How the Pandemic Should Provoke Systemic Change in the Global Humanitarian System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Peran Pemerintah Bangladesh Dalam Menangatasi Masalah Pekerja Anak Dalam Industri Fast Fashion Tahun 2009-2019
PERAN PEMERINTAH BANGLADESH DALAM MENANGATASI MASALAH PEKERJA ANAK DALAM INDUSTRI FAST FASHION TAHUN 2009-2019 SKRIPSI Diajukan Kepada Program Studi Hubungan Internasional Fakultas Psikologi dan Ilmu Sosial Budaya Universitas Islam Indonesia Untuk Memenuhi Sebagian Dari Syarat Guna Memperoleh Derajat Sarjana S1 Hubungan Internasional oleh: Rafi Pasha Hartadiputra 17323085 PROGRAM STUDI HUBUNGAN INTERNASIONAL FAKULTAS PSIKOLOGI DAN ILMU SOSIAL BUDAYA UNIVERSITAS ISLAM INDONESIA 2021 HALAMAN PENGESAHAN Skripsi dengan Judul: PERAN PEMERINTAH BANGLADESH DALAM MENGATASI MASALAH PEKERJA ANAK DALAM INDUSTRI FAST FASHION TAHUN 2009-2019 Dipertahankan di Depan Penguji Skripsi Prodi Hubungan Internasional Fakultas Psikologi dan Ilmu Sosial Budaya Universitas Islam Indonesia Untuk Memenuhi Sebagian Dari Syarat-Syarat Guna Memperoleh Derajat Sarjana S1 Hubungan Internasional Pada Tanggal: 7 April 2021 Mengesahkan Program Studi Hubungan Internasional Fakultas Psikologi dan Ilmu Sosial Budaya Universitas Islam Indonesia Ketua Program Studi (Hangga Fathana, S.I.P., B.Int.St., M.A) Dewan Penguji: TandaTangan 1. Hadza Min Fadhli Robby, S.IP., M.Sc. 2. Gustri Eni Putri, S.IP., M.A. 3. Hasbi Aswar, S.IP., M.A. HALAMAN PERNYATAAN Yang bertanda tangan di bawah ini,saya : Nama : Rafi Pasha Hartadiputra No. Mahasiswa 17323085 Program Studi : Hubungan Internasional Judul Skripsi :Peran Pemerintah Bangladesh dalam Mengatasi Masalah Pekerja Anak dalam Industri Fast Fashion Tahun 2009- 2019 Melalui surat ini saya menyatakan bahwa : Selama melakukan penelitian dan -
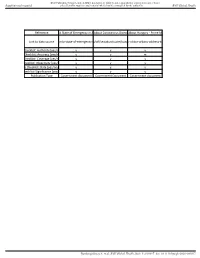
Reference a State of Emergency in Anabout Coronavirus Disease
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health Reference A State of Emergency in AnAbout Coronavirus DiseaseAbout Hungary - Prime Minister Viktor Orbán’s address to the Hungarian parliament before the start of daily business [Internet]. [cited 2020 May 8]. Available from: http://abouthungary.hu/speeches-and-remarks/prime-minister-viktor-orbans-address-to-the-hungarian-parliament-before-the-start-of-daily-business/ Link to data sourcelease.com/a-state-of-emergency-ino.jp/stf/seisakunitsuite/bunya/ister-viktor-orbans-address-to-the-h S Checklist: Authority [yes/no y y y S Checklist: Accuracy [yes/no/ y y m S Checklist: Coverage [yes/no/ y y y S Checklist: Objectivity [yes/no y y y CODS Checklist: Date [yes/no/m y y y S Checklist: Significance [yes/no y y y Publication Type Government document Government Document Government document Bandyopadhyay S, et al. BMJ Global Health 2021; 5:e003097. doi: 10.1136/bmjgh-2020-003097 BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health Actualité [Internet]. [cited Another2 445 coronavirus casesattualita.it. Contagio CoronAustralian Government Depar w.sante.gov.ma/pages/actualites.asp8/another-445-coronavirus-cases-c a/contagio-coronavirus-aggio/resources/publications/coron y m y Y y y m Y y m y Y y y y Y y y y Y y y y Y Government Document Government Document Government Document Government Document Bandyopadhyay S, et al. -

