Right Atrium: Sinus Venarum
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
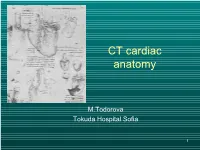
CT Cardiac Anatomy
CT cardiac anatomy M.Todorova Tokuda Hospital Sofia 1 MDCT vs US 2 Position of the heart • Position in the thoracic cavity • Cardiac apex • Cardiac base 3 Systematic approach Cardiac CT • Right atrium • Aorta • Right ventricle • Coronaries • PA • Cardiac Veins • PV • Valves • Left atrium • Pericardium • Left ventricle 4 Right atrium 5 Right atrium • RA appendage – Pectinate muscles >2mm – 20 sc.cm normal size on 4 ch.view • Crista terminalis • Sulcus terminalis • Coronary sinus • Thebesian valve • Eustachian valve • Internal septum • Fossa ovalis 6 Tricuspid valve • Tricuspid valve- separates RA from RV • Trileflet valve- anterior,posterior, septal • Structure- leflet,annulus,commi ssures 7 Right ventricle 8 RV-anatomy inflow tract 4 chamber view outflow tract 9 Volumetric parameters of RV • Normal quantitative RV Values • EF = 61+/-6 • End diastolic volume = 173+/-39 • End systolic volume = 69+/-22 • Strike volume = 104+/=21 • Mass = 35-45 10 RV-anatomic structure • Tricuspid valve • RV wall • Pulmonary valve • Intrventricular septum • Anterior longitudinal sulcus • Posterior longitudinal sulcus • Moderator band 11 • Interventricular septum – Separates ventricles – Thin wall – Convexity toward the right ventricle – Muscular ventricular septum – Membrannous ventricular septum • Anterior and posterior longitudinal sulcus – Ventricles separeted externally by grooves – Anterior longitudinal sulcus – Posterior longitudinal sulcus – Moderator band 12 Pulmonary valve • Three leaflet • Semilunar morphology 13 PA anatomy 14 Left atrium and pulmonary veins 15 • Pulmonry veins – Two inferior and two superior into either side of LA 16 LA - anatomy • LA • LA appendage – Arises from the superiorlateral aspect of the LA – Projects anteriorly over the proximal LCX artery – Pectinate muscles >1mm 17 Mitral valve • represent inflow tract of LV • bicuspid • fibrous ring mitral valve-annulus • triangular leaflets 18 Left ventricle 19 LV - anatomy • Inflow tract • Outflow tract • Chordae tendinae • Papillary muscles 20 LV wall Normal Anterior MI LV papillary muscles Ferencik et al. -

THE HEART Study Objectives
THE HEART Study Objectives: You are responsible to understand the basic structure of the four chambered heart, the position and structure of the valves, and the path of blood flow through the heart. Structure--The Outer Layer pericardium: a specialized name for the celomic sac that surrounds the heart. fibrous pericardium: the most outer, fibrous layer of the pericardium. serous pericardium: there are two surfaces (layers) to this tissue a) parietal layer: the outer layer of the serosa surrounding the heart. Lines the fibrous pericardium, and the combination of the two layers is also called the parietal pericardium. b) visceral layer: the inner layer of the serosa surrounding and adhering to the heart. Also called the visceral pericardium or epicardium. pericardial cavity: the potential space between the parietal and visceral layers of the serous pericardium. The cavity is filled with serous fluid Structure--The Heart: Blood is delivered to the right atrium from the coronary sinus, inferior vena cava and superior vena cava Blood travels to the right ventricle from the right atrium via the right atrioventricular valve Blood travels from the left atrium to the left ventricle via the left atrioventricular valve Blood leaves the heart via the pulmonary valve to the pulmonary trunk, is delivered to the lungs for oxygenation and returns via the pulmonary veins to the left atrium a) crista terminalis: separates the anterior rough-walled and posterior smooth-walled portions of the right atrium. b) right auricle: small, conical, muscular, pouch-like appendage. c) musculi pectinate (pectinate muscles): internal muscular ridges that fan out anteriorly from the crista terminalis. -

Chapter 20: Cardiovascular System: the Heart
