Drugs Formulary
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
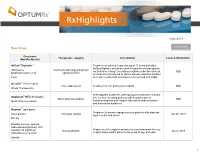
July 2019 New Drugs
July 2019 Learn more New drugs Drug name Therapeutic category Indication(s) Launch information Manufacturer(s) AirDuo® Digihaler™ Treatment of asthma in patients aged 12 years and older. AirDuo Digihaler should be used for patients not adequately (fluticasone Corticosteroid/ long-acting beta controlled on a long term asthma control medication such as TBD propionate/salmeterol) agonist (LABA) an inhaled corticosteroid or whose disease warrants initiation Teva of treatment with both an inhaled corticosteroid and LABA Accrufer® (ferric maltol) Iron replacement Treatment of iron deficiency in adults TBD Shield Therapeutics ® Anticoagulant in patients undergoing percutaneous coronary Angiomax RTU (bivalrudin) intervention, including patients with heparin-induced Direct thrombin inhibitor TBD MAIA Pharmaceuticals thrombocytopenia and heparin-induced thrombocytopenia and thrombosis syndrome Baqsimi™ (glucagon) Treatment of severe hypoglycemia in patients with diabetes nasal powder Glucagon analog July 28, 2019 ages 4 years and above Eli Lilly Cuvitru (immune globulin subcutaneous [human], 20% Replacement therapy for primary humoral immunodeficiency solution) 10 mg/50 mL Immunoglobulin July 2, 2019 subcutaneous injection in adult and pediatric patients two years of age and older Baxalta 1 RxHighlights July 2019 Drug name Therapeutic category Indication(s) Launch information Manufacturer(s) Drizalma Sprinkle™ (duloxetine) Treatment of major depressive disorder in adults; generalized Serotonin and norepinephrine anxiety disorder in adults and pediatric -

The Activation of the Glucagon-Like Peptide-1 (GLP-1) Receptor by Peptide and Non-Peptide Ligands
The Activation of the Glucagon-Like Peptide-1 (GLP-1) Receptor by Peptide and Non-Peptide Ligands Clare Louise Wishart Submitted in accordance with the requirements for the degree of Doctor of Philosophy of Science University of Leeds School of Biomedical Sciences Faculty of Biological Sciences September 2013 I Intellectual Property and Publication Statements The candidate confirms that the work submitted is her own and that appropriate credit has been given where reference has been made to the work of others. This copy has been supplied on the understanding that it is copyright material and that no quotation from the thesis may be published without proper acknowledgement. The right of Clare Louise Wishart to be identified as Author of this work has been asserted by her in accordance with the Copyright, Designs and Patents Act 1988. © 2013 The University of Leeds and Clare Louise Wishart. II Acknowledgments Firstly I would like to offer my sincerest thanks and gratitude to my supervisor, Dr. Dan Donnelly, who has been nothing but encouraging and engaging from day one. I have thoroughly enjoyed every moment of working alongside him and learning from his guidance and wisdom. My thanks go to my academic assessor Professor Paul Milner whom I have known for several years, and during my time at the University of Leeds he has offered me invaluable advice and inspiration. Additionally I would like to thank my academic project advisor Dr. Michael Harrison for his friendship, help and advice. I would like to thank Dr. Rosalind Mann and Dr. Elsayed Nasr for welcoming me into the lab as a new PhD student and sharing their experimental techniques with me, these techniques have helped me no end in my time as a research student. -

Antiseptics and Disinfectants for the Treatment Of
Verstraelen et al. BMC Infectious Diseases 2012, 12:148 http://www.biomedcentral.com/1471-2334/12/148 RESEARCH ARTICLE Open Access Antiseptics and disinfectants for the treatment of bacterial vaginosis: A systematic review Hans Verstraelen1*, Rita Verhelst2, Kristien Roelens1 and Marleen Temmerman1,2 Abstract Background: The study objective was to assess the available data on efficacy and tolerability of antiseptics and disinfectants in treating bacterial vaginosis (BV). Methods: A systematic search was conducted by consulting PubMed (1966-2010), CINAHL (1982-2010), IPA (1970- 2010), and the Cochrane CENTRAL databases. Clinical trials were searched for by the generic names of all antiseptics and disinfectants listed in the Anatomical Therapeutic Chemical (ATC) Classification System under the code D08A. Clinical trials were considered eligible if the efficacy of antiseptics and disinfectants in the treatment of BV was assessed in comparison to placebo or standard antibiotic treatment with metronidazole or clindamycin and if diagnosis of BV relied on standard criteria such as Amsel’s and Nugent’s criteria. Results: A total of 262 articles were found, of which 15 reports on clinical trials were assessed. Of these, four randomised controlled trials (RCTs) were withheld from analysis. Reasons for exclusion were primarily the lack of standard criteria to diagnose BV or to assess cure, and control treatment not involving placebo or standard antibiotic treatment. Risk of bias for the included studies was assessed with the Cochrane Collaboration’s tool for assessing risk of bias. Three studies showed non-inferiority of chlorhexidine and polyhexamethylene biguanide compared to metronidazole or clindamycin. One RCT found that a single vaginal douche with hydrogen peroxide was slightly, though significantly less effective than a single oral dose of metronidazole. -

