Rail Accident Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reunification East Midlands G R Y E a a W T C Il Entral Ra
DONATE BY TEXT! REUNIFICATION EAST MIDLANDS G R Y E A A W T C IL ENTRAL RA THE UK’S BIGGEST HERITAGE RAILWAY PROJECT Reconnecting two halves of the Great Central Railway and joining them to Network Rail Supported by David Clarke Railway Trust Friends of the Great Central Main Line East Midlands Railway Trust www.gcrailway.co.uk/unify POTENTIAL EXTENSION TO TRAM INTERCHANGE NOTTINGHAM TRANSPORT HERITAGE CENTRE RUSHCLIFFE HALT REUNIFICATION EAST MIDLANDS G R Y E A A W T C IL ENTRAL RA SITE OF EAST LEAKE STATION By replacing five hundred metres of BARNSTONE missing track between two sections N TUNNEL of the Great Central Railway, we can NOT TO SCALE create an eighteen-mile heritage line STANFORD VIADUCT complete with a main line connection. This is no impossible dream - work is CONNECTION TO THE MISSING MIDLAND MAIN LINE underway, but we need your help to SECTION get the next sections built. LOUGHBOROUGH LOCOMOTIVE SHED TO EAST LEAKE AND RUDDINGTON LOUGHBOROUGH CENTRAL STATION A60 ROAD BRIDGE REQUIRES OVERHAULING EMBANKMENT REQUIRES REPAIRING QUORN & WOODHOUSE STATION MIDLAND MAIN LINE BRIDGE ✓ NOW BUILT! FACTORY CAR PARK SWITHLAND CROSSING REQUIRES CONTRUCTION VIADUCT RAILWAY TERRACE BRANCH LINE TO ROAD BRIDGE TO BE CONSTRUCTED USING MOUNTSORREL RECLAIMED BRIDGE DECK HERITAGE CENTRE ROTHLEY EMBANKMENT STATION NEEDS TO BE BUILT POTENTIAL DOUBLE TRACK GRAND UNION TO LEICESTER ✓ CANAL BRIDGE NOW RESTORED LEICESTER NORTH STATION TO LEICESTER REUNIFICATION Moving Forward An exciting adventure is underway. Following Two sections of the work have been the global pandemic, we’re picking up the completed already, which you can read all pace to build an exciting future for the Great about here. -

Crossing the Canal
NOTTINGHAM RUDDINGTON K O O R B A 6 M 0 A H R I A F NOTTINGHAM HERITAGE CENTRE !RUDDINGTON FIELDS" CROSSING THE CANAL RUSHCLIFFE BRITISH HALT GYPSUM EAST LEAKE STATION KINGSTON BROOK EAST LEAKE EAST LEAKE TUNNEL It’s time for Bridging the Gap part two! STANFORD The Great Central is working to VIADUCT reconnect two halves of the railway to LOUGHBOROUGH MIDLAND CROSSING STATION THE CANAL create an eighteen mile heritage line. You’ve already helped us to build a new R I V E LOUGHBOROUGH R S bridge across the Midland Main Line. O A R LOUGHBOROUGH G RAND U CENTRAL NION C Now it’s time to work on the next part of STATION ANAL MIDLAND MAIN LINE the project. We’re raising half a million BARROW UPON SOAR QUORNDON pounds to restore the canal bridge at QUORN & Loughborough and to finish the design WOODHOUSE STATION A6 work for the rest of the reunification scheme. SWITHLAND MOUNTSORREL RESERVOIR HALT MOUNTSORREL MOUNTSORREL HERITAGE BRANCH CENTRE ROTHLEY R I SWITHLAND V E SIDINGS R S O A R ROTHLEY STATION ROTHLEY BROOK A46 MAIN LINE BIRSTALL BRIDGING MlTHE NATION GREAT CENTRAL RAILWAY MUSEUM LEICESTER NORTH LEICESTER STATION The project to reunify A number of major pieces of CROSSING two halves of the Great infrastructure remain to be built. THE CANAL Before we can tackle them, we need to Central Railway is one complete design work and secure of the most ambitious planning permission. But something undertaken by any we can do right now is restore the heritage railway. -

BR Standard Class 6 'Clan Class' Drivers Guide
