Applied Anatomy of the Wrist, Thumb and Hand
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2019 IWIW Meeting Abstracts, Las Vegas, Wed. Sept. 4Th SESSION 1
2019 IWIW Meeting Abstracts, Las Vegas, Wed. Sept. 4th SESSION 1: Carpal Ligament 1 Stable Central Column Theory of Carpal Mechanics Michael Sandow FRACS Wakefield Orthopaedic Clinic Adelaide, Australia Background: The carpus is a complicated and functionally challenged mechanical system and advancements in the understanding have been compromised by the recognition that there is no standard carpal mechanical system and no typical wrist. This paper cover component of a larger project that seeks to develop a kinetic model of wrist mechanics to allow reverse analysis of the specific biomechanical controls or rule of a specific patient's carpus, and then use those to create a forward mathematical model to reproduce the unique individual's anatomical motion based on the extracted rules. Objectives and Methods: Based on previous observations, the carpus essentially moves with only 2 degrees of freedom - pitch (flexion / extension) and yaw (radial deviation / ulnar deviation), while largely preventing roll (pronation / supination). The object of this paper is therefore to present the background and justification to support the rules based motion (RBM) concept states that the motion of a mechanical system, such as the wrist, is the net interplay of 4 rules - morphology, constraint, interaction and load. The Stable Central Column Theory (SCCT) of wrist mechanics applies the concept of RBM to the carpus, and by using a reverse engineering computational analysis model, identified a consistent pattern of isometric constraints, creating a "Two-Gear Four-Bar" linkage. This study assessed the motion of the carpus using a 3D dynamic visualization model, and the hypothesis was that the pattern and direction of motion of the proximal row, and the distal row with respect the immediately cephalad carpal bones or radius would be very similar in all directions of wrist motion. -

Defining the Morphometrics of the First Metacarpal for the Development of an Osseointegrated Prosthesis
Defining the Morphometrics of the First Metacarpal for the Development of an Osseointegrated Prosthesis Authors: JJ Vaux OMS-IV1, RR Hugate, M.D.2, JW Hills3, RF Grzybowski, D.O.4, CK Funk. Ph.D.1 Affiliations: 1Rocky Vista University College of Osteopathic Medicine, 2Colorado Limb Consultants, 3Dept of Materials and Mechanical Engineering, Denver University, 4Diversified Radiology Objective: Amputation of the thumb presents a serious insult to the hand and can result in up to a 22% loss of functionality in that limb (2,3). To date, several different techniques have been explored for reconstruction of the thumb, however none seem to be incredibly successful (1,4). We believe the answer lies in an osseointegrated prosthesis within the first metacarpal. In order to successfully create an osseointegrated prosthesis, the morphometrics of the first metacarpal are needed. The aim of this study was to define the geometry of the first metacarpal in order to help create a standardized set of stems and prostheses to treat patients who have suffered amputation of the thumb at the level of the first metacarpal phalangeal joint (MCPJ). Methods: A total of eighty first metacarpals from forty-one cadavers were studied. All soft tissues were removed and the first metacarpals were imaged by computed tomography (CT). Three-dimensional models were constructed using cuts from the coronal, sagittal, and axial planes. Using a HyperMesh software, the individual first metacarpals were analyzed and measurements were taken for overall length, radius of curvature, medullary canal diameter, cortical thickness, and distance from the distal end to the center of the isthmus. -

Fractures Long Bones, Upper Limb (Includes Hand)
Ministry of Defence Synopsis of Causation Fractures Long Bones, Upper Limb (includes hand) Author: Mr John A Dent, Ninewells Hospital and Medical School, Dundee Validator: Mr Sheo Tibrewal, Queen Elizabeth Hospital, London September 2008 Disclaimer This synopsis has been completed by medical practitioners. It is based on a literature search at the standard of a textbook of medicine and generalist review articles. It is not intended to be a meta-analysis of the literature on the condition specified. Every effort has been taken to ensure that the information contained in the synopsis is accurate and consistent with current knowledge and practice and to do this the synopsis has been subject to an external validation process by consultants in a relevant specialty nominated by the Royal Society of Medicine. The Ministry of Defence accepts full responsibility for the contents of this synopsis, and for any claims for loss, damage or injury arising from the use of this synopsis by the Ministry of Defence. 2 1. Definition 1.1. A bone breaks as a result of a variety of injuring forces. The fracture produced in a long bone may be of its shaft or diaphysis; towards one of its ends where the bone widens (metaphysis); or of the end of the bone, where it forms a joint with the next bone (Figure 1). Fractures near a joint may involve the joint surface causing intra-articular fractures. 1.2. It must always be remembered that the soft tissues surrounding the bone will also be damaged to a varying extent by the injuring force. -

