Gender Identity Development
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Practical Tips for Working with Transgender Survivors of Sexual Violence
Practical Tips: working with trans survivors michael munson Practical Tips for Working With Transgender Survivors of Sexual Violence Who Are Transgender People? Transgender is an umbrella term which encompasses the whole “gender community,” including transsexuals, cross‐dressers, intersexed individuals, androgynes, bigendered persons, genderqueers, SOFFAs (Significant Others, Friends, Family and Allies) and others. Transgender may also refer to people who do not fit neatly into either the “male” or “female” categories, instead crossing or blurring gender lines. The term can also refer to butch lesbians and effeminate gay men. In some communities, “transgender” refers only to cross‐dressers. By definition, transgender individuals piece together a self‐identity that is different from or in opposition to what everyone tells them they are. Although the rise of the Internet and growing public visibility of transgender people and issues are making it easier for individuals to tap into preexisting identity models, the transgender experience is still largely an isolated, individual one. This might be the primary reason why the nomenclature for the trans experience is both unsettled and, among trans people themselves, very hotly contested. There are literally hundreds of words used to describe a trans identity or experience (See last page). Therefore, definitions and examples should be used gingerly and in a way that makes it possible for each trans individual hirself to use the term(s) s/hei considers most reflective of hir self‐conception and experience. Key Concepts Our culture strongly promotes the idea of an immutable gender binary in which people are supposed to fit into only one of just two gender boxes, and stay there from birth to death. -

Black Boi, Boss Bitch
Black Boi, Boss Bitch Lauryn Hill 18 Jan 1995 - 26 Sep 1998 BLACK QUEER LOOKS Y todo comenzo bailando.... 27 Oct 1998 “Y todo comenzo bailando”...The earliest memories I can recall of my existence are festive. 20 Pound Pots of pernil & pigfeet. Pasteles, Gandulez, Guinea, Pollo Guisado. Habichuelas. 5 different types of beans & 5 different dishes on one plate. Even if only 4 niggas pulled up to the crib, abuela was always cooking for 40. The image of her red lipstick stain on hefty glasses of Budweiser that once contained Goya olives is forever etched in my mind. This was that poor boricua family that stored rice & beans in “I Can’t Believe it’s Not Butter” containers.The kind of family that blasted Jerry Rivera’s & Frankie Ruiz voices over dollar-store speakers. The kind that prized Marc Anthony, Hector LaVoe, El Gran Combo, La India, Tito Rojas. Victor Manuelle. Salsa Legends that put abuela's feet to work. My cousin Nina & her wife Iris who sparked their Ls in the bathroom, waving around floor length box braids, and bomb ass butch-queen aesthetics. “Pero nino, you hoppin on the cyph?. Uncle Negro or “Black”as we called him for his rich dark-skin, stay trying to wife my mom’s friends. 7:11 pm. 7 pounds 8 oz. October 27th. Maybe it was the lucky 7. Maybe it was fated for them to welcome another, intensely-loving Scorpio into their home. Or maybe it was just another blissful evening in the barrio. Where Bottles of Henny would be popped, and cousins & aunts & uncles you didn’t even know you had would reappear. -

The Oxford Democrat : Vol. 70. No.52
The Oxford Democrat. 1903. NUMBER 52. VOLUME 70. SOUTH PARIS, MAINE, TUESDAY, DECEMBER 29, KH tiMh'.l lo; ili l 'y. oners, but Beverley soon suspected tl tt rutiler item, who was coining out 01 never fails. But he'll tell Clark to eta.v JUNKS, Fruit Marketing and Storage. *«W>4^3*4HfcHêHîMlHWHfr^ Furii «worth was on his guard in a C. THE a "tralllc In hah," ae the terrible bu-tl- u cabin nut far away, beard and knew where he is, and Vigo can do no more." ^ AMONG FARMERS. Some of the most and twin!;iing. lie set his jaw and uttered preening impor- ness had been named, was going on. the voice. What effect Helm's hold and appar- & Machinist, in- a< I!· htnh.· Smith tant relating to the fri\it f nil ugly oath: then qiii-k MA1NK. questions miH"î Savages came In from far away with Ho. lio. little cried artless talk h:id upon Hamilton's SOUTH PARIS, are those that out of the y4"i«P my lady!" ently at the with "SFLKD THIS PLOW." dustry grow he struck siucwlse pistol of general machinery, steam en in horticulture to scalps yet scarcely dry dangling at Adrien ne's captor in a breezy, jocund mind Is not recorded, hut the meager Manufacturer anil tools., .present tendency pro- his blade. It was a move which might mill work, spool machinery their belis. It made the Vir- "You wouldn't run over u facts at command show that ,'lties, drille made and duce each fruit in that section where it #| young tone. -