Activity Chapter 19 1) Which of the following terms identifies the anatomical region found between the lungs that extends from the sternum to the vertebral column and from the first rib to the diaphragm? a) Epicardium d) Mediastinum b) Abdominal cavity e) Thoracic cavity c) Pericardium 2) The membrane that surrounds and protects the heart is called the a) pericardium. d) mediastinum. b) pleura. e) endocardium. c) myocardium. 3) The apex of the heart is normally pointed a) at the midline. d) is different for males and females b) to the left of the midline. e) posteriorly. c) to the right of the midline. 4) Which of the following is used to reduce friction between the layers of membranes surrounding the heart? a) Synovial fluid d) Pericardial fluid b) Endocardium e) Capillary endothelium c) Pleural fluid 5) Identify the pouch-like structure that increases the total filling capacity of the atrium. a) Ventricle d) Interatrial septum b) Coronary sulcus e) Auricle. c) Fossa ovalis 6) Identify the groove found on the surface of the heart and marks the boundary between the right and left ventricles. a) Coronary sulcus d) Coronary sinus b) Anterior interventricular sulcus e) Anterior intraventricular sulcus c) Posterior interventricular sulcus 7) Identify the muscular ridges that are found on the anterior wall of the right atrium and extend into the auricles. a) Pectinate muscles d) Papillary muscles b) Trabeculae carneae e) Chordae tendinae c) Coronary sulci 8) Through which structure does blood pass from the right atrium to the right ventricle? a) Bicuspid valve d) Mitral valve b) Interventricular septum e) Ascending aorta c) Tricuspid valve 9) Contraction of the ventricles of the heart leads to blood moving directly a) into arteries. -

Light and Scanning Electron Microscopic Examination of the Saanen Goat Heart
Turkish Journal of Veterinary and Animal Sciences Turk J Vet Anim Sci (2020) 44: 1172-1180 http://journals.tubitak.gov.tr/veterinary/ © TÜBİTAK Research Article doi:10.3906/vet-2005-137 Light and scanning electron microscopic examination of the Saanen goat heart 1, 2 1 Sedef SELVİLER SİZER *, Yonca Betil KABAK , Murat KABAK 1 Department of Anatomy, Faculty of Veterinary Medicine, Ondokuz Mayıs University, Samsun, Turkey 2 Department of Pathology, Faculty of Veterinary Medicine, Ondokuz Mayıs University, Samsun, Turkey Received: 29.05.2020 Accepted/Published Online: 27.09.2020 Final Version: 18.12.2020 Abstract: It is important to know the morphological structure of the heart, which is a vital organ of the body, in detail. For this reason, we aimed to examine the morphological structure of the Saanen goat heart using light and scanning electron microscopy (SEM). A total of thirteen Saanen goat hearts were used in the study. To demonstrate the histological structure of the heart, samples taken from 9 hearts were fixed in 10% formaldehyde solution and blocked in paraffin after routine histological procedures. Histological staining was performed on the sections taken from the blocks. Four hearts were fixed in a 2.5% glutaraldehyde solution for electron microscopic examination. The samples taken were dehydrated with different concentrations of acetone, treated with osmium tetroxide, and critical point dried in accordance with SEM procedures. After being coated with gold/palladium (Au/Pd), samples were made ready for imaging under SEM. The general structure of the heart was determined in detail with histological and SEM examination. Although the structural findings of the Saanen goat heart were generally similar to findings in the literature, the shapes of the cells that formed the Purkinje fiber networks in SEM examination were different from other species. -

The Circulatory System Provides a Way for the Blood to Be Transported Throughout the Body
INTRODUCTORY REMARKS: •The circulatory system provides a way for the blood to be transported throughout the body. This provides nutrients to the cells and allows wastes to be removed. •Open vs. Closed Circulatory System Review the essential roles of the following blood vessels: Arteries - Arterioles – Veins - Venules - Capillaries - THE HEART The Heart services 2 circuits •A heart is a hollow muscular pump. Systemic circuit (whole body other than lungs) [bring oxygenated blood to the rest of the body] •Hearts consist of two chamber types separated by valves and or septa. Pulmonary circuit (lungs) [re-oxygenates blood] 1. Atrium - This type of chamber receives *heart beats ≈100,000 times/day (≈8000 liters of blood into the heart. blood) 2. Ventricle - This type of chamber is the pumping chamber. 