Gross Anatomy
www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY www.BookOfLinks.com Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of the information contained in this work. Readers are encouraged to confirm the infor- mation contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY David A. Morton, PhD Associate Professor Anatomy Director Department of Neurobiology and Anatomy University of Utah School of Medicine Salt Lake City, Utah K. Bo Foreman, PhD, PT Assistant Professor Anatomy Director University of Utah College of Health Salt Lake City, Utah Kurt H. -
Anatomical Snuffbox
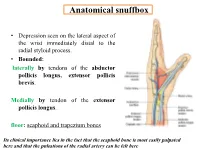
Anatomical snuffbox • Depression seen on the lateral aspect of the wrist immediately distal to the radial styloid process. • Bounded: laterally by tendons of the abductor pollicis longus, extensor pollicis brevis. Medially by tendon of the extensor pollicis longus. floor: scaphoid and trapezium bones Its clinical importance lies in the fact that the scaphoid bone is most easily palpated here and that the pulsations of the radial artery can be felt here Anatomical snuffbox Anatomical snuffbox • Contents: 2) Origin of the 1) The radial artery cephalic vein pass subcutaneously over the snuffbox. 3) Superficial branch of the radial nerve pass subcutaneously over the snuffbox. Blood supply of the hand Anastomoses occur between the radial and ulnar arteries via the superficial and deep palmar arches The Deep palmar arch is formed mainly by the radial artery while the superficial palmar arch is formed mainly by the ulnar artery 3-On entering the palm, it curves laterally behind (deep) the palmar 4-The arch is aponeurosis and in front completed on (superficial) of the long flexor the lateral side tendons forming by the the superficial palmar arch superficial branch of the radial artery. 2-Then it gives off its deep branch of which runs in front of the FR , and joins the radial artery to complete the deep palmar arch 1-Enters the hand anterior (superficial) to the Superficial flexor retinaculum palmar branch of radial artery through Guyon’s canal Radial artery 5-The superficial palmar arch gives off digital arteries from its convexity which pass to the fingers and supply them Superficial palmar arch Deep palmar branch of ulnar artery Superficial palmar branch of radial artery Ulnar artery Radial artery Radial Artery first dorsal interosseous muscle 1-From the floor of the anatomical snuff-box the radial artery leaves the dorsum of the hand by turning forward between the two heads of the first dorsal interosseous muscle. -

Carpal Tunnel Syndrome
Information O from Your Family Doctor Carpal Tunnel Syndrome What is carpal tunnel syndrome? hands a lot. You may notice that over time your Carpal tunnel syndrome (KAR-pal TUN-el grip gets weaker and you tend to drop heavy SIN-drome) is a common, painful disorder objects. of the wrist and hand. It happens when the median nerve, which runs through the wrist, How is it diagnosed? gets squeezed under a band of tissue called a Talk to your doctor if you are having these ligament. This causes pain and other symptoms symptoms. He or she will ask questions about along the nerve (see drawing). the ways you use your hands and about specific What causes it? Anything that increases Shading indicates area pressure on the median where symptoms are felt nerve can cause carpal tunnel syndrome. Sometimes pregnancy and health conditions like arthritis and diabetes can increase the pressure. People who use their hands and wrists repeatedly in the same way (for example, Transverse typists, carpenters, and carpal cashiers) are more likely to get ligament carpal tunnel syndrome. What are the symptoms? Carpal tunnel syndrome Thenar may cause pain, numbness, muscles Wrist or tingling in your wrist and bone hand, mostly in the middle finger, index finger, and Tendon thumb. The symptoms are Median usually worse at night and nerve when you use your wrists and ILLUSTRATION BY KATHRYN BORN continued O Page 1 of 2 Information O from Your Family Doctor Carpal Tunnel Syndrome (continued) symptoms in each part of your hand and wrist. He or she may also test how your nerves and Notes: muscles respond to electrical stimulation. -