Sexual Orientation and Trans Sexuality 101
Sexual Orientation and Trans Sexuality 101 Michael L Krychman MD Executive Director of the Southern California Center for Sexual Health and Survivorship Medicine Associate Clinical Professor UCI AASECT Certified Sexual Counselor Developmental Sexuality Review • Things do go wrong! – Chromosomal – Hormonal Gender Identity & Sexual Orientation are Different! • Every individual has a – biological sex – a gender identity – a sexual orientation. – (All can be considered fluid!) • Being transgender does not mean you’re gay and being gay does not mean you’re transgender. – There is overlap, in part because gender variance is often seen in gay context. – Masculine females and feminine males are often assumed to be gay; – “Anti-gay” discrimination and violence often targets gender expression, not sexuality Anatomy does not determine sexual orientation Homophobia is different than Transphobia Case: Ego Dystonic Bisexual Transgender Male becoming a female Has both a male and female partner Parts: heterosexual Identity: homosexual Gender Identity & Sexual Orientation are Different! • Coming out as gay is different than coming out as transexual • Trans people are often marginalized in G/L context. • How do we apply cultural competency lessons that apply around heterosexism to gender variance? • CDC categorizes MTFs and partners as MSM; • neither partner self-identifies as MSM • Power relationship between HCP and client is intensified; provider as gate-keeper who must give ongoing “approval” Development of Sexual Orientation and Gender Identity Etiological -
Lgbt Resource Roundup
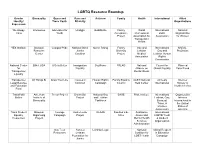
LGBTQ Resource Roundup Gender Bisexuality Queer and Race and Activism Family Health International Allied Identity/ Trans Youth Ethnicity Organizations Expression We Happy Interweave Advocates for Unid@s GetEQUAL Family World International National Trans Youth Acceptance Professional LGBT Organization Project Association for Association for Women Transgender Health YES Institute Bisexual Campus Pride National Black Queer Rising Family Gay and International NARAL- Resource Justice Diversity Lesbian Gay and ProChoice Center Coalition Project Medical Lesbian Human Association Rights Commission National Center BiNet USA It Gets Better Immigration SoulForce PFLAG National Council for Planned for Equality Alliance on Global Equality Parenthood Transgender Mental Illness Equality Transgender All Things Bi Draw Your Line Causes in Human Rights Family Equality GLBT National Amnesty Intersex Legal Defense Common Campaign Council Help Center International Society of and Education North America Fund TransFaith American Trevor Project Brown Boi National Gay SAGE Pride Institute International Organization Online Institute of Project and Lesbian Lesbian, Gay, Intersex Bisexuality Taskforce Bisexual, International in Trans, & the United Intersex States of Association America Trans Student Bisexual Courage Audre Lorde GLAAD Families Like Substance International Equality Organizing Campaign Project Mine Abuse and LGBTQ Youth Resources Project Mental Health & Student Services Organization Administration Gay Teen Astraea Lambda Legal National Global Respect -

Outline Introduction, Background, and Terminology
SUMMARY OF CLINICAL EVIDENCE FOR GENDER REASSIGNMENT SURGERIES Outline Introduction, Background, and Terminology ................................................................................................ 2 Categories of Gender Reassignment Surgery ........................................................................................... 3 Summaries of Clinical Evidence for Gender Reassignment Surgeries ......................................................... 4 Surgeries for Female-to-Male (FTM) individuals..................................................................................... 4 Breast/Chest Surgery ........................................................................................................................ 4 Genital Surgeries ............................................................................................................................... 4 Other Surgeries ................................................................................................................................. 4 Surgeries for Male-to-Female (MTF) individuals..................................................................................... 5 Breast/Chest Surgery ........................................................................................................................ 5 Genital Surgeries ............................................................................................................................... 5 Other Surgeries ................................................................................................................................ -