1 Main Heart Anatomy •Right heart is concerned with pulmonary circulation •Left heart is concerned with systemic circulation RA- Vena Cavae RV- Pulmonary Artery LA- Pulmonary Veins LV-Aorta •The heart is located in the anterior chest, directly posterior to the sternum (peri / around; cardium / refers to the heart) 1. Pericardium •Serous membrane sac around the heart •Formed like a balloon around a fist. Fist= heart Balloon= pericardial sac •Visceral pericardium covers the outer surface of the heart •Parietal pericardium lines the inner surface of the pericardial cavity •The pericardial space is filled with pericardial fluid (≈10-20 ml) acts as a lubricant during heart beats 2 2. Myocardium - The heart muscle tissue itself. The inner myocardial surface is lined with an endothelial sheet of tissue called the endocardium. Cardiac muscle cells act as a single unit called a functional syncytium. -
Lab 3 Heart Sounds, Valve Problems and Blood Flow
Lab 3 Heart Sounds, Valve Problems and Blood Flow MDufilho 1 Heart Sound Lub-dup, lub-dup, lub-dup • Lub – lower pitch • Dup – higher pitch • Normal heart sounds -Animated Normal S1 S2 MDufilho 2 Figure 18.20 Areas of the thoracic surface where the sounds of individual valves can best be detected. Aortic valve sounds heard in 2nd intercostal space at right sternal margin Pulmonary valve sounds heard in 2nd intercostal space at left sternal margin Mitral valve sounds heard over heart apex (in 5th intercostal space) in line with middle of clavicle Tricuspid valve sounds typically heard in right sternal margin of 5th MDufilho intercostal space 3 Figure 18.5e – Heart Valves Aorta Left pulmonary artery Superior vena cava Right pulmonary artery Left atrium Left pulmonary veins Pulmonary trunk Right atrium Mitral (bicuspid) valve Right pulmonary veins Fossa ovalis Aortic valve Pectinate muscles Pulmonary valve Tricuspid valve Right ventricle Left ventricle Chordae tendineae Papillary muscle Interventricular septum Trabeculae carneae Epicardium Inferior vena cava Myocardium Endocardium Frontal section MDufilho 4 (not in text) Valve Prolapse MDufilho 5 (not in text) Valve Prolapse MDufilho 6 (not in text) Valvular Stenosis MDufilho 7 (not in text) Valvular Stenosis Heart Sounds S3 S4 Murmurs MDufilho 8 Figure 18.5b Blood Supply to the Myocardium Left common carotid artery Brachiocephalic trunk Left subclavian artery Superior vena cava Aortic arch Ligamentum arteriosum Right pulmonary artery Left pulmonary artery Ascending aorta Left pulmonary -

Morphological and Biometric Characteristics of the Pectinate Muscles and the Taenia Sagittalis of the Right Atrium in the Human Heart
ORIGINAL ARTICLE Eur. J. Anat. 23 (5): 355-359(2019) Morphological and biometric characteristics of the pectinate muscles and the taenia sagittalis of the right atrium in the human heart Ana Barriga1, Jorge Henriquez2, Enrique Olave2 1Institute of Anatomy, Histology and Pathology, Universidad Austral de Chile, Chile, 2Faculty of Medicine, Universidad de La Frontera, Chile SUMMARY in 46.6% of the hearts examined, two or more TS in 29.8% and no TS in 23.6%. The length of the The crista terminalis (CT) is a well-defined fibro- pectinate muscles is variable; the shortest are lo- muscular crest formed by the union of the venous cated on the medial wall. Six types of pectinate sinus and the primitive right auricle, which extends muscle patterns were observed. along the posterolateral face of the right atrial wall. The pectinate muscles (PM) are muscular crests Key words: Pectinate muscles – Right atrium – which extend anterolaterally from the CT to the Human heart – Biometry auricle and may present in a series of variable shapes and sizes. The biggest and most promi- INTRODUCTION nent PM is called the taenia sagittalis (TS). PM with highly trabeculated muscle fibres predispose The crista terminalis (CT) is a well-defined fibro- patients to the occurrence of arrhythmias. The pre- muscular crest formed by the union of the venous sent article is a descriptive study of the anatomical sinus and the primitive right atrium, which extends and biometric characteristics of the right atrium. along the posterolateral face of the right atrial wall We studied 30 hearts of adult Chilean individuals, (Salustri et al., 2010). -

Overview of Cardiac Anatomy Relevant to Catheter Ablation
