The Earthquake in Ecuador: Significant Damage to Editorial Health Facilities; Emergency Medical Teams Deployed WHO Emergency Reform
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Instituto Ecuatoriano De Seguridad Social Dirección Del Seguro General De Salud Individual Y Familiar
INSTITUTO ECUATORIANO DE SEGURIDAD SOCIAL DIRECCIÓN DEL SEGURO GENERAL DE SALUD INDIVIDUAL Y FAMILIAR UNIDADES MÉDICAS I.E.S.S. Nº UNIDAD MÉDICA PROVINCIA CIUDAD DIRECCIÓN TELÉFONO REGIONAL 1: Esmeraldas, Pichincha y Santo Domingo de los Tsáchilas 1 Hospital Carlos Andrade Marín Pichincha Quito 18 de Septiembre y Ayacucho PBX: 02-2564939 Nivel III 2 Hospital de Esmeraldas Esmeraldas Esmeraldas Avenidas Colón y Guayas PBX: 06-2712465 Nivel II 3 CAA Central Quito Pichincha Quito Calle Benalcázar N-12 PBX: 02-2957121 4 CAA Chimbacalle Pichincha Quito Av. Napo E-164 y Casitagua PBX: 02-2653444 5 CAA Cotocollao Pichincha Quito Av. De la Prensa 55-118 y Pulida PBX: 02-2590080 6 CAA El Batán Pichincha Quito Av. De las Palmeras y Río Coca Directo: 02-2449369 7 CAA Santo Domingo Santo Domingo Santo Domingo Av. Quito Km 1 s/n y Los Naranjos PBX: 02-2750430 de los Tsáchilas de los Colorados 8 UAA Amaguaña Pichincha Amaguaña Calle José Miranda e Iglesias s/n Directo: 02-2879699 Barrio María Auxiliadora 9 UAA Cayambe Pichincha Cayambe Juan Montalvo 803 y Sucre Directo: 02-2360182 10 UAA La Ecuatoriana Pichincha Quito Av. La Ecuatoriana s/n Directo: 02-2696712 11 UAA Sur Occidental Pichincha Quito Av. Mariscal Sucre 11-27 y Hernando Directo: 02-3103485 Prado Sector El Pintado INSTITUTO ECUATORIANO DE SEGURIDAD SOCIAL DIRECCIÓN DEL SEGURO GENERAL DE SALUD INDIVIDUAL Y FAMILIAR Nº UNIDAD MÉDICA PROVINCIA CIUDAD DIRECCIÓN TELÉFONO 12 UAA San Juan Pichincha Quito Guatemala OE10-352 y San Mateo Directo: 02-2280011 13 UAA Sangolquí Pichincha Sangolquí Eloy Alfaro 112 y Espejo PBX: 02-2331050 Diagonal Estadio Rumiñahui 14 UAA Tabacundo Pichincha Tabacundo Velasco Ibarra 206 Directo: 02-2366008 15 UAA San Lorenzo Esmeraldas San Lorenzo Roberto Luis Cervantes s/n Directo: 06-2780173 REGIONAL 2: Galápagos, Guayas, Los Ríos, Sta. -

Ecuador Malaria General Malaria Information: Predominantly P
Document is provided for sample purposes only. Content is not updated and should not be used for traveler counseling. Ecuador Malaria General malaria information: predominantly P. vivax. Transmission occurs throughout the year. Issues to Consider Location-specific recommendations: Factors favoring chemoprophylaxis Chemoprophylaxis is recommended for all travelers: elevations below 1,500 m (4,900 ft) in most cantons east of the Andes and in • Adventure travel certain cantons of Esmeraldas, Carchi [1], and Cotopaxi [6] provinces; all cities and towns within these areas. • Risk-averse and vulnerable travelers Chemoprophylaxis is recommended for certain travelers (see Issues to Consider box): elevations below 1,500 m in certain • Areas subject to infrequent epidemics