BR Standard Class 6 'Clan Class' Drivers Guide Steam locomotive expansion pack for Train Simulator BR Standard Class 6 'Clan Class' 1 CONTENTS INTRODUCTION .................................................................................................................. 4 Locomotives ...................................................................................................................... 4 Tenders ............................................................................................................................. 8 Coaches .......................................................................................................................... 11 The ‘Clan’ Project ............................................................................................................ 13 History ......................................................................................................................... 13 72010 modifications ..................................................................................................... 14 The ‘Clan’ Project Patron and President ...................................................................... 15 Where will the locomotive run and where will it be based? ........................................... 16 What will it cost? .......................................................................................................... 16 Find out more ............................................................................................................... 17 INSTALLATION ................................................................................................................. -
Class 460 Train Operating Manual
Class 460 Train Operating Manual Produced by: Master Key Simulations Master Key Simulations Juniper Class 460 Operating Manual - Revision 3 © 2017 Introduction - Page 1 Index Introduction…………………………………………………………………………………3 Technical Specifications…………………………………………………………………..4 Rolling Stock……………………………………………………………………………….5 Cab Layout…………………………………………………………………………………9 Keyboard Controls……………………………………………………………………….17 Controls Description………………………………………………………….………….18 Train Monitoring System..……………………………………………………………….25 Cab Secure Radio……………….……………………………………………………….36 GSM-R Radio…………………….……………………………………………………….39 Train Protection & Warning System……………………………………………………42 Miniature Circuit Breakers……………………………………………………………….45 Safety Isolation & Cut-Out Switches……………………………...……………………47 Warning Indicator Panel…………………………………………………………………48 Door Release Panel……………………………………………………………………...49 Driving Instructions……………………………………………………………………….50 Included Scenarios……………………………………………………………………….54 Advanced Scenario Features…………………………………………………………...55 Summary & Credit………………………………………………………………………..56 Legend ♦ A red diamond indicates the system/feature being described is only partially simulated, or not simulated in its entirety. DISCLAIMER: This manual has been developed solely for use in connection with the Master Key Simulations Class 460 add-on for Train Simulator, and is for entertainment ONLY. It is NOT to be used for training or real-world application. Master Key Simulations Juniper Class 460 Operating Manual - Revision 3 © 2017 Index - Page 2 Introduction The Class -

Great Central Railway Robinson Class 8K 2-8-0 Locomotives (LNER & BR Class O4), and GWR Class 3000 by Peter Sheppard The
Great Central Railway Robinson Class 8K 2-8-0 Locomotives (LNER & BR Class O4), and GWR Class 3000 By Peter Sheppard The first class 8K 2-8-0 freight locomotive was built by the Great Central Railway (GCR) at their Gorton works in 1911. It was to a design by J. G. Robinson. Later there was a large order from the Railway Operating Division of the Royal Engineers (R.O.D.). Class 8M (later O5) locomotives built around the same time were later converted to Class O4. Some locomotives were sent to France during the First World War and were returned. On at least two occasions batches of locomotives were loaned to the GWR by the LNER and then were returned. Some locomotives were bought by the GWR , LNWR and LMS. Some locomotives were requisitioned by the government in 1943 and sent to the Middle East, they never came back. Five more were requisitioned in 1952 and sent to Egypt. Others were sold to Australia and China. Added to this various different modifications were made to the locomotives and each modification formed a different sub class. There were 9 such sub- classes and these were numbered Class O4/1 to O4/8. The reader may think that those numbers total 8 and not 9. The explanation is that there were two sub-classes O4/2. The requirement for the first sub-class O4/2 had ended in 1924 so when a need arose for a new sub class in 1925 the vacant number was re-used. Details of the various sub-classes are given later in this article. -