Darolutamide in Nonmetastatic, Castration-Resistant Prostate Cancer
The new england journal of medicine Original Article Darolutamide in Nonmetastatic, Castration-Resistant Prostate Cancer Karim Fizazi, M.D., Neal Shore, M.D., Teuvo L. Tammela, M.D., Ph.D., Albertas Ulys, M.D., Egils Vjaters, M.D., Sergey Polyakov, M.D., Mindaugas Jievaltas, M.D., Murilo Luz, M.D., Boris Alekseev, M.D., Iris Kuss, M.D., Christian Kappeler, Ph.D., Amir Snapir, M.D., Ph.D., Toni Sarapohja, M.Sc., and Matthew R. Smith, M.D., Ph.D., for the ARAMIS Investigators* ABSTRACT BACKGROUND Darolutamide is a structurally unique androgen-receptor antagonist that is under de- From Institut Gustave Roussy, Université velopment for the treatment of prostate cancer. We evaluated the efficacy of darolu- Paris-Sud, Villejuif, France (K.F.); Carolina Urologic Research Center, Myrtle Beach, tamide for delaying metastasis and death in men with nonmetastatic, castration- SC (N.S.); Tampere University Hospital resistant prostate cancer. and University of Tampere, Tampere (T.L.T.), and Orion Pharma, Orion Corporation, METHODS Espoo (A.S., T.S.) — all in Finland; Na- tional Cancer Institute, Vilnius (A.U.), We conducted a randomized, double-blind, placebo-controlled, phase 3 trial involving and Medical Academy, Lithuanian Uni- men with nonmetastatic, castration-resistant prostate cancer and a prostate-specific versity of Health Sciences, Kaunas (M.J.) antigen doubling time of 10 months or less. Patients were randomly assigned in a 2:1 — both in Lithuania; Stradins Clinical University Hospital, Riga, Latvia (E.V.); ratio to receive darolutamide (600 mg [two 300-mg tablets] twice daily) or placebo N.N. Alexandrov National Cancer Center while continuing androgen-deprivation therapy. -

Cross-Linking of Alpha 2-Plasmin Inhibitor to Fibrin by Fibrin- Stabilizing Factor
Cross-linking of alpha 2-plasmin inhibitor to fibrin by fibrin- stabilizing factor. Y Sakata, N Aoki J Clin Invest. 1980;65(2):290-297. https://doi.org/10.1172/JCI109671. Research Article The concentration of alpha 2-plasmin inhibitor in blood plasma is higher than that in serum obtained from the blood clotted in the presence of calcium ions, but is the same as that in serum obtained in the absence of calcium ions. Radiolabeled alpha2-plasmin inhibitor was covalently bound to fibrin only when calcium ions were present at the time of clotting of plasma or fibrinogen. Whereas, when batroxobin, a snake venom enzyme that lacks the ability to activate fibrin- stabilizing factor, was used for clotting fibrinogen, the binding was not observed. When fibrin-stablizing, factor-deficient plasma was clotted, the specific binding of alpha 2-plasmin inhibitor to fibrin did not occur even in the presence of calcium ions and the concentration of alpha 2-plasmin inhibitor in serum was the same as that in plasma. Monodansyl cadaverine, a fluorescent substrate of the fibrin-stablizing factor, was incorporated into alpha 2-plasmin inhibitor by activated fibrin-stablizing factor. All these findings indicate that alpha 2-plasmin inhibitor is cross-linked to fibrin by activated fibrin-stabilizing factor when blood is clotted. Analysis of alpha 2-plasmin inhibitor-incorporated fibrin by sodium dodecyl sulfate gel electrophoresis showed that the inhibitor was mainly cross-linked to polymerized alpha-chains of cross-linked fibrin. Cross-linking of alpha 2-plasmin inhibitor to fibrin renders fibrin clot less susceptible to fibrinolysis by plasmin. -