cantons east of the Andes and in certain cantons of Carchi [1], Imbabura [2], Guayas [11], and El Oro [15] provinces; all cities • Immigrants visiting friends and relatives and towns within these areas. • Flexible itineraries Travel longer than 1 month Insect precautions only are recommended (negligible transmission is reported): elevations below 1,500 m in various cantons west • of the Andes and certain cantons of Orellana and Zamora-Chinchipe [17] provinces; all cities and towns within these areas except • Unreliable medical expertise and/or treatment drugs at destination Guayaquil, Manta, Portoviejo, Santa Elena, Babahoyo, and Machala. Factors against chemoprophylaxis No preventive measures are necessary (no evidence of transmission exists): the cities of Quito, Guayaquil, Manta, Portoviejo, Santa Elena, Babahoyo, and Machala; the Galápagos Islands; elevations above 1,500 m; all other areas not mentioned above. • Air-conditioned hotels only • Urban areas only Preventive measures: Travelers should observe insect precautions from dusk to dawn in areas with any level of transmission. -

Inventario Preliminar De Las Emisiones De Contaminantes Del Aire
Inventario Preliminar de las Emisiones de Contaminantes del Aire, de los cantones Ambato, Riobamba, Santo Domingo de los Colorados, Latacunga, Ibarra, Manta, Portoviejo, Esmeraldas y Milagro Proyecto Calidad del Aire III Año Base 2010 Quito, 2014 Inventario Preliminar de las Emisiones de Contaminantes del Aire, de los cantones Ambato, Riobamba, Santo Domingo de los Colorados, Latacunga, Ibarra, Manta, Portoviejo, Esmeraldas y Milagro Proyecto Calidad del Aire Fase III Año Base 2010 Gobierno Nacional del Ecuador Econ. Rafael Correa Delgado Presidente de la República del Ecuador Ms. Lorena Tapia Ministra del Ambiente Abg. Juan Carlos Soria Subsecretario de Calidad Ambiental Blgo. Christian Samaniego Director Nacional de Control Ambiental Dra. Ruth Molina Chávez Equipo Técnico del Proyecto Ing. Verónica Gordillo Cueva Calidad del Aire Ecuador, 2014 Este informe presenta el resumen del documento “Inventario Nacional Preliminar de las Emisiones de Contaminantes del Aire, que incluyen las ciudades de Ambato, Riobamba, Santo Domingo de los Colorados, Latacunga, Ibarra, Manta, Portoviejo, Esmeraldas y Milagro”, documento elaborado por el Dr. René Parra Narváez, mediante contrato de consultoria suscrito con el Ministerio de Ambiente. Como parte del equipo consultor participaron: Ing. Letty Andrade Espinoza, Ing. María Gabriela Andrade, Ing. Daniela Flor Cevallos, Lizeth Vásconez Navas y Ana Dávila Gavilanez. Las siguientes personas y entidades, colaboraron en la colecta y/o entrega de información: Dra. Ruth Molina, Ministerio del Ambiente; Ing. Verónica Gordillo, Ministerio del Ambiente; Ing. Natalia Salazar, Ministerio del Ambiente - Dirección Provincial de Tungurahua; Ing. Roberto Ortega, Municipio de Ibarra; QF David Rodríguez, Municipio de Santo Domingo; Sra. Soraya Peñarrieta, Municipio de Portoviejo; Blgo. Denny Moreno, Municipio de Milagro; Ing. -