Scottish Railways: Sources
Scottish Railways: Sources How to use this list of sources This is a list of some of the collections that may provide a useful starting point when researching this subject. It gives the collection reference and a brief description of the kinds of records held in the collections. More detailed lists are available in the searchroom and from our online catalogue. Enquiries should be directed to the Duty Archivist, see contact details at the end of this source list. Beardmore & Co (GUAS Ref: UGD 100) GUAS Ref: UGD 100/1/17/1-2 Locomotive: GA diesel electric locomotive GUAS Ref: UGD 100/1/17/3 Outline and weight diagram diesel electric locomotive Dunbar, A G; Railway Trade Union Collection (GUAS Ref: UGD 47) 1949-67 GUAS Ref: UGD 47/1/6 Dumbarton & Balloch Joint Railway 1897-1909 GUAS Ref: UGD 47/1/3 Dunbar, A G, Railway Trade Union Collection 1869-1890 GUAS Ref: UGD 47/3 Dunbar, A G, Railway Trade Union Collection 1891-1892 GUAS Ref: UGD 47/2 London & North Eastern Railway 1922-49 Mowat, James; Collection (GUAS Ref: UGD 137) GUAS Ref: UGD 137/4/3/2 London & North Western Railway not dated Neilson Reid & Co (GUAS Ref: UGD 10) 1890 North British Locomotive Co (GUAS Ref: UGD 11) GUAS Ref: UGD 11/22/41 Correspondence and costs for L100 contract 1963 Pickering, R Y & Co Ltd (GUAS Ref: UGD 12) not dated Scottish Railway Collection, The (GUAS Ref: UGD 8) Scottish Railways GUAS Ref: UGD 8/10 Airdrie, Coatbridge & Wishaw Junction Railway 1866-67 GUAS Ref: UGD 8/39 Airdrie, Coatbridge & Wishaw Junction Railway 1867 GUAS Ref: UGD 8/40 Airdrie, Coatbridge -
Miscellaneous Items Ref Item Description and Source Notes No
Miscellaneous Items Ref Item Description and Source Notes No. X X003 Scrapbook, photographs - ex. Magazines etc. X004 Scrapbook, newscuttings X007 "Railway Magazine" - 1912 June X012 "Travels at Home" - pub. With authy of G.C X015 Sam Fay - Article, picture, "Vanity Fair" X016 Murder in Pennines - Article, R.W. Jan 1970 X017 Past Glories, station refreshment rooms - V.R.Webster X021 A veteran of the MSLR - Article, R.M. April 1959 X022 Wadsley bridge station - Article, M.R.C X023 Railway development at Aylesbury BM No 55 X024 Diversions over Woodhead RM Jan 1970 X025 Manchester-Sheffield Electrification - Article, R.M. November 1954 X026 Bowbridge Pilot - Article, R.M. Nov. 1954 X027 Abandonment of SAMR? - letter, Dec. 22nd. 1837 X028 Accident book - Mexboro', 1925 X029 "Transport goes to war" - Book, 1942 X033 Occurrence books, mainly from Mexboro' area - B.R 16 no. 1948-58 X036 Prospectus, Preservation Loughborough - G.C.R 1976 X037 Prop. Closure Sheff.-Pen.-Huddersfield Service - Documents 1981 X038 S.Y.P.T.E. Transport Development Plan - Book 1978 X039 Index - G.C.R.J Vol. VIII X040 Index - G.C.R.J Vol. IX X041 Index - G.C.R.J Vol. X X042 Index - G.C.R articles in R.M X043 Index - G.C.R. LDECR articles in R.M X044 History of Railways around Doncaster - Ms, D.L.Franks X045 "The Plight of the Railways" - Leaflet, G.Huxley X046 "I remember" - Glossop - Booklet X049 "Woodhead Wanderer" railtour - Programme X050 Railtour Doncaster - Lincoln area - Programme X051 The Iron horse comes to town - Article, Appleby-Frodingham news, 1959 X054 The Yarborough Hotel - Notes, from Bradshaw 1853 X055 When service had meaning, The Story of and Early Railwayman's life - D.L Franks X056 Seven ages of Rlys - Ms, D.L. -

The Financial Impact of the Great Central Railway's London Extension