New Fixation Approach for Transverse Metacarpal Neck Fracture: a Biomechanical Study
Chiu et al. Journal of Orthopaedic Surgery and Research (2018) 13:183 https://doi.org/10.1186/s13018-018-0890-2 RESEARCHARTICLE Open Access New fixation approach for transverse metacarpal neck fracture: a biomechanical study Yung-Cheng Chiu1,2, Ming-Tzu Tsai3, Cheng-En Hsu4,5, Horng-Chaung Hsu1,2, Heng-Li Huang6,7 and Jui-Ting Hsu6,7* Abstract Background: Fifth metacarpal neck fracture, also known as boxer’s fracture, is the most common metacarpal fracture. Percutaneous Kirschner-wire (K-wire) pinning has been shown to produce favorable clinical results. However, the fixation power of K-wires is a major concern. Plate fixation is also a surgical option, but it has the disadvantages of tendon adhesion, requirement of secondary surgery for removal of the implant, and postoperative joint stiffness. A fixation method that causes little soft tissue damage and provides high biomechanical stability is required for patients with fifth metacarpal neck fracture for whom surgical intervention is indicated. The present study proposed fixation using K-wires and a cerclage wire to treat fifth metacarpal neck fracture. The fixation power of this new method was compared with that of K-wires alone and plates. Methods: We used a saw blade to create transverse metacarpal neck fractures in 16 artificial metacarpal bone specimens, which were then treated with four types of fixation as follows: (1) locking plate with five locking bicortical screws (LP group), (2) regular plate with five bicortical screws (RP group), (3) two K-wires (K group), and (4) two K-wires and a figure-of-eight cerclage wire (KW group). -

CS-FFRA-05 – 2005-16 Super Duty Fabricated Radius Arms NOTE
Carli Suspension: 422 Jenks Circle, Corona, CA 92880 Tech Support: (714) 532-2798 CS-FFRA-05 – 2005-16 Super Duty Fabricated Radius Arms NOTE: Please review the product instructions prior to attempting installation to ensure installer is equipped with all tools and capabilities necessary to complete the product installation. We recommend thoroughly reading the instructions at least twice prior to attempting Installation. Before beginning disassembly of the vehicle, check the “What’s Included” section of the instructions to ensure you’ve received all parts necessary to complete installation. Further, verify that the parts received are PROPER TO YOUR application (year range, motor, etc.) to avoid potential down-time in correcting potential discrepancies. Any discrepancies will be handled by Carli Suspension and the correcting products will be shipped UPS Ground. LIFETIME PRODUCT WARRANTY Carli Suspension provides a limited lifetime product warranty against defects in workmanship and materials from date of purchase to the original purchaser for all products produced by Carli Suspension. Parts not manufactured by, but made to Carli Suspension’s specifications by third party manufacturers will carry a warranty through their respective manufacturer. (i.e. King Shocks, Bilstein Shocks, Fox Shocks). Deaver Leaf Spring’s warranty will be processed by Carli Suspension. Proof of purchase (from the original purchaser only) will be required to process any warranty claims. Carli Suspension products must be purchased for the listed Retail Price reflected by the price listed on the Carli Suspension Website at the time of purchase. Carli Suspension reserves the right to refuse warranty claims made by any customer refusing or unable to present proof of purchase, or presenting proof of purchase reflecting a price lower than Carli Suspension’s Retail Price at the time the item was purchased. -
What Is a Scaphoid Fracture?
Sussex Hand CONDITION Surgery Scaphoid Fractures CONDITION The scaphoid is one of the small What is a bones that make up your wrist. It is the commonest wrist bone Scaphoid Fracture? to break. Normal Wrist Xray Sometimes the diagnosis is delayed, Sometimes an operation is often by months or years. In this recommended. The exact situation xrays, MRI and CT scans approach will depend on the type might all be required to make a full of injury. Commonly a screw is Rest of the Thumb assessment of what is needed. placed down the centre of the metacarpal wrist bones scaphoid to keep the fragments (8 small bones lined up and still whilst the bone in total) The scaphoid What treatment is heals. This can sometimes be bone needed for a scaphoid done in a minimally invasive way fracture? with very small incisions (see Distal ulna This depends on a great many ‘Percutaneous screw fixation of Distal radius things. Some important factors are: Scaphoid Fractures’). Later on 1. How old is the injury? Fresh bigger operations might be A fracture of the scaphoid fractures have better healing necessary to re-align a bent potential scaphoid and put new bone into 2. Which part of the scaphoid is the old fracture (see ‘ORIF of broken? The nearer the fracture is Scaphoid Fractures +/-bone to end of the scaphoid next to the grafting’). radius (proximal pole) the more Very obvious chance there is of problems with What is the outcome fracture in the healing. This is to do with the blood following a scaphoid middle (waist) supply to the scaphoid bone which fracture? of the scaphoid is not good in the proximal pole. -