Ecuador Yellow Fever
Document is provided for sample purposes only. Content is not updated and should not be used for traveler counseling. Ecuador Yellow Fever Vaccination recommendation: Recommended for travelers aged ≥ 9 months: Esmeraldas Province and areas east of the Andes Mountains below 2,300 m (7,500 ft) (see map). Daytime insect precautions are essential for unvaccinated travelers. Generally not recommended (except for highly risk-averse travelers and long-stay travelers): itineraries limited to areas west of the Andes Mountains below 2,300 m except Guayaquil (see map). No human cases of YF have ever been reported from these areas, and data analysis by WHO indicates extremely low potential for YF virus exposure. Not recommended: itineraries limited to the cities of Guayaquil, Quito, Cuenca, or Otavalo; the Cotopaxi Volcano; areas above 2,300 m; or the Galápagos Islands. NOTE: Entry requirements may apply for this country. Please see the YF requirement statement in the Travax country profile. 83°W 81°W 79°W 77°W Galápagos Islands !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! COLOMBIA !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! 1°N Esmeraldas !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! " !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!Tulcán E !! !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!A" -
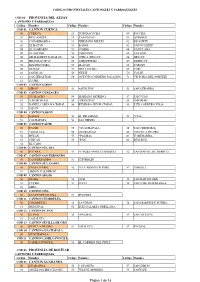
Anexo Con Codificación
CODIGOS PROVINCIALES CANTONALES Y PARROQUIALES CÓD 01 PROVINCIA DEL AZUAY CANTONES Y PARROQUIAS Código Nombre Código Nombre Código Nombre CÓD 01 CANTON CUENCA 50 CUENCA 13 TOTORACOCHA 60 PACCHA 01 BELLAVISTA 14 YANUNCAY 61 QUINGEO 02 CAÑARIBAMBA 15 HERMANO MIGUEl 62 RICAURTE 03 EL BATAN 51 BAÑOS 63 SAN JOAQUIN 04 EL SAGRARIO 52 CUMBE 64 SANTA ANA 05 EL VECINO 53 CHAUCHA 65 SAYAUSI 06 GIL RAMIREZ DAVALOS 54 CHECA (JIDCAY) 66 SIDCAY 07 HUAYNACAPAC 55 CHIQUINTAD 67 SININCAY 08 MACHANGARA 56 LLACAO 68 TARQUI 09 MONAY 57 MOLLETURO 69 TURI 10 SAN BLAS 58 NULTI 70 VALLE 11 SAN SEBASTIAN 59 OCTAVIO CORDERO PALACIOS 71 VICTORIA DEL PORTETE 12 SUCRE COD 02 CANTON GIRON 50 GIRON 51 ASUNCION 52 SAN GERARDO COD 03 CANTON GUALACEO 50 GUALACEO 54 MARIANO MORENO 57 SAN JUAN 51 *CHORDELEG 55 *PRINCIPAL 58 ZHIDMAD 52 DANIEL CORDOVA TORAL 56 REMIGIO CRESPO TORAL 59 LUIS CORDERO VEGA 53 JADAN COD 04 CANTON NABON 50 NABON 52 EL PROGRESO 54 *OÑA 51 COCHAPATA 53 LAS NIEVES COD 05 CANTON PAUTE 50 PAUTE 55 *GUACHAPALA 59 SAN CRISTOBAL 51 *AMALUZA 56 GUARAINAG 60 *SEVILLA DE ORO 52 BULAN 57 *PALMAS 61 TOMEBAMBA 53 CHICAN 58 *PAN 62 DUG DUG 54 EL CABO COD 06 CANTON PUCARA 50 PUCARA 51 *CAMILO PONCE ENRIQUEZ 52 SAN RAFAEL DE SHARUG COD 07 CANTON SAN FERNANDO 50 SAN FERNANDO 51 CHUMBLIN COD 08 CANTON STA. ISABEL 50 SANTA ISABEL 52 *EL CARMEN DE PIJILI 53 ZHAGLLI 51 ABDON CALDERON COD 09 CANTON SIGSIG 50 SIGSIG 53 GUEL 55 SAN BARTOLOME 51 CUCHIL 54 LUDO 56 SAN JOSE DE RARANGA 52 GIMA COD 10 CANTON OÑA 50 SAN FELIPE DE OÑA 51 SUSUDEL COD 11 CANTON CHORDELEG 50 CHORDELEG 52 LA UNION 54 SAN MARTIN DE PUZHIO 51 PRINCIPAL 53 LUIS GALARZA ORELLANA COD 12 CANTON EL PAN 50 EL PAN 52 *PALMAS 53 SAN VICENTE 51 *AMALUZA COD 13 CANTON SEVILLA DE ORO 50 SEVILLA DE ORO 51 AMALUZA 52 PALMAS COD 14 CANTON GUACHAPALA 50 GUACHAPALA C0D 15 CANTON CAMILO PONCE E. -