From Cold War to Civil War: 75 Years of Russian-Syrian Relations — Aron Lund
7/2019 From Cold War to Civil War: 75 Years of Russian-Syrian Relations — Aron Lund PUBLISHED BY THE SWEDISH INSTITUTE OF INTERNATIONAL AFFAIRS | UI.SE Abstract The Russian-Syrian relationship turns 75 in 2019. The Soviet Union had already emerged as Syria’s main military backer in the 1950s, well before the Baath Party coup of 1963, and it maintained a close if sometimes tense partnership with President Hafez al-Assad (1970–2000). However, ties loosened fast once the Cold War ended. It was only when both Moscow and Damascus separately began to drift back into conflict with the United States in the mid-00s that the relationship was revived. Since the start of the Syrian civil war in 2011, Russia has stood by Bashar al-Assad’s embattled regime against a host of foreign and domestic enemies, most notably through its aerial intervention of 2015. Buoyed by Russian and Iranian support, the Syrian president and his supporters now control most of the population and all the major cities, although the government struggles to keep afloat economically. About one-third of the country remains under the control of Turkish-backed Sunni factions or US-backed Kurds, but deals imposed by external actors, chief among them Russia, prevent either side from moving against the other. Unless or until the foreign actors pull out, Syria is likely to remain as a half-active, half-frozen conflict, with Russia operating as the chief arbiter of its internal tensions – or trying to. This report is a companion piece to UI Paper 2/2019, Russia in the Middle East, which looks at Russia’s involvement with the Middle East more generally and discusses the regional impact of the Syria intervention.1 The present paper seeks to focus on the Russian-Syrian relationship itself through a largely chronological description of its evolution up to the present day, with additional thematically organised material on Russia’s current role in Syria. -

1 V.9 I.1 Cornell International Affairs Review Board of Advisors
1 V.9 I.1 CORNELL INTERNATIONAL AFFAIRS REVIEW BOARD OF ADVISORS Dr. Heike Michelsen, Primary Advisor Director of Programming, Einaudi Center for International Studies Professor Robert Andolina Cornell Johnson School of Management Professor Ross Brann Department of Near Eastern Studies Professor Matthew Evangelista Department of Government Professor Peter Katzenstein Department of Government Professor Isaac Kramnick Department of Government Professor David Lee Department of Applied Economics and Management Professor Elizabeth Sanders Department of Government Professor Nina Tannenwald Brown University Professor Nicolas van de Walle Department of Government Cornell International Affairs Review, an independent student organization located at Cornell University, produced and is responsible for the content of this publication. This publication was not reviewed or approved by, nor does it necessarily express or reflect the policies or opinions of, Cornell University or its designated representatives. 2 CIAR CORNELL INTERNATIONAL AFFAIRS REVIEW GRADUATE STUDENT SENIOR ADVISORS Wendy Leutert PhD Candidate Department of Government Whitney Taylor PhD Candidate Department of Christine Barker Masters Candidate Cornell Institute for Public Affairs 3 V.9 I.1 PRESIDENTS’ LETTER Lucas Png Cornell University Class of 2017 President, CIAR Thank you for picking up a copy of our latest issue. CIAR is grateful for your sup- port! Our club has grown with an influx of freshmen and new members, and at the end of this current year, we will be passing the torch to the next Executive Board, to continue CIAR’s mission of stimulating discussion about international affairs at Cornell and beyond. The Journal is as stunning as ever. By no means a quick read, it provides insight- ful and thought provoking analysis of important issues at hand. -

