VITREO RETINAL SOCIETY - INDIA Official Website : Aug 2016
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Activity Report 2009 – 2010
Activity Report 2009 – 2010 L V Prasad Eye Institute Kallam Anji Reddy Campus L V Prasad Marg, Banjara Hills Hyderabad 500 034, India Tel: 91 40 3061 2345 Fax: 91 40 2354 8271 e-mail: [email protected] L V Prasad Eye Institute Patia, Bhubaneswar 751 024 Orissa, India Tel: 91 0674 3989 2020 Fax: 91 0674 3987 130 e-mail: [email protected] L V Prasad Eye Institute G M R Varalakshmi Campus Door No: 11-113/1 Hanumanthawaka Junction Visakhapatnam 530 040 Andhra Pradesh, India Tel: 91 0891 3989 2020 Fax: 91 0891 398 4444 L V Prasad Eye Institute e-mail: [email protected] Excellence • Equity • Effi ciency Art with vision, for vision Artist-in-residence Sisir Sahana in his workshop on A view of the Art Gallery on Level 6 at Hyderabad LVPEI’s Kallam Anji Reddy campus, Hyderabad creating campus, where several works by Mr Surya Prakash, one of his signature glass sculptures. Inset: A piece from our senior artist-in-residence are on display. his latest collection, entitled “The long climb”. Inset: The hand that wields the paintbrush! L V Prasad Eye Institute Committed to excellence and equity in eye care Activity Report April 2009 – March 2010 Collaborating Centre for Prevention of Blindness L V Prasad Eye Institute, a not-for-profi t charitable organization, is governed by two trusts: Hyderabad Eye Institute and Hyderabad Eye Research Foundation. Donations to Hyderabad Eye Research Foundation are 175% exempt under section 35 (i) (ii) and donations made to Hyderabad Eye Institute are 50% exempt under section 80G of the Income Tax Act. -
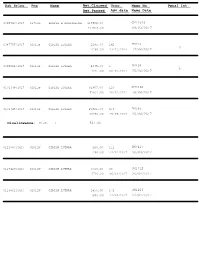
Dak Srlno. Pno Name Amt.Claimed Amt.Passed Adv.Date Vrno. Memo No. Memo Date Penal Int. Disallowance: Misc.
Dak Srlno. Pno Name Amt.Claimed Vrno. Memo No. Penal Int. Amt.Passed Adv.date Memo Date 0098743/1617 01701R PRADIP K CHATTERJEE 117959.00 CM17349 117959.00 09/03/2017 0087755/1617 02011W GIRISH LUTHRA 2280.00 142 DM310 3 2280.00 13/12/2016 17/04/2017 0095822/1617 02011W GIRISH LUTHRA 4335.00 1 DM494 2 4335.00 02/01/2017 25/04/2017 0101338/1617 02011W GIRISH LUTHRA 91857.00 123 CM1060 91857.00 16/01/2017 18/04/2017 0101345/1617 02011W GIRISH LUTHRA 20821.00 916 DM563 20280.00 19/09/2016 26/04/2017 Disallowance: Misc. : 541.00 0111987/1617 02011W GIRISH LUTHRA 260.00 112 DM7417 260.00 14/02/2017 30/03/2017 0129420/1617 02011W GIRISH LUTHRA 3720.00 68 CM1712 3720.00 06/03/2017 26/04/2017 0129861/1617 02011W GIRISH LUTHRA 1850.00 171 CM1403 1850.00 14/03/2017 24/04/2017 Dak Srlno. Pno Name Amt.Claimed Vrno. Memo No. Penal Int. Amt.Passed Adv.date Memo Date 0130742/1617 02011W GIRISH LUTHRA 150.00 CM1973 150.00 28/04/2017 0114746/1617 02272N SARISH MATHUR 24284.00 246 CM19094 24284.00 27/01/2017 31/03/2017 0101476/1617 02426N DINESH K SHARMA 105710.00 CM18173 89244.00 22/03/2017 Disallowance: Luggage/Baggage : 6825.00 Conveyance of Vehicle : 4466.00 Misc. : 5175.00 0110497/1617 02454A SUBASH R GOUNIYAL 3558.00 CM18068 3558.00 21/03/2017 0116874/1617 02454A SUBASH R GOUNIYAL 80316.00 217 DM46 2192 80316.00 19/12/2016 04/04/2017 0127337/1617 02454A SUBASH R GOUNIYAL 4950.00 CM1081 4950.00 18/04/2017 0102758/1617 02484W AJAY K PANDEY 47193.00 226 CM16899 47193.00 22/11/2016 01/03/2017 0111315/1617 02484W AJAY K PANDEY 18186.00 104 DM7008 192 18186.00 13/01/2017 08/03/2017 Dak Srlno. -

The Indian Journal of Medical Research.Pdf
.X' Volume 139 Number 1 January 2014 ISSN: 0971-5916 Estd : 1913 Submit online: littp://\v>v>v.journalonweb.coiii/ijnir THE INDIAN JOURNAL OF MEDICAL RESEARCH nevXS INDIAN COUNCIL OF MEDICAL RESEARCH NEW DELHI www.ijmp.org.ip Indian J Med Res 139, January 2014, pp 1-184 Contents Editorial Alzheimer's disease prevention & acetyl salicylic acid: a believable story Massimiliano Pomponi & Massimo F.L. Pomponi Commentaries Approach to the diagnosis ofdevelopmental delay - The changing scenario Neerja Gupta & Madhulika Kabra India can do more about intestinal worm infections Nilanthi de Silva Review Articles Role ofgut pathogens in development ofinitable bowel syndrome Madhiisudan Grover Probiotic foods: Can their increasing use in India