PUNTOS DE ENTREGA AGENCIAS EXPRESITO CARGA CIUDAD DIRECCIÓN TELÉFONO HORARIOS Ambato (Santiago De Ave Cevallos Y Mariano Eguez Esq C.C
Actualizacion 04 Agosto 2021 [email protected] PUNTOS DE ENTREGA AGENCIAS EXPRESITO CARGA CIUDAD DIRECCIÓN TELÉFONO HORARIOS Ambato (Santiago de Ave Cevallos y Mariano Eguez Esq C.C. Teofilo Lopez 2 y 3 Lunes a Viernes De 9:30 a 13:30 De 14:00 a 17:30 Pillaro, Pelileo, Baños) ARBOLEDA TRAVEL (03) 2829972 - 0984183230 Sábado 10:00 a 13:00 Cuenca (Cumbe, Calle Vega Muñoz 17- 42 y Miguel Heredia Lunes a Viernes 9:00 a 13:30 De 14:30 a 18:00 (07) 2838606 072825086 Girón, Gualaceo, Sta Sabado sin atencion Isabel) 0999527613 0992233451 Guayaquil Ave. de las Americas // Ciudadela Simon Bolivar MZ. 4 Edificio 57 Diagonal (04) 3726200 Lunes a Viernes 9:00 a 17:00 Aeropuerto Nuevo whatsapp 59343726200 Sábado 10:00 a 13:00 Loja (Saraguro, Pasaje Sinchona 205-53 entre Miguel Riofrio y Rocafuerte NEXO CURIER Lunes a Viernes 9:00 a 12:30 De 14:30 a 17:00 Sábado Cariamanga, (07) 2723957- 0980040107 sin atencion Catamayo) Macas Amazonas S/N y 5 de Agosto (07) 2525190 - 0984864806 Lunes a Viernes 10:00 a 13:00 De 14:00 a 16:30 (twinza-Morona) Machala 25 de Junio y Juan Montalvo (07) 2965813 - 0999868073 Lunes a Viernes 08:30 a 12:30 De 14:00 a 18:00 Manta Av. 21 # 1640 y calle 17 (Detras de metal hierro) IBC Curier Lunes a Viernes 9:00 a 12:00 De 13:00 a 18:00 (05) 2610763 - 0997829076 Sábado 8:00 a 12:00 Lunes a Viernes 8:30 a 17:30 Milagro Av. -

Tarifas De Transporte Terrestre Público De Pasajeros Interprovincial E Intraprovincial En El Ecuador
Anexo 1: Tarifas de Transporte Terrestre Público de Pasajeros Interprovincial e Intraprovincial en el Ecuador Tarifa Tarifas Provincia de Origen Cantón de Origen Ciudad / Sector Origen Provincia Destino Cantón de Destino Ciudad / Sector Destino preferencial 2021 2021 AZUAY CUENCA CUENCA AZUAY CHORDELEG CHORDELEG $ 1,27 $ 0,63 AZUAY CUENCA CUENCA AZUAY EL PAN EL PAN $ 1,61 $ 0,81 AZUAY CUENCA CUENCA AZUAY GIRÓN ASUNCIÓN $ 2,19 $ 1,09 AZUAY CUENCA CUENCA AZUAY GIRÓN BESTIÓN $ 1,32 $ 0,66 AZUAY CUENCA CUENCA AZUAY GIRÓN CALEDONEAS $ 1,32 $ 0,66 AZUAY CUENCA CUENCA AZUAY GIRÓN CHAULLA MAS RIRCAY $ 1,32 $ 0,66 AZUAY CUENCA CUENCA AZUAY GIRÓN GIRÓN $ 1,21 $ 0,60 AZUAY CUENCA CUENCA AZUAY GIRÓN LENTAG $ 1,44 $ 0,72 AZUAY CUENCA CUENCA AZUAY GIRÓN LENTAG (ESCUELA) $ 1,55 $ 0,78 AZUAY CUENCA CUENCA AZUAY GIRÓN MASTA $ 0,92 $ 0,46 AZUAY CUENCA CUENCA AZUAY GIRÓN NORAMBOTE $ 1,27 $ 0,63 AZUAY CUENCA CUENCA AZUAY GIRÓN SAN GERARDO $ 1,61 $ 0,81 AZUAY CUENCA