EASO COI Query Response Published on 7 November 2019
COI QUERY Country of Origin CONGO, DEMOCRATIC REPUBLIC OF Main subject Situation of single women Question(s) 1. Treatment of single women by society 1.2 Forced marriage: legislation and practices 2. State ability to enforce the law on forced marriage, including information on the existence and effectiveness of dedicated units at the police stations. 3. Access to shelters, employment, and other basic services for single women with or without network Date of completion 25 June 2021 Query Code Q16-2021 Contributing EU+ COI units N/A (if applicable) Disclaimer This response to a COI query has been elaborated according to the EASO COI Report Methodology and EASO Writing and Referencing Guide. The information provided in this response has been researched, evaluated and processed with utmost care within a limited time frame. All sources used are referenced. A quality review has been performed in line with the above mentioned methodology. This document does not claim to be exhaustive neither conclusive as to the merit of any particular claim to international protection. If a certain event, person or organisation is not mentioned in the report, this does not mean that the event has not taken place or that the person or organisation does not exist. Terminology used should not be regarded as indicative of a particular legal position. The information in the response does not necessarily reflect the opinion of EASO and makes no political statement whatsoever. The target audience is caseworkers, COI researchers, policy makers, and decision making authorities. The answer was finalised on 25 June 2021. Any event taking place after this date is not included in this answer. -
A Bridge to Firmer Ground: Learning from International Experiences to Support Pathways to Solutions in the Syrian Refugee Context
A BRIDGE TO FIRMER GROUND: LEARNING FROM INTERNATIONAL EXPERIENCES TO SUPPORT PATHWAYS TO SOLUTIONS IN THE SYRIAN REFUGEE CONTEXT FULL RESEARCH REPORT MARCH 2021 The Durable Solutions Platform (DSP) aims to generate knowledge that informs and inspires forwardthinking policy and practice on the long-term future of displaced Syrians. Since its establishment in 2016, the DSP has developed research projects and supported advocacy efforts on key questions regarding durable solutions for Syrians. In addition, DSP has strengthened the capacity of civil society organizations on solutions to displacement. For more, visit https://www.dsp-syria.org/ The nonpartisan Migration Policy Institute seeks to improve immigration and integration policies through authoritative research and analysis, opportunities for learning and dialogue, and the development of new ideas to address complex policy questions. The Institute is guided by the belief that countries need to have sensible, well thought- out immigration and integration policies in order to ensure the best outcomes for both immigrants and receiving communities. For more, visit https://www.migrationpolicy.org/ This document has been produced with the financial assistance of the European Regional Development and Protection Programme (RDPP II) for Lebanon, Jordan and Iraq, which is supported by the Czech Republic, Denmark, the European Union, Ireland and Switzerland. The contents of this document are the sole responsibility of the Durable Solutions Platform and can under no circumstances be regarded as reflecting the position of the RDPP or its donors. A BRIDGE TO FIRMER GROUND Acknowledgements This report was authored by Camille Le Coz, Samuel Davidoff-Gore, Timo Schmidt, Susan Fratzke, Andrea Tanco, Belen Zanzuchi, and Jessica Bolter. -

The 'New Humanitarian Aid Landscape'
The ‘new humanitarian aid landscape’ Case study: MSF interaction with non-traditional and emerging aid actors in Syria 2013-14 Photo credit © Michael Goldfarb/MSF credit Photo By Jonathan Whittall July 2014 1 Contents Executive summary 1. Introduction 2 2 1.1 Syria’s geopolitical landscape 3 3 2. Research rationale and methodology 5 5 The way in which the Syria war has been fought - and the its dealings with new aid actors – overly reliant on inter- 2.1 Analysis of media reports 5 5 regional geo-political dynamics that frame it - has result- national staff with limited experience in the region - and 2.2 Archive material / primary sources 5 5 ed in a polarized aid environment. Either aid is provided its standards and protocols were seen as a barrier in some officially through Damascus - and subject to huge restric- cases. 2.3 Semi structured interviews 5 5 tions rendering many parts of the country unreachable – 3. Research findings 6 6 or aid is provided directly into opposition controlled areas In such an environment there is an argument to be made without the consent of the Syrian government and subject for a more rapid internationalization of MSF – including 3.1 The parties to the conflict 7 7 to massive insecurity. through the recruitment of staff from the region. In ad- 3.2 Conduct of hostilities 7 7 dition to this, there is a need to ensure that the flexibility The experiences of MSF in attempting to gain official ac- required to work in such an environment exists not only 3.3 Humanitarian implications 10 10 cess to Syria highlight the difficulties for an organisation among the operations line management but also from 3.4 The aid environment: Two parallel systems 12 12 to overcome the defining features of the Syrian govern- both technical support departments and in the profiles of 3.5 Aid delivered officially 13 13 ments approach to aid delivery: What MSF had to offer field workers recruited at all levels. -