List of Approved Ndas for Biological Products That Were Deemed to Be Blas on March 23, 2020
List of Approved NDAs for Biological Products That Were Deemed to be BLAs on March 23, 2020 On March 23, 2020, an approved application for a biological product under section 505 of the Federal Food, Drug, and Cosmetic Act (FD&C Act) was deemed to be a license for the biological product under section 351 of the Public Health Service Act (PHS Act) (see section 7002(e)(4)(A) of the Biologics Price Competition and Innovation Act of 2009). To enhance transparency and facilitate planning for the March 23, 2020, transition date, FDA compiled a preliminary list of approved applications for biological products under the FD&C Act that were listed in FDA’s Approved Drug Products with Therapeutic Equivalence Evaluations (the Orange Book) and that would be affected by this transition provision. FDA posted this list on the FDA website in December 2018, and periodically updated this list before the March 23, 2020, transition date. The September 2019 update to this preliminary list added certain administratively closed applications related to approved applications for biological products that were on the December 2018 version of this list. The January 2020 update to the preliminary list reflected a change to the definition of “biological product” made by the Further Consolidated Appropriations Act, 2020, which was enacted on December 20, 2019. Section 605 of this Act further amended the definition of a “biological product” in section 351(i) of the PHS Act to remove the parenthetical “(except any chemically synthesized polypeptide)” from the statutory category of “protein.” FDA has provided below a list of each approved application for a biological product under the FD&C Act that was deemed to be a license (i.e., an approved biologics license application (BLA)) for the biological product on March 23, 2020. -

PROVERA Medroxyprogesterone Acetate Tablets 2.5Mg, 5Mg, 10Mg, 100 Mg, 200 Mg Tablets
PROVERA Medroxyprogesterone acetate tablets 2.5mg, 5mg, 10mg, 100 mg, 200 mg tablets What is in this leaflet establish a regular menstrual breast cancer or breast lumps cycle not diagnosed by your doctor This leaflet answers some common bleeding or discharge from questions about PROVERA. It does certain types of cancer including your nipples not contain all the available cancer of the breast, kidney and information. It does not take the endometrium (the lining of the miscarriage place of talking to your doctor or womb). pharmacist. cancer of the womb or ovary PROVERA, in combination with an uncontrolled high blood estrogen containing medicine, is All medicines have risks and pressure. benefits. Your doctor has weighed used to relieve symptoms of the risks of you taking PROVERA menopause in women with an intact Do not take PROVERA if you are against the benefits it is expected to uterus. This is called hormone pregnant or intend to become have for you. replacement therapy (HRT). pregnant. PROVERA is used to protect the If you have any concerns about lining of the uterus while the PROVERA may affect your taking this medicine, ask your estrogens relieve the symptoms of developing baby if you take it doctor or pharmacist. Keep this menopause. PROVERA is not during pregnancy. leaflet with your medicine. suitable as a HRT treatment in women who have undergone a Do not take PROVERA if the You may need to read it again. hysterectomy. packaging is torn or shows signs of tampering. Do not take Your doctor may have prescribed PROVERA after the expiry date What PROVERA is PROVERA for another purpose. -