CAOC01 9/18/07 2:35 PM Page 1 I Fundamentals CAOC01 9/18/07 2:35 PM Page 3 Overview of cardiac anatomy relevant to 1 catheter ablation Siew Yen Ho Every new diagnostic technique and every new surgical for appropriate clinical correlations. He termed the orienta- or interventional procedure in the heart leads to a review tion of the heart, seen in its living condition, as “attitudinal.” of the organ’s anatomy relevant to that particular tech- Since electrophysiologists “view” the patient with the nique or procedure. Although the anatomy of the heart heart in situ, it is essential that the attitudinal approach [3] has remained unchanged, the perspectives from which should be adopted when describing the spatial relation- clinicians can approach the heart have evolved through ships of chambers and structures. The names of the cham- the ages. Catheter ablation for cardiac arrhythmias is the bers remain unaltered, although right heart chambers are relatively “new boy on the block” that has led to a new not strictly to the right nor left heart chambers strictly to perception of cardiac anatomy in the normally structured the left. as well as the congenitally malformed heart. In this chap- The heart lies in the mediastinum of the thoracic cavity, ter, I hope to provide an overview of the fundamentals in between the left and right lungs. When viewed from the anatomy of the normally structured heart, with emphasis front, the heart has a trapezoidal silhouette. Two-thirds of on features relevant to catheter ablation. Necessarily, much its bulk lies to the left of the midline of the chest, with its of the information is basic, although crucial to knowing apex directed to the left and inferiorly. -

Standardized Review of Atrial Anatomy for Cardiac Electrophysiologists
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/235416273 Standardized Review of Atrial Anatomy for Cardiac Electrophysiologists Article in Journal of Cardiovascular Translational Research · February 2013 DOI: 10.1007/s12265-013-9447-2 · Source: PubMed CITATIONS READS 7 57 5 authors, including: Damián Sánchez-Quintana Gonzalo Pizarro Universidad de Extremadura Spanish National Centre for Cardiovascular R… 167 PUBLICATIONS 3,792 CITATIONS 43 PUBLICATIONS 416 CITATIONS SEE PROFILE SEE PROFILE Jose Ramon Lopez Minguez José Angel Cabrera Hospital Universitario Infanta Cristina de Bad… European University of Madrid 107 PUBLICATIONS 1,174 CITATIONS 100 PUBLICATIONS 2,865 CITATIONS SEE PROFILE SEE PROFILE Some of the authors of this publication are also working on these related projects: REPARA View project Interventional cardiology View project All content following this page was uploaded by Damián Sánchez-Quintana on 11 October 2016. The user has requested enhancement of the downloaded file. All in-text references underlined in blue are added to the original document and are linked to publications on ResearchGate, letting you access and read them immediately. Standardized Review of Atrial Anatomy for Cardiac Electrophysiologists Damián Sánchez-Quintana, Gonzalo Pizarro, José Ramón López-Mínguez, Siew Yen Ho & José Angel Cabrera Journal of Cardiovascular Translational Research ISSN 1937-5387 Volume 6 Number 2 J. of Cardiovasc. Trans. Res. (2013) 6:124-144 DOI 10.1007/s12265-013-9447-2 1 23 Your article is protected by copyright and all rights are held exclusively by Springer Science +Business Media New York. This e-offprint is for personal use only and shall not be self- archived in electronic repositories. -
ANATOMICAL WORD ROOTS Appendix I
Learning Assistance Center University of Hawaii at Manoa ANATOMICAL WORD ROOTS Appendix I When studying anatomy for the first time, many students are confronted with numerous unfamiliar terms that must be mastered, because effective communication requires their use. Some understanding of the derivation of anatomical terms from their classical origins will help to fix their meanings and spelling in mind. The following list is a sampling of the more important word roots used in anatomy, and of the Greek (GK) and Latin (L.) from which they have been derived. Usually only the nominative singular is given for a noun, but the genitive (gen.), nomitive plural (pl.), or diminutive (dim.) is included if sufficiently different or if it has formed the past participle (p.p.), is needed to recognized the root. Most of the examples cited are anatomical structure, but major groups of organisms