ameliorate the burden of chronic lifestyle disorders? Neerja Hajela, G. Balakrish Nair, B.S. Ramah'ishna & N.K. Ganguly Distribution ofgenetic polymorphisms ofgenes encoding drug metabolizing enzymes & drug transporters - a review with Indian perspective Gurusamy Umamaheswaran, Dhakchinamoorthi Krishna Kumar & Chandrasekaran Adithan Original Articles Clinical utility ofmultiplex ligation-dependent probe amplification technique in identification ofaetiology of unexplained mental retardation: A study in 203 Indian patients Vy'ay R. Boggula, Anju Shukla, Siimita Danda, Sankar V. Hariharan, Sheela Nampoothiri, Rashmi Kumar <& Shubha R. Phadke Prevalence & risk factors for soil transmitted helminth infection among school children in south India Deepthi Kattula, Rajiv Sarkar, Sitara Swarna Rao Ajjampur, Shantidani Minz, Bruno Levecke, Jayaprakash Muliyil & Gagandeep Kang Association between obstetric complications & previous pregnancy outcomes with current pregnancy outcomes in Uttar Pradesh, India Deepti Singh, Srinivas Goli & Sulabha Parsuraman Endophthalmitis patients seen in a tertiaiy eye care centre in Odisha: A clinico-microbiological analysis Savitri Sharma, Tapas R. -

Sakthy Academy Coimbatore
Sakthy Academy Coimbatore Bharat Ratna Award: List of recipients Year Laureates Brief Description 1954 C. Rajagopalachari An Indian independence activist, statesman, and lawyer, Rajagopalachari was the only Indian and last Governor-General of independent India. He was Chief Minister of Madras Presidency (1937–39) and Madras State (1952–54); and founder of Indian political party Swatantra Party. Sarvepalli He served as India's first Vice- Radhakrishnan President (1952–62) and second President (1962–67). Since 1962, his birthday on 5 September is observed as "Teachers' Day" in India. C. V. Raman Widely known for his work on the scattering of light and the discovery of the effect, better known as "Raman scattering", Raman mainly worked in the field of atomic physics and electromagnetism and was presented Nobel Prize in Physics in 1930. 1955 Bhagwan Das Independence activist, philosopher, and educationist, and co-founder of Mahatma Gandhi Kashi Vidyapithand worked with Madan Mohan Malaviya for the foundation of Banaras Hindu University. M. Visvesvaraya Civil engineer, statesman, and Diwan of Mysore (1912–18), was a Knight Commander of the Order of the Indian Empire. His birthday, 15 September, is observed as "Engineer's Day" in India. Jawaharlal Nehru Independence activist and author, Nehru is the first and the longest-serving Prime Minister of India (1947–64). 1957 Govind Ballabh Pant Independence activist Pant was premier of United Provinces (1937–39, 1946–50) and first Chief Minister of Uttar Pradesh (1950– 54). He served as Union Home Minister from 1955–61. 1958 Dhondo Keshav Karve Social reformer and educator, Karve is widely known for his works related to woman education and remarriage of Hindu widows. -
Apvrs 2017 Final Program
OCT2 Module and OCT Angiography Module CONTENTS 1 FOREWORD & WELCOME MESSAGES ��������������������������������������������������������������������������3 1.1 FOREWORD – Congress President Dr Kenneth FONG ........................................................................................ 5 1.2 FOREWORD – Scientific Program Committee Chair A/Prof Andrew CHANG ..................................................... 6 1.3 WELCOME MESSAGE – Asia-Pacific Vitreo-retina Society President Dr Taraprasad DAS ................................... 7 1.4 WELCOME MESSAGE – Asia-Pacific Vitreo-retina Society Secretary-General Prof Dennis LAM ........................ 8 1.5 WELCOME MESSAGE – Malaysia Ministry of Health Director-General Datuk Dr Noor Hisham ABDULLAH ...... 9 2 COUNCILS & COMMITTEES �����������������������������������������������������������������������������������������11 2.1 HOSTS ................................................................................................................................................................. 13 2.1.1 Asia-Pacific Vitreo-retina Society ............................................................................................................... 13 2.1.2 Malaysian Society of Ophthalmology ........................................................................................................ 14 2.2 SCIENTIFIC PROGRAM COMMITTEE ................................................................................................................ 15 2.3 SUBMITTED PROGRAM COMMITTEE .............................................................................................................. -

