Mycetoma- a Resurgence
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

10 Mycetoma Revisited.Pdf
Review Articles / Prace Poglądowe MYCETOMA REVISITED NOWE SPOJRZENIE NA MYCETOMA Hassan Iffat, Keen Abid Postgraduate Department of Dermatology, STD & Leprosy Govt. Medical College & Associated SMHS Hospital, Srinagar-Kashmir, India, [email protected] N Dermatol Online. 2011; 2(3): 147-150 Date of submission: 25.02.2011 / acceptance: 06.03.2011 Conflicts of interest: None Abstract Mycetoma or ‘Madura foot’ is a chronic infection of skin and subcutaneous tissues, fascia and bone. It may be caused by true fungi (eumycetoma) or by filamentous bacteria (actinomycetoma). The lesions are composed of suppurating abscesses and draining sinuses with the presence of grains which are characteristic of the etiologic agents. The introduction of new broad spectrum antimicrobials and antifungals offers the hope of improved drug efficacy. This article discusses the historical aspects, epidemiology, clinical findings, laboratory diagnosis and treatment of mycetoma. Streszczenie Mycetoma lub ‘stopa madurska’ to przewlekłe zakaŜenie skóry i tkanki podskórnej, powięzi i kości. MoŜe być spowodowane przez grzyby prawdziwe (eumycetoma) lub bakterie nitkowate (actinomycetoma). Zmiany przedstawiają się jako ropiejące wrzody i zatoki z obecnością ziaren, które są charakterystyczne dla tych czynników etiologicznych. Wprowadzenie nowych o szerokim spektrum antybiotyków i leków przeciwgrzybiczych daje nadzieję na poprawę skuteczności leczenia. W tym artykule omówiono aspekty historyczne, epidemiologię, objawy kliniczne, diagnostykę laboratoryjną i leczeniu mycetoma. -

Niclosamide Is Active in Vitro Against Mycetoma Pathogens
molecules Article Niclosamide Is Active In Vitro against Mycetoma Pathogens Abdelhalim B. Mahmoud 1,2,3,† , Shereen Abd Algaffar 4,† , Wendy van de Sande 5, Sami Khalid 4 , Marcel Kaiser 1,2 and Pascal Mäser 1,2,* 1 Department of Medical Parasitology and Infection Biology, Swiss Tropical and Public Health Institute, 4051 Basel, Switzerland; [email protected] (A.B.M.); [email protected] (M.K.) 2 Faculty of Science, University of Basel, 4001 Basel, Switzerland 3 Faculty of Pharmacy, University of Khartoum, Khartoum 11111, Sudan 4 Faculty of Pharmacy, University of Science and Technology, Omdurman 14411, Sudan; [email protected] (S.A.A.); [email protected] (S.K.) 5 Erasmus Medical Center, Department of Medical Microbiology and Infectious Diseases, 3000 Rotterdam, The Netherlands; [email protected] * Correspondence: [email protected]; Tel.: +41-61-284-8338 † These authors contributed equally to this work. Abstract: Redox-active drugs are the mainstay of parasite chemotherapy. To assess their repurposing potential for eumycetoma, we have tested a set of nitroheterocycles and peroxides in vitro against two isolates of Madurella mycetomatis, the main causative agent of eumycetoma in Sudan. All the tested compounds were inactive except for niclosamide, which had minimal inhibitory concentrations of around 1 µg/mL. Further tests with niclosamide and niclosamide ethanolamine demonstrated in vitro activity not only against M. mycetomatis but also against Actinomadura spp., causative agents of actinomycetoma, with minimal inhibitory concentrations below 1 µg/mL. The experimental compound MMV665807, a related salicylanilide without a nitro group, was as active as niclosamide, indicating that the antimycetomal action of niclosamide is independent of its redox chemistry (which Citation: Mahmoud, A.B.; Abd Algaffar, S.; van de Sande, W.; Khalid, is in agreement with the complete lack of activity in all other nitroheterocyclic drugs tested). -