mention in the book are included, and often a common word is cited to help fix the root in mind. This list of roots is far from inclusive; most familiar words for which the classical and the modern term and meaning are very similar have been omitted; e.g., auditory, cardiac, humerus, pharynx, ulna. Those whose appetites are whetted should consult standard dictionaries or such references as Jaeger (1955) for further study. a – Gr.a or an-, prefix meaning without, not. (agnatha, anapsid) ab – L.ab-, prefix meaning away from. (Abduction) abdom – L.abdomen, abdomen (probably from abdo, to canceal). (Abdomen, Abdominal) acanth – Gr. Akantha, spine, thorn, (Acanthodii) acetabul – L.acetabulum, vinegar cup (from acetum, vinegar). (Acetabulum) acro – Gr.akros, topmost, extreme. -
The Terminal Crest: Morphological Features Relevant to Electrophysiology D Sánchez-Quintana, R H Anderson, J a Cabrera, V Climent, R Martin, J Farré,Syho
406 BASIC RESEARCH Heart: first published as 10.1136/heart.88.4.406 on 1 October 2002. Downloaded from The terminal crest: morphological features relevant to electrophysiology D Sánchez-Quintana, R H Anderson, J A Cabrera, V Climent, R Martin, J Farré,SYHo ............................................................................................................................. Heart 2002;88:406–411 Objective: To investigate the detailed anatomy of the terminal crest (crista terminalis) and its junctional regions with the pectinate muscles and intercaval area to provide the yardstick for structural normality. Design: 97 human necropsy hearts were studied from patients who were not known to have medical histories of atrial arrhythmias. The dimensions of the terminal crest were measured in width and thick- ness from epicardium to endocardium, at the four points known to be chosen as sites of ablation. See end of article for Results: The pectinate muscles originating from the crest and extending along the wall of the append- authors’ affiliations ....................... age towards the vestibule of the tricuspid valve had a non-uniform trabecular pattern in 80% of hearts. Fine structure of the terminal crest studied using light and scanning electron microscopy consisted of Correspondence to: much thicker and more numerous fibrous sheaths of endomysium with increasing age of the patient. 36 Dr S Y Ho, Paediatrics, specimens of 45 (80%) specimens studied by electron microscopy had a predominantly uniform longi- National Heart & Lung Institute, Imperial College, tudinal arrangement of myocardial fibres within the terminal crest. In contrast, in all specimens, the Dovehouse Street, London junctional areas of the terminal crest with the pectinate muscles and with the intercaval area had cross- SW3 6LY, UK; ing and non-uniform architecture of myofibres. -
Cardiac Masses
Cardiac Masses Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Cardiac Masses: Considerations • Definition of the mass – Nature – Location – Benign or malignant • Presentation – Obstruction – Direct myocardial involvement – Embolization – Constitutional or systemic symptoms • Echocardiography is primary modality • Multimodality imaging Cardiac Masses: Differential Diagnosis • Anatomical variants • Implanted devices • Thrombus • Vegetations • Tumors – Primary – Metastatic • Artifacts Anatomical Variants • Left atrium – Pectinate muscles – Q-tip (“warfarin ridge”) • Right atrium – Crista terminalis – Eustachian valve – Chiari network • Ventricles – False bands – Moderator band – Hypertrophy – Papillary muscles – Non-compaction • Pericardium – Pericardial cysts – Pericardial fat • Valves – Excresences – Mitral annular calcification • Lipomatous hypertrophy of interatrial septum • Atrial septal aneurysm • Hiatus hernias Anatomical Variants LAA Th RA Implanted Devices • Pacemaker leads • Cardioverter-defibrillator leads • Right heart catheters • Occluder devices • Prosthetic valves/clips • Foreign bodies Implanted Devices LA RA CT Implanted Devices LA LA RA wire Thrombus • Most common intra-cardiac mass • Location often associated with cardiac pathology – LV thrombus • Acute MI – Estimated 4-15% patients with anterior MI (LV apex) • Dilated cardiomyopathy – DDx: false tendons, trabeculations, artifacts, apical hypertrophy, tumors, non-compaction, Loeffler’s – LA thrombus • Appendage • Body – RA thrombus •