Annual Activity Report April 2004 - March 2005
AnnualAnnual ActivityActivity ReportReport AprilApril 20042004 -- MarchMarch 20052005 Committed to excellence and equity in eye care L V Prasad Eye Institute L V Prasad Marg, Banjara Hills, Hyderabad 500 034, India L V Prasad Eye Institute Phone: 91 40 3061 2345 Fax: 91 40 2354 8271 Hyderabad, India Email: [email protected] Web site: www.lvpei.org Our Mission The mission of L V Prasad Eye Institute is to be a centre of excellence in eye care services, basic and clinical research into eye diseases and vision- threatening conditions, training, product development, and rehabilitation for those with incurable visual disability, with a focus on extending equitable and efficient eye care services to underserved populations in the developing world. Untitled 2005 Acrylic on canvas 58” x 44” painting by Surya Prakash L V Prasad Eye Institute Committed to excellence and equity in eye care Annual Activity Report April 2004 - March 2005 World Health Organization Collaborating Centre for Prevention of Blindness L V Prasad Eye Institute Hyderabad, India L V Prasad Eye Institute is a not-for-profit charitable organization. Director, Dr Kallam Anji Reddy Distinguished Chair of Ophthalmology Ravi Thomas Uveitis & Ocular Immunology EYE HOSPITAL Virender S Sangwan Cornea & Anterior Segment Somasheila Murthy Virender S Sangwan Prashant Garg Strabismus Pravin V Krishna B Venkateshwar Rao Somasheila Murthy Ravi Thomas Gullapalli N Rao Jyoti Matalia M S Sridhar K Ramesha Optometry B Ramamurthy J Ganesh Babu Jayeeta Bose Neuro-ophthalmology Devraj Goud -
Activity Report 2010 – 2011
L V Prasad Eye Institute Excellence • Equity • Effi ciency Gardens at LVPEI ACTIVITY REPORT 2010 – 2011 Secondary Centres © LVPEI/2011 Vision To create excellent and equitable eye care systems that reach all those in need. Mission The mission of L V Prasad Eye Institute is to be a centre of excellence in eye care services, basic and clinical research into eye diseases and vision-threatening conditions, training, product development, and rehabilitation for those with incurable visual disability, with a focus on extending equitable and effi cient eye care to underserved populations in the Cover: In Braille L V Prasad Eye Institute developing world. So that all may see Activity Report 2010-2011 L V Prasad Eye Institute Committed to excellence and equity in eye care AACTIVITYCTIVITY RREPORTEPORT AAprilpril 22010010 – MMarcharch 22011011 Excellence | Equity | Effi ciency 2 The LVPEI Eye Health Pyramid 3 Activity Report 2010–2011 The year at a glance The LVPEI pyramid of service delivery touches all levels of society, from remote rural villages to busy urban centres. From primary eye care to advanced tertiary (quaternary), we have provided eye care services to hundreds of thousands of people, without compromising on quality. This year, we reached a total of 1,396,741 people including 181,534 children through these various levels of care. Of this almost a million (989,316) received eye care services entirely free of cost as part of our community programs and through our higher-level facilities. Ripples from our circle of impact on people’s life and sight continue to spread beyond our campuses’ and nation’s boundaries. -

English Version