The New Humanitarian Basics
HPG Working Paper The new humanitarian basics Marc DuBois May 2018 HPG Humanitarian Policy Group About the author Marc DuBois works as an independent humanitarian analyst and consultant based in London. He previously spent 15 years in various roles with Médecins Sans Frontières (MSF), most recently as the Executive Director of MSF-UK. This Working Paper is part of the HPG series ‘Constructive Deconstruction: Imagining Alternative Humanitarian Action’. Humanitarian Policy Group Overseas Development Institute 203 Blackfriars Road London SE1 8NJ United Kingdom Tel. +44 (0) 20 7922 0300 Fax. +44 (0) 20 7922 0399 E-mail: [email protected] Website: http://www.odi.org/hpg © Overseas Development Institute, 2018 Readers are encouraged to quote or reproduce materials from this publication but, as copyright holders, ODI requests due acknowledgement and a copy of the publication. This and other HPG Reports are available from www. odi.org.uk/hpg. Contents 1 Introduction: prototyping a new humanitarian action 1 2 Setting the stage 3 2.1 What do we mean by ‘humanitarian action’? 3 2.2 Neither a fire department nor a rescue team 3 3 Rescoping crisis response 5 3.1 ‘Seeing’ less humanitarian crisis: rescoping the basis for intervention 5 3.2 Fitting the means to the end: identifying the limits of the humanitarian role 7 4 Towards a humanity-centred humanitarian action 9 4.1 A new humanitarian connectivity: rescoping humanitarian productivity 9 4.2 Going local 10 4.3 The principles of humanitarian action 11 4.4 Reorienting humanitarian protection 13 5 The -

Children and Armed Conflict September 2020
Newsletter on Children’s rights – Children and Armed Conflict September 2020 Table of content Colombia - How Colombia’s armed groups are exploiting COVID-19 to recruit children ............... 1 Global - Prioriser les enfants pour qu’advienne la paix dans le monde .......................................... 2 Global - Security Council demands an end to attacks on schools worldwide ................................. 2 Global - 'I had to kill so many people': the battle to protect children in conflicts .......................... 2 Global - Security Council Open Debate on Children and Armed Conflict: Remarks by Ms. Virginia Gamba, SRSG for Children and Armed Conflict ............................................................................... 2 India - Children worst affected as terror networks spread their tentacles across borders: India at United Nations ................................................................................................................................. 3 Libya - UN chief urges closure of all migrant detention centres in Libya ........................................ 3 Mexico - Conflicto armado y Covid-19 arrebatan educación a los niños indígenas ....................... 3 Sub-Saharan Africa - Experts: Boko Haram Recruiting Children as Soldiers, Suicide Bombers ...... 3 Paraguay - Legisladores buscan penalizar el uso de niños en conflictos armados ......................... 4 Sahel - Les groupes armés continuent d'enrôler les enfants soldats .............................................. 4 United Arab Emirates -

Climate Change and Security in North Africa Focus on Algeria, Morocco and Tunisia
Climate change and security in North Africa Focus on Algeria, Morocco and Tunisia By Sophie Desmidt, ECDPM Research Paper | February 2021 2 Climate change and security in North Africa Contents Contents 2 Acknowledgements 2 Introduction 3 Understanding cascading climate risks: concept and methodology 5 Climate risk assessment for North Africa 8 Cascading climate risks in North Africa 16 Possible future scenarios 29 Implications for Europe 32 Bibliography 37 Acknowledgements I would like to thank various colleagues for the very useful comments they have made on the different drafts of this paper. This includes my colleagues Volker Hauck, Chloe Teevan and Hanne Knaepen, as well as Glada Lahn at Chatham House, for their extensive comments and review. I also want to thank Maëlle Salzinger and Ashley Neat for their excellent research support. Valeria Pintus advised on and helped with the different aspects of the production process, together with Joyce Olders who mastered the layout of this paper. 3 Climate change and security in North Africa Introduction This research paper takes a regional perspective and looks at the cascading climate risks for three countries in North Africa, namely Algeria, Morocco and Tunisia, also known as the Maghreb.1 This region presents a particular challenge with regards to transboundary or – cascading – climate risks, particularly given its high levels of water stress (and the importance of water in several key sectors and systems in the region) and the prediction that the region is bound to become hotter and drier in the future (IEP 2020). Cascading climate risks, or transboundary climate risks, are climate risks that cross national and sectoral borders. -