Table 9-10 Ligaments of the Wrist and Their Function
Function and Movement of the Hand 283 Table 9-10 Ligaments of the Wrist and Their Function Extrinsic Ligaments Function Palmar radiocarpal Volarly stabilizes radius to carpal bones; limits excessive wrist extension Dorsal radiocarpal Dorsally stabilizes radius to carpal bones; limits excessive wrist flexion Ulnar collateral Provides lateral stability of ulnar side of wrist between ulna and carpals Radial collateral Provides lateral stability of radial side of wrist between radius and carpals Ulnocarpal complex and articular Stabilizes and helps glide the ulnar side of wrist; stabilizes distal disk (or triangular fibrocartilage radioulnar joint complex) Intrinsic Ligaments Palmar midcarpal Forms and stabilizes the proximal and distal rows of carpal bones Dorsal midcarpal Forms and stabilizes the proximal and distal rows of carpal bones Interosseous Intervenes between each carpal bone contained within its proximal or distal row Accessory Ligament Transverse carpal Stabilizes carpal arch and contents of the carpal tunnel Adapted from Hertling, D., & Kessler, R. (2006). Management of common musculoskeletal disorders: Physical therapy principles and methods. Philadelphia, PA: Lippincott, Williams & Wilkins.; Oatis, C. A. (2004). Kinesiology: The mechanics and pathomechanics of human movement. Philadelphia, PA: Lippincott, Williams & Wilkins.; Weiss, S., & Falkenstein, N. (2005). Hand rehabilitation: A quick reference guide and review. St. Louis, MO: Mosby Elsevier. The radial and ulnar collateral ligaments provide lateral and medial support, respectively, to the wrist joint. The ulnocarpal complex is more likely to be referred to as the triangular fibro- cartilage complex (TFCC) and includes the articular disk of the wrist. The TFCC is the major stabilizer of the distal radioulnar joint (DRUJ) and can tear after direct compressive force such as a fall on an outstretched hand. -

Isolated Trapezoid Fractures a Case Report with Compilation of the Literature
Bulletin of the NYU Hospital for Joint Diseases 2008;66(1):57-60 57 Isolated Trapezoid Fractures A Case Report with Compilation of the Literature Konrad I. Gruson, M.D., Kevin M. Kaplan, M.D., and Nader Paksima, D.O., M.P.H. Abstract as an axial load5,6 or bending stress7 transmitted indirectly Isolated fractures of the trapezoid bone have been rarely to the trapezoid through the second metacarpal. We present reported in the literature, the mechanism of injury being a case of an acute, isolated trapezoid fracture that resulted an axial or bending load transmitted through the second from direct trauma to the distal carpus and that was treated metacarpal. We report a case of an isolated, nondisplaced nonoperatively. Additionally, strategies for diagnosis and trapezoid fracture that was sustained by direct trauma treatment, as well as a synthesis of the published results and subsequently treated successfully in a short-arm cast. for both isolated and concomitant trapezoid fractures, are Diagnostic and treatment strategies for isolated fractures presented. of the trapezoid bone are reviewed as well as the results of operative and nonoperative treatment. Case Report A 25-year-old right-hand dominant male presented to the ractures of the carpus most commonly involve the emergency room (ER) complaining of isolated right-wrist scaphoid,1 with typical physical examination findings pain and swelling of 1 day’s duration. The patient stated Fof “snuffbox” tenderness. This presentation is fre- that a heavy metal door at work had closed onto the back quently the result of the patient falling onto an outstretched of his wrist causing an immediate onset of swelling and hand. -

Upper Limb Fractures in Rugby in Huddersfield 1986- 1 990
Br J Sp Med 1991; 25(3) From the Clinic Br J Sports Med: first published as 10.1136/bjsm.25.3.139 on 1 September 1991. Downloaded from Upper limb fractures in rugby in Huddersfield 1986- 1 990 K.S. Eyres FRCS', A. Abdel-Salam FRCS2 and J. Cleary FRCS3 Research Registrar, Department of Human Metabolism and Clinical Biochemistry, University of Sheffield, Sheffield, UK 2 Orthopaedic Registrar, Huddersfield Royal Infirmary, Huddersfield, UK 3 Orthopaedic Consultant, Huddersfield Royal Infirmary, Huddersfield, UK Most injuries sustained by rugby players affect the soft Case 1 tissues, and fracture is relatively uncommon. Whereas the lower limb is most affected in footballers, the upper limb A 24-year-old full-back fractured his left clavicle in a tends to be injured in rugby players. Thirty consecutive scrummage in 1988 (Figure 1). Six months later, he fractures and ten dislocations affecting the upper limb, sustained a direct blow to the left shoulder. Radio- sustained by 35 rugby players, are reported. graphs showed a fracture to the greater tuberosity of the left humerus (Figure 2). He was treated with a Keywords: Rugby injury, hamate fracture, sports injury collar and cuff and was able to return to matchplay after 2 months. Nine months later he fell onto his left hand after a tackle. Radiographs showed a sagittal Most injuries sustained in rugby matches are to the fracture of the body of the hamate and a fracture of soft tissues. Fractures are relatively uncommon, the base of the fourth metacarpal (Figure 3). He was estimated to account for only 4% of injuries in adult treated conservatively with plaster immobilization, matches and for 5% of injuries in school matches'.