The financial impact of the Great Central Railway’s London extension By Tony Sheward © Tony Sheward 2020 1 THE FINANCIAL IMPACT OF THE GREAT CENTRAL RAILWAY’S LONDON EXTENSION 1. Introduction The general opinion of authorities, who have written about the Great Central Railway’s (GCR) London Extension, seems to be that the project was not a financial success and acted as a drag on the company’s performance in the years following its opening. This article attempts to examine the financial results of the GCR in the years immediately leading up to the decision to commit to the project, the construction period, and operations from its opening up to 1913. It seeks to discover whether there were other factors, which influenced its financial performance either positively or negatively. For convenience, the title Great Central Railway is used throughout even though this name was not adopted by the Manchester, Sheffield & Lincolnshire Railway until 1897. A glossary of the abbreviations for the various lines is included at the end. The detailed financial figures are presented in four time periods as follows: a. The Immediate Years Prior to Work on the London Extension 1887-93 b. Construction of the London Extension Phase I 1894-99 c. Construction of the London Extension Phase II 1900-06 d. The Years after Completion of the London Extension Work 1907-13 The article takes as its main source the annual reports of GCR1 and the Railway Returns2. The historical background for the article is mainly taken from published sources, in particular the three-part history of the GCR by George Dow3 and the short history of the GCR by Robert Hartley.4 Although up to 1912, the annual reports were prepared in two half yearly tranches, the information in this article is presented by calendar year for ease of understanding and comparison. -

2019 Graham Farish Catalogue Launched
PRESS INFORMATION 2019 Graham Farish Catalogue Launched Bachmann Europe Plc has today launched its 2019 Graham Farish catalogue at a trade event held in London. The Graham Farish catalogue covers British outline N Scale models. This year, several models will be upgraded to include provision for the fitting of Sound, allowing us to increase the number of SOUND FITTED models following the overwhelming popularity of the Castle Class Steam Locomotive and Class 40 Diesel Locomotive – the first Graham Farish locomotives to be offered with this feature. SOUND FITTED models will now feature the suffix ‘SF’ on their item number which will gradually replace the ‘DS’ suffix that was previously used. New tooling is being developed for the WD 40T ‘Parrot’ Wagon and HKA Bogie Hopper Wagon to further expand our extensive range of wagons. Details of these developments, and a full listing of new items, can be found below. NEW TOOLING N SCALE WAGONS NEW TOOLING – WD 40T ‘PARROT’ BOGIE WAGON 250 wagons were constructed in 1917 to the standard LNWR 40 ton ‘Parrot’ bogie trolley design for the War Department – for use at home and by the French Railways during the First World War. After the war 25 of these were passed over to the LNWR to join the original ‘Parrot’ wagons and a further 140 were sold to the Midland Railway, plus some to the Caledonian Railway. The remainder of the wagons were either left in France or retained for use by the British Military. At the time of the Grouping in 1923, all the wagons in railway company ownership became part of the LMS fleet. -
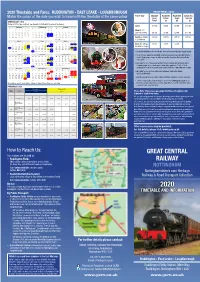
2020 Timetable and Fares: RUDDINGTON