Caring for Transgender People with Severe Mental Illness
Caring for Transgender People with Severe Mental Illness MAY 2018 Transgender people, like the general population, can suffer from a variety of common and rare severe mental health illnesses (SMI). Severe mental illness (SMI) refers to psychiatric disorders that are relatively persistent and result in comparatively severe impairment in major areas of function, disruption of normal developmental processes, and reduced vocational capacity and social relationships.1 People with SMI experience unique vulner- abilities within society, which include a longstanding history of being institu- tionalized, marginalized, victimized, and subjected to experimental psychiatric interventions.2 There is strong evidence that people with SMI are woefully underserved and rarely receive evidence-based treatments even when they are able to access care.2 In turn, transgender people are more likely than the general population to expe- rience discrimination in housing, employment, and healthcare.3 Many are verbal- ly and physically victimized starting at a young age.3 Abuse related to gender minority status has a dose-response relationship with major depressive disorder and suicidality among transgender adolescents.4 Daily experiences of anti-trans- gender stigma, prejudice, and discrimination become internalized and ultimately affect psychological health.5,6 An estimated 40% of all transgender people have attempted suicide in their lifetimes.3 Though research on transgender behavioral health is limited, studies have found a higher risk for mood disorders, posttrau- matic stress disorder (PTSD), and substance use disorders, but not psychotic disorders compared to the rest of the population.7,8 When risk profiles based on transgender status and SMI intersect, patients are liable to experience a particu- larly dangerous array of vulnerabilities that require attentive, specialized care. -

Trans People, Transitioning, Mental Health, Life and Job Satisfaction
DISCUSSION PAPER SERIES IZA DP No. 12695 Trans People, Transitioning, Mental Health, Life and Job Satisfaction Nick Drydakis OCTOBER 2019 DISCUSSION PAPER SERIES IZA DP No. 12695 Trans People, Transitioning, Mental Health, Life and Job Satisfaction Nick Drydakis Anglia Ruskin University, University of Cambridge and IZA OCTOBER 2019 Any opinions expressed in this paper are those of the author(s) and not those of IZA. Research published in this series may include views on policy, but IZA takes no institutional policy positions. The IZA research network is committed to the IZA Guiding Principles of Research Integrity. The IZA Institute of Labor Economics is an independent economic research institute that conducts research in labor economics and offers evidence-based policy advice on labor market issues. Supported by the Deutsche Post Foundation, IZA runs the world’s largest network of economists, whose research aims to provide answers to the global labor market challenges of our time. Our key objective is to build bridges between academic research, policymakers and society. IZA Discussion Papers often represent preliminary work and are circulated to encourage discussion. Citation of such a paper should account for its provisional character. A revised version may be available directly from the author. ISSN: 2365-9793 IZA – Institute of Labor Economics Schaumburg-Lippe-Straße 5–9 Phone: +49-228-3894-0 53113 Bonn, Germany Email: [email protected] www.iza.org IZA DP No. 12695 OCTOBER 2019 ABSTRACT Trans People, Transitioning, Mental Health, Life and Job Satisfaction For trans people (i.e. people whose gender is not the same as the sex they were assigned at birth) evidence suggests that transitioning (i.e. -

Trransition-Related Health Care
31 CHAPTER VIII Trransition-Related Health Care The kinds of health care associated with gender transition needs associated with transition than for treating someone have too often been misunderstood as cosmetic, experimental with diabetes who needs vital care. In both cases, a doctor or simply unnecessary. Yet there is medical consensus that makes an individualized assessment to determine if treatment is hormone therapy and gender-affirming surgery are medically warranted—if it is, both patients should get the recommended necessary for many transgender people. It’s quite clear now that care. a person’s gender identity—one’s inner sense of being male or This fact sheet explains the medical community’s current female—is deep-seated and cannot be changed. Therefore, this framework for understanding transition-related care as transition-related health care can be crucial. medically necessary and how Lambda Legal and other The courts have come a long way on this issue in recent advocates are applying this in the legal domain to challenge years, citing decades of medical data to find in more and more denial of such care as discrimination. Also highlighted are ways cases that not providing transition-related health care as readily that private industry and municipal government have begun to as other medically necessary treatment is discrimination. follow the medical mainstream by dropping barriers to health The problem is that most public and private insurance care for transgender people and setting standards for a more companies are still behind the times. Many cite cost, even equitable future. though that hasn’t turned out to be an issue at all for the growing number of employers now providing coverage. -