Recurrent Scedosporium Apiospermum Mycetoma Successfully Treated by Surgical Excision and Terbinafine Treatment: a Case Report and Review of the Literature Eszter J
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Repository of the Academy's Library Tóth et al. Ann Clin Microbiol Antimicrob (2017) 16:31 DOI 10.1186/s12941-017-0195-z Annals of Clinical Microbiology and Antimicrobials CASE REPORT Open Access Recurrent Scedosporium apiospermum mycetoma successfully treated by surgical excision and terbinafine treatment: a case report and review of the literature Eszter J. Tóth1,2, Géza R. Nagy3, Mónika Homa1,2, Marianna Ábrók4, Ildikó É. Kiss4, Gábor Nagy1,2, Zsuzsanna Bata‑Csörgő3, Lajos Kemény3, Edit Urbán4, Csaba Vágvölgyi2 and Tamás Papp1,2* Abstract Background: Scedosporium apiospermum is an emerging opportunistic filamentous fungus, which is notorious for its high levels of antifungal-resistance. It is able to cause localized cutaneous or subcutaneous infections in both immu‑ nocompromised and immunocompetent persons, pulmonary infections in patients with predisposing pulmonary diseases and invasive mycoses in immunocompromised patients. Subcutaneous infections caused by this fungus frequently show chronic mycetomatous manifestation. Case report: We report the case of a 70-year-old immunocompromised man, who developed a fungal mycetoma‑ tous infection on his right leg. There was no history of trauma; the aetiological agent was identified by microscopic examination and ITS sequencing. This is the second reported case of S. apiospermum subcutaneous infections in Hungary, which was successfully treated by surgical excision and terbinafine treatment. After 7 months, the patient remained asymptomatic. Considering the antifungal susceptibility and increasing incidence of the fungus, Sce- dosporium related subcutaneous infections reported in the past quarter of century in European countries were also reviewed. -

Scedosporium Apiospermum EUMYCETOMA SUCCESSFULLY TREATED with ORAL VORICONAZOLE: REPORT of a CASE and REVIEW of the BRAZILIAN REPORTS on SCEDOSPORIOSIS
Rev. Inst. Med. Trop. Sao Paulo 55(2):121-123, March-April, 2013 doi: 10.1590/S0036-46652013000200010 Scedosporium apiospermum EUMYCETOMA SUCCESSFULLY TREATED WITH ORAL VORICONAZOLE: REPORT OF A CASE AND REVIEW OF THE BRAZILIAN REPORTS ON SCEDOSPORIOSIS Flávio de Mattos OLIVEIRA(1,2), Gisela UNIS(3,4), Bruno HOCHHEGGER(5) & Luiz Carlos SEVERO(2,6,7) SUMMARY We describe a case of white-grain eumycetoma caused by Scedosporium apiospermum in an immunocompetent host that was successfully treated with oral voriconazole, and we review the Brazilian reports on scedosporiosis. KEYWORDS: Scedosporium apiospermum; Pseudallescheria boydii; Scedosporiosis; Eumycetoma, Voriconazole. INTRODUCTION examination revealed a tumor-like process of the foot that had several draining sinus tracts (Fig. 1). Foot plain radiography showed widening The asexual state of the ascomycete Scedosporium apiospermum of joint spaces, periostial reaction, bone destruction, erosive changes (previously known as Monosporium apiospermum) and its sexual and demineralization (Fig. 2). An incisional skin biopsy was taken from state, Pseudallescheria apiosperma (previously Allescheria boydii, the foot over opening draining sinuses. Haematoxilin and eosin stain Petriellidium boydii and Pseudallescheria boydii), are ubiquitous demonstrated a granulomatous response on the dermis and subcutaneous saprobic fungi commonly found in temperate climates, and have been tissue containing localized abscesses with spherical white-grain recovered from water, sewage, soil, swamps, and manure2,4. Both sexual eumycetoma. Culture of a sample of the biopsy on Sabouraud glucose forms are frequently seen in human infections (scedosporiosis), both agar revealed fungal growth identified as S. apiospermum. as the cause of systemic disease in immunocompromised patients and eumycetoma in immunocompetent patients2. Eumycetoma is a chronic progressive granulomatous infection of the subcutaneous tissue. -
Acremonium Mycetoma: a Case Report and Discussion
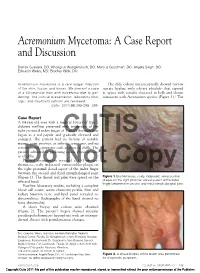
Acremonium Mycetoma: A Case Report and Discussion Denise Guevara, DO; Khongruk Wongkittiroch, DO; Marcus Goodman, DO; Angela Singh, DO; Eduardo Weiss, MD; Bradley Glick, DO Acremonium mycetoma is a rare fungal infection The slide culture microscopically showed narrow of the skin, tissue, and bones. We present a case septate hyphae with solitary phialides that tapered of a 64-year-old man with mycetoma due to gar- at apices with conidia clustered in balls and chains dening. The clinical presentation, laboratory find- consistent with Acremonium species (Figure 3).1 The ings, and treatment options are reviewed. Cutis. 2011;88:293-295, 299. Case Report A 64-year-old man with a medical history of type 2 diabetes mellitus presented with tenderness of the right proximal index finger of 1 year’s duration that began as a red papule and gradually elevated and enlarged. The patient had CUTISno history of notable trauma, pain, pruritus, or arthritic symptoms, and no constitutional symptoms such as fever or chills. The patient admitted to gardening exotic plant specices as a hobby. Physical examination revealed a 131-cm ery- thematous, scaly, indurated, verrucouslike plaque on the Doright proximal dorsal aspectNot of the index finger Copy between the second and third interphalangeal joint (Figure 1). The thumb and palm were spared on the Figure 1. Erythematous, scaly, indurated, verrucouslike affected hand. plaque on the right proximal dorsal aspect of the index finger between the second and third interphalangeal joint. Baseline laboratory studies, including a complete blood cell count, serum chemistry profile, liver and kidney function tests, and lipid panel revealed no abnormalities. -

