHY ENVIRONMENTS - Towards an estimate of the environmental burden of disease ENVIRONMENTS - Towards PREVENTING DISEASE THROUGH HEALTHY WHO PREVENTING DISEASE THROUGH HEALTHY ENVIRONMENTS Towards an estimate of the environmental burden of disease A. Prüss-Üstün and C. Corvalán WHO Library Cataloguing-in-Publication Data Prüss-Üstün, Annette.