NATIONAL ACADEMY OF MEDICAL SCIENCES (INDIA) ANNUAL REPORT 2013-14 Postal Address: NATIONAL ACADEMY OF MEDICAL SCIENCES (INDIA) NAMS House, Ansari Nagar, Mahatma Gandhi Marg, New Delhi – 110029 Telephone: 011-26588718, 26589326 President : 011-26588792 Secretary : 011-26589289 Fax No.: 011-26588992 E-mail: [email protected] Website: http://nams-india.in 2 CONTENTS Page no. The Council ─ 2013-14 4 Officers & Executive Staff 5 Editorial Board of Annals of NAMS 6 A. Organizational Activities 7-63 Annual Meeting 8 Award of Fellowships & Memberships at the Annual Meeting 9-17 Lifetime Achievement Award 18 Orations and Awards 19-21 Prof. J.S. Bajaj Award 22 Meetings of the Council 23 Election of Fellows – 2013 23-26 Election of Members – 2013 26-32 Candidates proposed for Membership (MNAMS) on passing DNB Examination 33-40 Fellows/Members on rolls of the Academy 41 Nominations of Medical Scientists for Orations and Awards – 2013-14 42-45 Golden Jubilee Commemoration Award Lecture 46 Maintenance of Building 47 Publication of Annals 47 Obituary 48 Text of the address by the President Dr. C.S. Bhaskaran, delivered at the Annual 49-53 Convocation on 26th October 2013, at Jodhpur (Annexure I) Text of the address by the Chief Guest Dr. R. Chidambaram, Principal Scientific Advisor, 54-57 Govt. of India, at the Annual Convocation on 26th October 2013, at Jodhpur (Annexure II) Text of the address by the Guest of Honour Prof. J.S. Bajaj, Emeritus President, NAMS 58-63 at the Annual Convocation on 26th October 2013, at Jodhpur (Annexure III) B. Academic -

Clinical Ophthalmology Medical and Surgical Approach
Clinical Ophthalmology MEDICAL AND SURGICAL APPROACH Clinical Ophthalmology MEDICAL AND SURGICAL APPROACH Second Edition Editor SANDEEP SAXENA MS MAMS Member, National Academy of Medical Sciences, India DAAD Visiting Professor, University of Bonn, Bonn, Germany Visiting Professor, UNC-Chapel Hill, Chapel Hill, USA Fellow, Barnes Retina Institute and Anheuser-Busch Eye Institute, St Louis, USA Fellow, New York-Presbyterian Hospital, New York, USA Professor, Department of Ophthalmology CSM Medical University (Erstwhile, King George’s Medical University) Lucknow, Uttar Pradesh, India Published by Jitendar P Vij Jaypee Brothers Medical Publishers (P) Ltd Corporate Office 4838/24 Ansari Road, Daryaganj, New Delhi - 110002, India, Phone: +91-11-43574357, Fax: +91-11-43574314 Registered Office B-3 EMCA House, 23/23B Ansari Road, Daryaganj, New Delhi - 110 002, India Phones: +91-11-23272143, +91-11-23272703, +91-11-23282021 +91-11-23245672, Rel: +91-11-32558559, Fax: +91-11-23276490, +91-11-23245683 e-mail: [email protected], Website: www.jaypeebrothers.com Offices in India • Ahmedabad, Phone: Rel: +91-79-32988717, e-mail: [email protected] • Bengaluru, Phone: Rel: +91-80-32714073, e-mail: [email protected] • Chennai, Phone: Rel: +91-44-32972089, e-mail: [email protected] • Hyderabad, Phone: Rel:+91-40-32940929, e-mail: [email protected] • Kochi, Phone: +91-484-2395740, e-mail: [email protected] • Kolkata, Phone: +91-33-22276415, e-mail: [email protected] • Lucknow, Phone: +91-522-3040554, -

Annual Report (2011-2012)
ExcellenceExcellence Equity Equity EfficiencyEfficiency L V Prasad Eye Institute L V Prasad Eye Institute So that all may see Kallam Anji Reddy Campus L V Prasad Marg, Banjara Hills Hyderabad 500 034, India Tel: 91 40 3061 2345 Fax: 91 40 2354 8271 email: [email protected] L V Prasad Eye Institute Patia, Bhubaneswar 751 024 Orissa, India Tel: 91 0674 3989 2020 Fax: 91 0674 3987 130 email: [email protected] L V Prasad Eye Institute G M R Varalakshmi Campus Door No: 11-113/1 Hanumanthawaka Junction Visakhapatnam 530 040 Andhra Pradesh, India Tel: 91 0891 3989 2020 Fax: 91 0891 398 4444 email: [email protected] L V Prasad Eye Institute 2011 – 2012 Kode Venkatadri Chowdary Campus Tadigadapa, Vijayawada 521137 Andhra Pradesh, India Activity Report Tel: 91 0866 3062020 e-mail: [email protected] Celebrating 25 years of excellence in eye care 25 Years of Sight, Strength, Dedication, Care Sisir Sahana, Glass and Mixed Media 2012 The LVPEI Eye Health Pyramid Artists Workshop at LVPEI Hyderabad: clockwise from below, Gurucharan Singh, Veer Munshi, Paramjit Singh, Madhvi Parekh, Sidharth, Prabhakar Kolte, Manu Parekh (August 2011) Vision To create excellent and equitable eye care systems that reach all those in need. Mission The mission of L V Prasad Eye Institute is to be a centre of excellence in eye care services, basic and clinical research into eye diseases and vision-threatening conditions, training, product development, and rehabilitation for those with incurable visual disability, with a focus on extending equitable and efficient eye care to underserved populations in the developing world.