Madurella Mycetomatis
Karrakchou et al. BMC Dermatology (2020) 20:1 https://doi.org/10.1186/s12895-019-0097-1 CASE REPORT Open Access Madurella mycetomatis infection of the foot: a case report of a neglected tropical disease in a non-endemic region Basma Karrakchou* , Ibtissam Boubnane, Karima Senouci and Badreddine Hassam Abstract Background: Mycetoma is an uncommon chronic granulomatous infection of cutaneous and subcutaneous tissues that can be caused by filamentous bacteria (actinomycetoma) or fungi (eumycetoma). It is the prerogative of young men between the third and fourth decade and is transmitted through any trauma causing an inoculating point. The classic clinical triad associates a painless hard and swelling subcutaneous mass, multiple fistulas, and the pathognomonic discharge of grains. Although endemic in many tropical and subtropical countries, mycetoma can also be found in non-endemic areas as in Morocco, and causes then diagnosis problems leading to long lasting complications. Therefore, we should raise awareness of this neglected disease for an earlier management. Under medical treatment however, mycetoma has a slow healing and surgery is often needed, and relapses are possible. Case presentation: Herein we report a case of a 64 years old patient, with a history of eumycetoma occurring ten years ago treated with oral terbinafine coupled with surgery. A complete remission was seen after 2 years. He presented a relapse on the previous scar 6 months ago. There wasn’t any bone involvement in the magnetic resonance imaging (MRI). The patient was put under oral terbinafine with a slow but positive outcome. Conclusion: Through this case report, we perform a literature review and highlight the importance of increase awareness of mycetoma in clinical practice especially in non-endemic regions. -

Unusual Presentation of Madurella Mycetomatis Mycetoma in a Paediatric Patient in India
MOJ Clinical & Medical Case Reports Case Report Open Access Unusual presentation of Madurella mycetomatis mycetoma in a paediatric patient in India Abstract Volume 4 Issue 5 - 2016 Eumycetoma due to Madurella mycetomatis is of worldwide occurrence. It usually Uma Tendolkar,1 Binoti Sheth,2 Sujata Baveja,1 presents with signs of tumefaction, sinuses and grains which are the hallmarks in 1 1 diagnosis of the disease. The present case was an eight year old boy admitted Nehal Mehta, Arghadip Samaddar, Santosh 2 1 with moderate swelling of the forearm with a discharging sinus. The swelling had Banshelkikar, Shanta Shubhra Das developed over a four month period. He gave history of trauma one year back to the 1Department of Microbiology, Lokmanya Tilak Municipal Medical site. He also had fever for two months. Imaging studies showed large cystic lesions College & General hospital, India in the bone. On surgical exploration it was observed that a large mass of compacted 2Department of Orthopaedics, LokmanyaTilak Municipal black grains (5cmX4cm) was filling the space between the radius and ulna bones. Medical College & General hospital, India A mycological examination of the black grains revealed fungal hyphae and culture showed growth of Madurella mycetomatis. An extensive surgical debridement and Correspondence: Uma Tendolkar, Professor, Department voriconazole treatment for 6weeks relieved the clinical symptoms but there was little of Microbiology, Lokmanya Tilak Municipal Medical College radiological improvement. This case represents a rare presentation of mycetoma & General hospital, Sion, Mumbai 400 022, India, Tel 91-22- with a rapid progression of the disease over a few months, not commonly seen with 24076381, Email [email protected] eumycotic agents. -