University of Westminster Eprints
University of Westminster Eprints http://eprints.wmin.ac.uk The road to military humanitarianism: how the human rights NGOs shaped a new humanitarian agenda David Chandler School of Social Sciences, Humanities & Languages Chandler, David C. The Road to Military Humanitarianism: How the Human Rights NGOs Shaped a New Humanitarian Agenda. Human Rights Quarterly 23:3 (2001). 678-700. © The John Hopkins University Press. Reproduced with permission of the John Hopkins University Press. The Eprints service at the University of Westminster aims to make the research output of the University available to a wider audience. Copyright and Moral Rights remain with the authors and/or copyright owners. Users are permitted to download and/or print one copy for non-commercial private study or research. Further distribution and any use of material from within this archive for profit-making enterprises or for commercial gain is strictly forbidden . Whilst further distribution of specific materials from within this archive is forbidden, you may freely distribute the URL of the University of Westminster Eprints (http://eprints.wmin.ac.uk ). In case of abuse or copyright appearing without permission e-mail [email protected]. David Chandler Forthcoming in Human Rights Quarterly, Vol. 23, No. 3, August 2001 The Road to Military Humanitarianism: How the Human Rights NGO’s Shaped A New Humanitarian Agenda Introduction The transformation of humanitarianism from the margins to the centre of the international policy-agenda has been achieved through the redefinition of humanitarian policy and practice and its integration within the fast-growing agenda of human rights. The new international discourse of human rights activism no longer separates the spheres of strategic state and international aid from humanitarianism, but attempts to integrate the two under the rubric of ‘ethical’ or ‘moral’ foreign policy. -

The Human Cost of Nuclear Weapons
The human cost Autumn 2015 97 Number 899 Volume of nuclear weapons Volume 97 Number 899 Autumn 2015 Volume 97 Number 899 Autumn 2015 Editorial: A price too high: Rethinking nuclear weapons in light of their human cost Vincent Bernard, Editor-in-Chief After the atomic bomb: Hibakusha tell their stories Masao Tomonaga, Sadao Yamamoto and Yoshiro Yamawaki The view from under the mushroom cloud: The Chugoku Shimbun newspaper and the Hiroshima Peace Media Center Tomomitsu Miyazaki Photo gallery: Ground zero Nagasaki Akitoshi Nakamura Discussion: Seventy years after Hiroshima and Nagasaki: Reflections on the consequences of nuclear detonation Tadateru Konoé and Peter Maurer Nuclear arsenals: Current developments, trends and capabilities Hans M. Kristensen and Matthew G. McKinzie Pursuing “effective measures” relating to nuclear disarmament: Ways of making a legal obligation a reality Treasa Dunworth The human costs and legal consequences of nuclear weapons under international humanitarian law Louis Maresca and Eleanor Mitchell Chemical, biological, radiological or nuclear events: The humanitarian response framework of the International Committee of the Red Cross Gregor Malich, Robin Coupland, Steve Donnelly and Johnny Nehme Humanitarian debate: Law, policy, action The use of nuclear weapons and human rights The human cost of nuclear weapons Stuart Casey-Maslen The development of the international initiative on the humanitarian impact of nuclear weapons and its effect on the nuclear weapons debate Alexander Kmentt Changing the discourse on nuclear weapons: The humanitarian initiative Elizabeth Minor Protecting humanity from the catastrophic humanitarian consequences of nuclear weapons: Reframing the debate towards the humanitarian impact Richard Slade, Robert Tickner and Phoebe Wynn-Pope An African contribution to the nuclear weapons debate Sarah J.