CUENCA AZUAY GIRÓN SANTA MARIANITA $ 0,98 $ 0,49 AZUAY CUENCA CUENCA AZUAY GIRÓN ZAPATA $ 0,92 $ 0,46 AZUAY CUENCA CUENCA AZUAY GUACHAPALA GUACHAPALA $ 1,27 $ 0,63 AZUAY CUENCA CUENCA AZUAY GUALACEO CHICTICAY $ 0,69 $ 0,35 AZUAY CUENCA CUENCA AZUAY GUALACEO GUALACEO $ 1,27 $ 0,63 AZUAY CUENCA CUENCA AZUAY GUALACEO JADAN $ 1,09 $ 0,55 AZUAY CUENCA CUENCA AZUAY GUALACEO ZHIDMAD $ 0,75 $ 0,37 AZUAY CUENCA CUENCA AZUAY NABÓN COCHAPATA $ 2,59 $ 1,29 AZUAY CUENCA CUENCA AZUAY NABÓN HERMANO MIGUEL $ 1,67 $ 0,83 AZUAY CUENCA CUENCA AZUAY NABÓN NABÓN $ 2,24 $ 1,12 AZUAY CUENCA CUENCA AZUAY NABÓN ZHIÑA -

Sanitation Service By
Document of The World Bank FOR OFFICIAL USE ONLY Public Disclosure Authorized Report No: 36579-EC PROJECT APPRAISAL DOCUMENT ON A Public Disclosure Authorized PROPOSED ADAPTABLE PROGRAM LOAN (APL-2) IN THE AMOUNT OF US$48 MILLION TO THE REPUBLIC OF ECUADOR FOR THE SECOND RURAL AND SMALL TOWNS WATER SUPPLY AND SANITATION PROJECT Public Disclosure Authorized (PRAGUAS 11) IN SUPPORT OF THE SECOND PHASE OF THE RURAL AND SMALL TOWNS WATER SUPPLY AND SANITATION PROGRAM June 23.2006 Finance, Private Sector, and Infrastructure Bolivia, Ecuador, Peru and Venezuela Country Management Unit Latin America and the Caribbean Region This document has a restricted distribution and may be used by recipients only in the Public Disclosure Authorized performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS Currency Unit = US Dollar FISCAL YEAR January 1 - December 31 ABBREVIATIONS AND ACRONYMS APL Adaptable Program Loan BCE Central Bank of Ecuador (Banco Central del Ecuador) BdE State Development Bank of Ecuador (Banco del Estado) BOT Build, operate and transfer contract CADS Consultancy to support the delegation of water, sanitation and/or solid waste services (Consultorias de apoyo a la delegacidn) CAS Country Assistance Strategy CGE General Controller's Office (Contraloria General del Estado) CNRH National Council on Water Resources (Consejo Nacional de Recursos Hidricos) CODAE Afro-Ecuadorian Development Corporation (Corporacidn de Desarrollo Afroecuatoriana) CODENPE Ecuadorian -

Codigo Descripcion Del Distrito Sede Codigo
PROVINCIAS QUE LA DIRECCIONES DISTRITALES OFICNAS DISTRITALES COMPONEN ZONA DE PLANIFICACION SEDE ZONAL CODIGO DESCRIPCION DEL DISTRITO SEDE CODIGO DESCRIPCION DEL DISTRITO SEDE 04D02 MONTUFAR - BOLÍVAR MONTUFAR CARCHI 04D01 SAN PEDRO DE HUACA - TULCAN TULCAN 04D03 ESPEJO -MIRA ESPEJO 08D03 MUISNE - ATACAMES ATACAMES 08D01 ESMERALDAS ESMERALDAS 08D04 QUININDE QUININDE ESMERALDAS 08D02 ELOY ALFARO ELOY ALFARO 08D05 SAN LORENZO SAN LORENZO 08D06 RIOVERDE RIOVERDE COORDINACION ZONAL 1 IBARRA IBARRA- PIMAMPIRO -SAN MIGUEL DE 10D02 ANTONIO ANTE -OTAVALO OTAVALO IMBABURA 10D01 IBARRA URCUQUI 10D03 COTACACHI COTACACHI 21D01 CÁSCALES - GONZALO PIZARRO - SUCUMBÍOS SUCUMBIOS SUCUMBÍOS 21D02 LAGO AGRIO LAGO AGRIO 21D03 CUYABENO - PUTUMAYO PUTUMAYO 21D04 SHUSHUFINDI SHUSHUFINDI ARCHIDONA - CARLOS JULIO