Mycetoma and Other Subcutaneous Mycoses
Lecture Title: Mycetoma and other Subcutaneous Mycoses (Musculoskeletal Block, Microbiology) Lecture Objectives.. 1. Acquire the basic knowledge about mycetoma and the clinical features of the disease 2. Acquire the basic knowledge about other common subcutaneous mycosis and their clinical features. 3. Know the main fungi that affect subcutaneous tissues, muscles and bones. 4. Identify the clinical settings of such infections 5. Know the laboratory diagnosis, and treatment of these infections. SUBCUTANEOUS MYCOSES Fungal infections involving the dermis, subcutaneous tissues, muscle and may extend to bone. They are initiated by trauma to the skin. Are difficult to treat and surgical intervention is frequently employed. Diseases in healthy host, however, more severe disease in immunocompromised host. SUBCUTANEOUS MYCOSES Mycetoma Subcutaneous zygomycosis Sporotrichosis Chromoblastomycosis Pheohyphomycosis Rhinosporidiosis Lobomycosis MYCETOMA Mycetoma is a chronic, granulomatous disease of the skin and subcutaneous tissue, which sometimes involves muscle, and bones. It is characterized by Swelling , abscess formation, and multiple draining sinuses that exude characteristic grains of clumped organisms . It typically affects the lower extremities, but also other areas of the body e.g. hand, back and neck. The disease was first described in the Madura district of India in 1842, (Madura foot). MYCETOMA Classified as : Eumycetoma: those caused by fungi Actinomycetoma: those caused by aerobic filamentous bacteria (Actinomycetes) Mycetoma is endemic in tropical, subtropical, and temperate regions. Sudan, Senegal, Somalia, India, Pakistan, Mexico, Venezuela Is more common in men than in women (ratio is 3:1). Commonly in people who work in rural areas, framers MYCETOMA Mycetoma is acquired via trauma of the skin Trauma painless subcutaneous firm nodule is observed massive swelling with skin rupture, and sinus tract formation old sinuses close and new ones open, draining exudates with grains (granules) Grains may sometimes be seen with the naked eye. -

Agents of Mycetoma
262 262 Agents of Mycetoma DUANE R. HOSPENTHAL* Mycetoma is a chronic progressive granulomatous infection of the transvalensis, Nocardia veterana, Nocardiopsis dassonvillei, and Strepto- skin and subcutaneous tissue most often affecting the lower extremi- myces sudanensis.2,6-8 Actinomycetoma grains are typically white or pale ties, typically a single foot. Disease is unique from other cutaneous or yellow, except those caused by Actinomadura pelletieri, which are red subcutaneous diseases in its triad of localized swelling, underlying to pink. sinus tracts, and production of grains or granules (comprised of aggre- gations of the causative organism) within the sinus tracts. These infec- tions may be caused by fungi and termed eumycotic mycetoma or Epidemiology eumycetoma, or by filamentous higher bacteria, termed actinomycotic The oldest description of this disease appears to date back to the mycetoma or actinomycetoma. The term mycetoma can also be found ancient Indian Sanskrit text Atharva Veda, in which reference is made in the literature incorrectly referring to a fungus ball found in a pre- to pada valmikam, translated to mean “anthill foot.”2 More modern existing cavity in the lung or within a paranasal sinus, most often descriptions from Madras, India, in the 19th century led to this disease caused by Aspergillus spp. Grain formation by infecting organisms is initially being called “madura foot,” or maduromycosis, a term still restricted to the diseases mycetoma, actinomycosis (see Chapter 255), used by some today to describe eumycotic mycetoma. Mycetoma is and botryomycosis. Actinomycosis is a disease produced by the anaer- most commonly found in tropical and subtropical climates, with the obic and microaerophilic higher bacteria that normally colonize the highest incidence being reported from endemic areas in the India mouth and gastrointestinal and urogenital tracts. -