A Little Shiny Gender Breakthrough": Community Understandings of Gender Euphoria
”A little shiny gender breakthrough": Community understandings of gender euphoria Presenter: Will Beischel (Brit Ellis, pinterest.com) Co-authors: Stephanie Gauvin and Dr. Sari van Anders : @WillBeischel : [email protected] 15 minute talk, questions at end of session I’m coming to you from Chicago, which is located on the traditional unceded homelands of the Council of the Three Fires: the Ojibwe, Odawa, and Potawatomi Nations. I’m a PhD student in psychology and I’ll be presenting some empirical qualitative work today on gender euphoria that I've done with Stephanie Gauvin and Sari van Anders What is Gender Dysphoria? ● The distress arising from conflicts between a person’s gender identity or expression and their assigned gender/sex (American Psychiatric Association, 2016) ● Physical body (Pulice-Farrow, Cusack, Galupo, 2019) ● Social gendered experiences (Galupo, Pulice-Farrow, Lindley, 2019) ● Often seen as a diagnostic term 2 I’ll start with a term that is probably familiar to many if not all of you, gender dysphoria, which is the distress arising from conflicts between a person’s gender identity or expression and their assigned gender/sex. Just a note that I use gender/sex as an umbrella term to indicate the entanglement of people’s social genders with their physical, bodily sexes, though not everyone experiences it this way. Research has demonstrated that gender dysphoria can be about sex or the physical body, as with feelings of discord between a person’s sex characteristics and their gender/sex identity, and it can also arise from social gendered experiences, such as people using the wrong pronouns or name for someone. -

Trans Mental Health and Social Work Resources, Harry Dixon, M.A., Katrina Hale, MSW, & Kelly Serafini, Ph.D
Trans Mental Health and Social Work Resources, Harry Dixon, M.A., Katrina Hale, MSW, & Kelly Serafini, Ph.D. 1 Agenda • Gender Dysphoria Criteria • Prevalence of Mental Health Disorders • Safety (Suicide/Homicide) • Treatment Outcomes & Mental Health • Psychotherapeutic Considerations • Patient Resources 2 BACKGROUND Kelly Serafini, Ph.D. 3 Being Transgender is Not a Mental Disorder • Although Gender Dysphoria is a mental illness, being transgender itself is not a disorder and it is not pathological • The dysphoria that is caused by the incongruence between physical anatomy and gender identity is distressing and it is treatable 4 Gender Dysphoria Disorder (Adults & Adolescents) • Difference between one’s experienced/expressed gender and assigned gender, and significant distress or problems functioning • Lasts at least 6 months • And 2 of the following criteria are met: A marked incongruence between one’s experienced/expressed gender and primary and/or secondary sex characteristics A strong desire to be rid of one’s primary and/or secondary sex characteristics A strong desire for the primary and/or secondary sex characteristics of the other gender A strong desire to be of the other gender A strong desire to be treated as the other gender A strong conviction that one has the typical feelings and reactions of the other gender 5 Gender Dysphoria Disorder (Children) • Lasts at least 6 months • And 6 of the following criteria are met: A strong desire to be of the other gender or an insistence that one is the other gender A strong preference -

A Primary Care Toolkit Contents
August 2021 Gender-affirming Care for Trans, Two-Spirit, and Gender Diverse Patients in BC: A Primary Care Toolkit Contents Table of Contents ................................................................................................................................................................... w Indigenous people and Two-Spirit considerations ....................................................................................................... iii Acknowledgment and Disclaimer ...................................................................................................................................... iv Introduction ................................................................................................................................................................................1 Gender-affirming health care options ............................................................................................................................... 2 Social options ..................................................................................................................................................................... 2 Medical options ................................................................................................................................................................. 2 Surgical options ................................................................................................................................................................. 2 Role of the primary care provider