Liquid Spray Formulations for Buccal Delivery of Cannabinoids
(19) TZZ_¥__T (11) EP 1 361 864 B1 (12) EUROPEAN PATENT SPECIFICATION (45) Date of publication and mention (51) Int Cl.: of the grant of the patent: A61K 9/08 (2006.01) A61K 9/107 (2006.01) 04.12.2013 Bulletin 2013/49 A61K 36/185 (2006.01) (21) Application number: 02712063.3 (86) International application number: PCT/GB2002/000620 (22) Date of filing: 14.02.2002 (87) International publication number: WO 2002/064109 (22.08.2002 Gazette 2002/34) (54) LIQUID SPRAY FORMULATIONS FOR BUCCAL DELIVERY OF CANNABINOIDS FLÜSSIGE SPRAY FORMULIERUNGEN ZUR BUCCALEN VERABREICHUNG VON CANNABINOIDEN PREPARATIONS DE SPRAY LIQUIDE POUR L’ADMINISTRATION BUCCALE DE CANNABINOIDES (84) Designated Contracting States: (74) Representative: Schiller, Dominic Christopher et AT BE CH CY DE DK ES FI FR GB GR IE IT LI LU al MC NL PT SE TR Harrison Goddard Foote LLP Designated Extension States: 4th Floor, Merchant Exchange RO SI 17-19 Whitworth Street West Manchester M1 5WG (GB) (30) Priority: 14.02.2001 GB 0103638 30.03.2001 US 280044 P (56) References cited: 05.04.2001 US 827158 WO-A-00/25127 WO-A-01/66089 11.05.2001 GB 0111597 WO-A-95/25504 WO-A1-02/32420 07.09.2001 GB 0121715 WO-A1-02/069993 US-A- 3 560 625 12.09.2001 US 951022 • EITAN ALHANATY; ET AL.: "Osmotic fragility of (43) Date of publication of application: liposomes as affected by antihemolytic 19.11.2003 Bulletin 2003/47 compounds" BIOCHIMICA ET BIOPHYSICA ACTA, vol. 339, no. 1, 1974, pages 146-155, (60) Divisional application: XP008008726 10180611.5 / 2 286 793 • PATRICIA S. -

United States Patent (19) 11 Patent Number: 6,019,993 Bal (45) Date of Patent: Feb
USOO6O19993A United States Patent (19) 11 Patent Number: 6,019,993 Bal (45) Date of Patent: Feb. 1, 2000 54) VIRUS-INACTIVATED 2-COMPONENT 56) References Cited FIBRIN GLUE FOREIGN PATENT DOCUMENTS 75 Inventor: Frederic Bal, Vienna, Austria O 116 263 1/1986 European Pat. Off.. O 339 607 4/1989 European Pat. Off.. 73 Assignee: Omrix Biopharmaceuticals S.A., O 534 178 3/1993 European Pat. Off.. Brussels, Belgium 2 201993 1/1972 Germany. 2 102 811 2/1983 United Kingdom. 21 Appl. No.: 08/530,167 PCTUS85O1695 9/1985 WIPO. PCTCH920.0036 2/1992 WIPO. 22 PCT Filed: Mar. 27, 1994 PCT/SE92/ 00441 6/1992 WIPO. 86 PCT No.: PCT/EP94/00966 PCTEP9301797 7/1993 WIPO. S371 Date: Nov.30, 1995 Primary Examiner-Carlos Azpuru Attorney, Agent, or Firm-Jacobson, Price, Holman, & S 102(e) Date: Nov.30, 1995 Stern, PLLC 87 PCT Pub. No.: WO94/22503 57 ABSTRACT PCT Pub. Date: Oct. 13, 1994 A two-component fibrin glue for human application includes 30 Foreign Application Priority Data a) a component A containing i) a virus-inactivated and concentrated cryoprecipitate that contains fibrinogen, and ii) Mar. 30, 1993 EP European Pat. Off. .............. 93105298 traneXamic acid or a pharmaceutically acceptable Salt, 51 Int. Cl." A61F 2/06; A61K 35/14 thereof, and b) component B containing a proteolytic 52 U s C - - - - - - - - - - - - - - - - - - - - - - - - - - -424/426. 530,380, 530/381: enzyme that, upon combination with component A, cleaves, O X O -- O - - - s 530(383. 530ass Specifically, fibrinogen present in the cryoprecipitate of 58) Field of Search 424/426,530,380 component A, thereby, effecting a fibrin polymer. -