Mycetoma Foot
Central JSM Foot and Ankle Bringing Excellence in Open Access Review Article *Corresponding author Elsheikh Mahgoub, Department of Microbiology, Mycetoma Foot University of Khartoum, Sudan, Email: Submitted: 15 March 2017 Elsheikh Mahgoub* Accepted: 23 March 2017 Department of Microbiology, University of Khartoum, Sudan Published: 25 March 2017 ISSN: 2475-9112 Abstract Copyright Mycetoma is a chronic progressive granulomatous infection characterized © 2017 Mahgoub by a painless swelling, development of sinuses that discharge pus and grains of different colors. It will ultimately involve bone that shows cavities in a plain x-ray. It OPEN ACCESS is important to determine whether the cause is bacterial (Actinomycetoma) or fungal (Eumycetoma) because the former is treated by antibiotics and the latter by antifungal Keywords drugs. Laboratory diagnosis is established by culture of grains or stained sections • Actinomycetoma for Histopathological examination. A good approach for treatment is removal of the • Eumycetoma affected tissue followed by antibiotic or antifungal for a period of about nine months. • Madurella mycetomatis The patient is to be followed up carefully for fear of side effects of the drug. INTRODUCTION Mycetoma Foot is an improvement on the old name Madura On examination the skin is attached to a firm swelling with in Actinomycetoma. Skin may remain normal or become dark foot which was coined by Carter in 1874 to describe a condition defined border in case of Eumycetoma but the margin diffuses colored or depigmented. It may also show more sweating than that affected a patient from Madura District in South West India the other limb. The inguinal lymph nodes may be enlarged due [1]. -

The Global Distribution of Actinomycetoma and Eumycetoma
PLOS NEGLECTED TROPICAL DISEASES REVIEW The global distribution of actinomycetoma and eumycetoma 1 2,3 Darcy EmeryID , David W. DenningID * 1 Manchester Medical School, University of Manchester, Manchester, United Kingdom, 2 The University of Manchester, National Aspergillosis Centre, Wythenshawe Hospital, Manchester Academic Health Science Centre, United Kingdom, 3 Global Action Fund for Fungal Infections, Geneva, Switzerland * [email protected] Abstract Background Mycetoma, a chronic infection of the skin and underlying structures, affects those with a close relationship to the land, often in resource-poor areas of the world. Whether caused by any one of a variety of fungus or bacteria, mycetoma causes significant disability and mortal- ity. Acknowledged as a neglected tropical disease (NTD) by the World Health Organization a1111111111 a1111111111 (WHO) in 2016, mycetoma is susceptible to being misunderstood, misdiagnosed, and mis- a1111111111 managed. In an effort to shift the balance in favor of recognition and effective treatment, a1111111111 sound epidemiological understanding is required. a1111111111 Methods and findings In this paper, a literature review of case reports and series (332 papers in total) is presented OPEN ACCESS as three maps. We identified 19,494 cases dating from 1876 to 2019, with cases contracted Citation: Emery D, Denning DW (2020) The global in 102 countries. The first map shows where mycetoma has ever been reported, the second distribution of actinomycetoma and eumycetoma. shows how many cases have been reported, and the third shows the ratio of eumycetoma PLoS Negl Trop Dis 14(9): e0008397. https://doi. (fungal) to actinomycetoma (bacterial). Most cases are found in Mexico, India, and Sudan, org/10.1371/journal.pntd.0008397 where mycetoma is studied rigorously. -

Series Fungal Infections 4 Neglected Endemic Mycoses
Series Fungal infections 4 Neglected endemic mycoses Flavio Queiroz-Telles, Ahmed Hassan Fahal, Diego R Falci, Diego H Caceres, Tom Chiller, Alessandro C Pasqualotto Fungi often infect mammalian hosts via the respiratory route, but traumatic transcutaneous implantation is also an Lancet Infect Dis 2017 important source of infections. Environmental exposure to spores of pathogenic fungi can result in subclinical and Published Online unrecognised syndromes, allergic manifestations, and even overt disease. After traumatic cutaneous inoculation, July 31, 2017 several fungi can cause neglected mycoses such as sporotrichosis, chromoblastomycosis, mycetoma, http://dx.doi.org/10.1016/ S1473-3099(17)30306-7 entomophthoramycosis, and lacaziosis. Most of these diseases have a subacute to chronic course and they can become See Online/Series recalcitrant to therapy and lead to physical disabilities, including inability to work, physical deformities, http://dx.doi.org/10.1016/ and amputations. For many years, paracoccidioidomycosis was considered the most prevalent endemic systemic S1473-3099(17)30303-1, mycosis in the Americas, but this situation might be changing with recognition of the worldwide presence of http://dx.doi.org/10.1016/ Histoplasma capsulatum. Both paracoccidioidomycosis and histoplasmosis can mimic several infectious and non- S1473-3099(17)30304-3, http://dx.doi.org/10.1016/ infectious medical conditions and lead to death if not recognised early and treated. Cutaneous implantation and S1473-3099(17)30309-2, systemic mycoses are neglected diseases that affect millions of individuals worldwide, especially in low-income http://dx.doi.org/10.1016/ countries where their management is suboptimum because challenges in diagnosis and therapeutic options are S1473-3099(17)30316-X, substantial issues.