2020 Timetable and Fares: RUDDINGTON - EAST LEAKE - LOUGHBOROUGH TRAIN FARES 2020 Ticket Type Standard Rushcliffe Rushcliffe Cream Tea Match the colour of the date you wish to travel with the timetable of the same colour Rover Return Single Specials Ticket (a) (b) (c) RUNNING DAYS: 2020 Running Days: 2020 (Dates in RED = Special Event. Timetable to be Confirmed) (Dates in RED = Special Event. See Website for further information & timetables) Adult £12.00 £9.00 £7.00 £22.00 January February March M T W T F S Su M T W T F S Su M T W T F S Su 1 2 3 4 5 1 2 1 Child (5 -15 6 7 8 9 10 11 12 3 4 5 6 7 8 9 2 3 4 5 6 7 8 under 5’s FREE) £6.00 £4.50 £3.50 £11.00 13 14 15 16 17 18 19 10 11 12 13 14 15 16 9 10 11 12 13 14 15 20 21 22 23 24 25 26 17 18 19 20 21 22 23 16 17 18 19 20 21 22 27 28 29 30 31 24 25 26 27 28 29 23 24 25 26 27 28 29 Family (2 Adults £30.00 £22.50 £17.50 £55.00 30 31 + 2 Children) April May June M T W T F S Su M T W T F S Su M T W T F S Su Special Events 1 2 3 4 5 1 2 3 1 2 3 4 5 6 7 Dogs (Excluding £3.00 £3.00 £3.00 - 6 7 8 9 10 11 12 4 5 6 7 8 9 10 8 9 10 11 12 13 14 Assistance Dogs) 13 14 15 16 17 18 19 11 12 13 14 15 16 17 15 16 17 18 19 20 21 20 21 22 23 24 25 26 18 19 20 21 22 23 24 22 23 24 25 26 27 28 27 28 29 30 25 26 27 28 29 30 31 29 30 • Rushcliffe Halt lies just to the North of the picturesque village of East Leake. -

Low Res Final
6 061061633 TTOORRNNADOADO THE NewNew Steam Steam forfor thethe Main Main Lin Le ine COMMUNICATION CORD No. 46 Spring 2017 Robin Coombes / Mandy Grant TORNADO! TON UP by Graeme Bunker - James Around 04:00hrs on 12th April 2017 Tornado to facilitate better pathing on busy routes. comes from a need to show that at 10% added another major milestone to the The original view was that simply proving above the certified speed the locomotive record books; the first steam locomotive to the locomotive was up to the task (which is still operating safely. This gives a margin achieve 100mph in the U.K. for 50 years. the original design had already proved when running at 90mph, and is in common The build up to the night’s events has before 1965) would not be sufficient. Many with other traction types. Safety was the been long in the making. It has always been hurdles were to be overcome before trials first priority, gaining data and experience the intention of the Trust that Tornado would be authorised. The decision that the of the locomotive above 75mph being the would be passed for 90mph operations locomotive would be trialled at 100mph objective. ➤ 1 Rob Morland Rob Morland then Driver Hanczar set the locomotive to it down the grade from the summit. For CONTENTS the next 16 miles speed never dropped PAGE 1 below 80mph and a maximum of 97mph Ton up Tornado! was recorded south of Bradbury but the PAGE 5 ‘ton’ still eluded us. The locomotive ran Editorial Walton-on -the-Naze 150th at or over 90mph for seven miles on this Railway celebration section, providing valuable data. -

View from the Vestibule Contents
VIEW FROM THE VESTIBULE As the time comes around to start put- ting The Droplight together, there is always the slight worry - will there be enough material? There were no such worries this time, which is an indica- tion of the level of activity over the past year - a lot has been going on be- hind the scenes to ensure that the LMSCA has a sustainable future, and as far as the `nuts and bolts' side of things is concerned, 2003 was a very successful year for acquiring spares. CONTENTS Indeed, at the time of writing a team has been rescuing gangways for future The Chairman's Ventilator 2 use, in a combined effort with other Finance Report 3 groups. A big `thank you' is due to Time Spent Wisely? 4 everyone who has helped in any way. Membership Report 4 2004 should be an interesting year, 3031 Progress (TK2) 5 with efforts concentrated on finishing Scouse Gold 7 3031 (TK2), and taking the initial steps with the NRM Third Open 7828, not LMSCA and the Carriage forgetting (fingers crossed) the result of Convention 9 our application for charitable status. The LMSCA the National We are fast approaching our first Railway Museum and 7828 10 AGM as mentioned elsewhere. When The Third Open Years 1923-2003 12 we say we would like to see you, we Progressive Railway Carriage really mean it! We also realise that Lifting and Repairing 15 many of you live a fair distance from Scotland Trip 2003 21 Derbyshire and travelling can be diffi- cult at this time of year, but if you pos- Shake, Rattle and Roll 22 sibly can, do please come along.