AROSEMENA NAPO TENA 15D02 EL CHACO QUIJOS QUIJOS 15D01 TOLA - TENA 17D10 CAYAMBE - PEDRO MONCAYO CAYAMBE PICHINCHA 17D11 MEJIA - RUMINAHUI RUMIÑAHUI PEDRO VICENTE MALDONADO - PUERTO QUITO - SAN MIGUEL DE LOS COORDINACION ZONAL 2 TENA 17D12 SAN MIGUEL DE LOS BANCOS BANCOS 22D01 LA JOYA DE LOS SACHAS LA JOYA DE LOS SACHAS ORELLANA 22D02 LORETO- ORELLANA ORELLANA 22D03 AGUARICO AGUARICO 05D02 LA MANA LA MANA 05D03 PANGUA PANGUA COTOPAXI 05D01 LATACUNGA LATACUNGA 05D04 PUJILI-SAQUISILI PUJILI 05D05 SIGCHOS SIGCHOS 05D06 SALCEDO SALCEDO 06D02 ALAUSI - CHUNCHI ALAUSI 06D03 CUMANDA - PALLATANGA PALLATANGA CHIMBORAZO 06D01 CHAMBO - RIOBAMBA RIOBAMBA 06D04 COLTA - GUAMOTE GUAMOTE 06D05 GUANO - PENIPE GUANO COORDINACION ZONAL 3 AMBATO PASTAZA 16D01 PASTAZA - MERA - SANTA CLARA PASTAZA 16D02 ARAJUNO ARAJUNO COORDINACION ZONAL 3 AMBATO AMBATO: HUACHI GRANDE, JUAN BENIGNO VELA, MONTALVO, PICAIGUA, PILAHUIN, SANTA 18D02 AMBATO AMBATO: LA PENÍNSULA - LA MERCED - ROSA, TOTORAS, CELIANO MONGE, HUACHI ATOCHA FICOA - LA MATRIZ - SAN CHICO, HUACHI LORETO, PISHILATA FRANCISCO - AUGUSTO N. -
Manabí, Ecuador a Guide To
A GUIDE TO MANABÍ, ECUADOR The coastal province of Manabí is a gem among Ecuador’s natural treasures. As a traveler here, you can experience its pristine beaches, mouthwatering local dishes and rich biodiversity, both on land and below water. Read on to discover the Wanderbus team’s tips to some of the best destinations to explore in Manabí from Ayampe to Cojimies. Don’t forget your sunblock! A Guide to Manabí, Ecuador OVERVIEW Located between the provinces of Esmeraldas and hiking,horseback riding, and even a dip in a natural Santa Elena, Manabí is one of the most beautiful mud bath. However, if you prefer to base out of segments along the Ecuadorian coast. It’s main cities a larger town with more restaurants, hostels and are Manta and Portoviejo, followed by Pedernales, El nightlife, you’ll find that in Manta, Puerto Lopez Carmen and Chone. and Canoa. Manabí is best known for its gorgeous, often isolated A great way to explore this province is to follow the beaches, and is a sought after destination for both Spondylus Route (Ruta del Spondylus), which begins local and international visitors. It’s one of the in the northern province of Esmeraldas, passes along warmest regions in Ecuador and the area along the Manabí’s coast, stopping at some of its top beach coast is known for its dry forests that are teeming destinations, and ends near Salinas, in with wildlife. the province of Santa Elena. Within Manabí, the most visited locations are located Whether you travel by public in and around Machalilla National Park, including transport, the Wanderbus or a the islands Isla de la Plata and Isla Salango. -

EARTHQUAKE in ECUADOR Situation Report No