Us Anti-Doping Agency
2019U.S. ANTI-DOPING AGENCY WALLET CARDEXAMPLES OF PROHIBITED AND PERMITTED SUBSTANCES AND METHODS Effective Jan. 1 – Dec. 31, 2019 CATEGORIES OF SUBSTANCES PROHIBITED AT ALL TIMES (IN AND OUT-OF-COMPETITION) • Non-Approved Substances: investigational drugs and pharmaceuticals with no approval by a governmental regulatory health authority for human therapeutic use. • Anabolic Agents: androstenediol, androstenedione, bolasterone, boldenone, clenbuterol, danazol, desoxymethyltestosterone (madol), dehydrochlormethyltestosterone (DHCMT), Prasterone (dehydroepiandrosterone, DHEA , Intrarosa) and its prohormones, drostanolone, epitestosterone, methasterone, methyl-1-testosterone, methyltestosterone (Covaryx, EEMT, Est Estrogens-methyltest DS, Methitest), nandrolone, oxandrolone, prostanozol, Selective Androgen Receptor Modulators (enobosarm, (ostarine, MK-2866), andarine, LGD-4033, RAD-140). stanozolol, testosterone and its metabolites or isomers (Androgel), THG, tibolone, trenbolone, zeranol, zilpaterol, and similar substances. • Beta-2 Agonists: All selective and non-selective beta-2 agonists, including all optical isomers, are prohibited. Most inhaled beta-2 agonists are prohibited, including arformoterol (Brovana), fenoterol, higenamine (norcoclaurine, Tinospora crispa), indacaterol (Arcapta), levalbuterol (Xopenex), metaproternol (Alupent), orciprenaline, olodaterol (Striverdi), pirbuterol (Maxair), terbutaline (Brethaire), vilanterol (Breo). The only exceptions are albuterol, formoterol, and salmeterol by a metered-dose inhaler when used -

The Role of Antispasmodics in Managing Irritable Bowel Syndrome
DOI: https://doi.org/10.22516/25007440.309 Review articles The role of antispasmodics in managing irritable bowel syndrome Valeria Atenea Costa Barney,1* Alan Felipe Ovalle Hernández.1 1 Internal Medicine and Gastroenterology specialist Abstract in San Ignacio University Hospital, Pontificia Universidad Javeriana, Bogotá, Colombia. Although antispasmodics are the cornerstone of treating irritable bowel syndrome, there are a number of an- tispasmodic medications currently available in Colombia. Since they are frequently used to treat this disease, *Correspondence: [email protected] we consider an evaluation of them to be important. ......................................... Received: 26/10/18 Keywords Accepted: 11/02/19 Antispasmodic, irritable bowel syndrome, pinaverium bromide, otilonium bromide, Mebeverin, trimebutine. INTRODUCTION consistency. The criteria must be met for three consecutive months prior to diagnosis and symptoms must have started Irritable bowel syndrome (IBS) is one of the most fre- a minimum of six months before diagnosis. (3, 4) quent chronic gastrointestinal functional disorders. It is There are no known structural or anatomical explanations characterized by recurrent abdominal pain associated with of the pathophysiology of IBS and its exact cause remains changes in the rhythm of bowel movements with either or unknown. Nevertheless, several mechanisms have been both constipation and diarrhea. Swelling and bloating are proposed. Altered gastrointestinal motility may contribute frequent occurrences. (1) to changes in bowel habits reported by some patients, and a IBS is divided into two subtypes: predominance of cons- combination of smooth muscle spasms, visceral hypersen- tipation (20-30% of patients) and predominance of dia- sitivity and abnormalities of central pain processing may rrhea (20-30% of patients). -
WHO Model List of Essential Medicines
WHO Model List of Essential Medicines 15th list, March 2007 Status of this document This is a reprint of the text on the WHO Medicines web site http://www.who.int/medicines/publications/essentialmedicines/en/index.html 15th edition Essential Medicines WHO Model List (revised March 2007) Explanatory Notes The core list presents a list of minimum medicine needs for a basic health care system, listing the most efficacious, safe and cost‐effective medicines for priority conditions. Priority conditions are selected on the basis of current and estimated future public health relevance, and potential for safe and cost‐effective treatment. The complementary list presents essential medicines for priority diseases, for which specialized diagnostic or monitoring facilities, and/or specialist medical care, and/or specialist training are needed. In case of doubt medicines may also be listed as complementary on the basis of consistent higher costs or less attractive cost‐effectiveness in a variety of settings. The square box symbol () is primarily intended to indicate similar clinical performance within a pharmacological class. The listed medicine should be the example of the class for which there is the best evidence for effectiveness and safety. In some cases, this may be the first medicine that is licensed for marketing; in other instances, subsequently licensed compounds may be safer or more effective. Where there is no difference in terms of efficacy and safety data, the listed medicine should be the one that is generally available at the lowest price, based on international drug price information sources. Therapeutic equivalence is only indicated on the basis of reviews of efficacy and safety and when consistent with WHO clinical guidelines.