EARTHQUAKE IN ECUADOR Situation Report No. April 4-21, 2016 KEY INFORMATION Seven hospitals operated by the Ministry of Public Health (MSP) and the Ecuadorian Social Security Institute (IESS) have severely damaged infrastructure and are not operational. Health personnel in the provinces of Manabí and Esmeraldas are also affected, including some deaths. Others lost family members and homes. There is potential risk of water-, vector-, and food-borne diseases due to limited drinking water and sanitation services, rubble and debris, and lack of proper shelter among people who have lost their homes. 7015 155 24,442 570 24 INJURED MISSING IN AFFECTED SHELTERS DEAD HEALTH FACILITIES Source: Risk Management Department, April 20, 2016, 7:30 p.m. Ministry of Public Health, April 20, 2016 HEALTH SITUATION Status of Health Services Network According to the preliminary assessment, the earthquake has affected the infrastructure of at least 24 MSP and IESS health facilities (14 health centers and 10 hospitals) in the provinces of Manabí and Esmeraldas. Seven (7) of the 10 hospitals and six of the 14 health centers that report damage are out of service. Another three health facilities are not operating despite suffering less damage, due to a lack of personnel, some of whom are afraid to return to work. Centro de Operaciones de Emergencia de la Organización Panamericana de la Salud www.paho.org/desastres 1 Table 1. Reported status of health facility infrastructure TIPO DE PROVINCIA CANTON NOMBRE DEL ESTABLECIMIENTO INSTITUCION DAÑO PROBABLE CONDICION -

Dpa Cpv 2010
División política administrativa del Ecuador Código Código Código Nombre de la Nombre del Nombre de la Parroquia Provincia Cantón Parroquia Provincia Cantón 01 01 50 AZUAY CUENCA CUENCA 01 01 51 AZUAY CUENCA BAÑOS 01 01 52 AZUAY CUENCA CUMBE 01 01 53 AZUAY CUENCA CHAUCHA 01 01 54 AZUAY CUENCA CHECA (JIDCAY) 01 01 55 AZUAY CUENCA CHIQUINTAD 01 01 56 AZUAY CUENCA LLACAO 01 01 57 AZUAY CUENCA MOLLETURO 01 01 58 AZUAY CUENCA NULTI 01 01 59 AZUAY CUENCA OCTAVIO CORDERO PALACIOS (SANTA ROSA) 01 01 60 AZUAY CUENCA PACCHA 01 01 61 AZUAY CUENCA QUINGEO 01 01 62 AZUAY CUENCA RICAURTE 01 01 63 AZUAY CUENCA SAN JOAQUIN 01 01 64 AZUAY CUENCA SANTA ANA 01 01 65 AZUAY CUENCA SAYAUSI 01 01 66 AZUAY CUENCA SIDCAY 01 01 67 AZUAY CUENCA SININCAY 01 01 68 AZUAY CUENCA TARQUI 01 01 69 AZUAY CUENCA TURI 01 01 70 AZUAY CUENCA VALLE 01 01 71 AZUAY CUENCA VICTORIA DEL PORTETE (IRQUIS) 01 02 50 AZUAY GIRON GIRON 01 02 51 AZUAY GIRON ASUNCION 01 02 52 AZUAY GIRON SAN GERARDO 01 03 50 AZUAY GUALACEO GUALACEO 01 03 52 AZUAY GUALACEO DANIEL CORDOVA TORAL (EL ORIENTE) 01 03 53 AZUAY GUALACEO JADAN 01 03 54 AZUAY GUALACEO MARIANO MORENO 01 03 56 AZUAY GUALACEO REMIGIO CRESPO TORAL (GULAG) 01 03 57 AZUAY GUALACEO SAN JUAN 01 03 58 AZUAY GUALACEO ZHIDMAD 01 03 59 AZUAY GUALACEO LUIS CORDERO VEGA 01 03 60 AZUAY GUALACEO SIMON BOLIVAR (CAB. EN GAÑANZOL) 01 04 50 AZUAY NABON NABON 01 04 51 AZUAY NABON COCHAPATA 01 04 52 AZUAY NABON EL PROGRESO (CAB.EN ZHOTA) 01 04 53 AZUAY NABON LAS NIEVES (CHAYA) 01 05 50 AZUAY PAUTE PAUTE 01 05 52 AZUAY PAUTE BULAN (JOSE VICTOR IZQUIERDO)