Non-Commercial Use Only
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Page 1 C H a D N I G E R N I G E R I a G a B O N CENTRAL AFRICAN
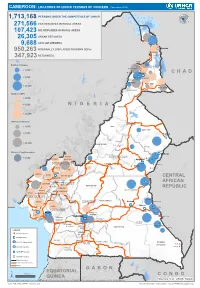
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (November 2019) 1,713,168 PERSONS UNDER THE COMPETENCENIGER OF UNHCR 271,566 CAR REFUGEES IN RURAL AREAS 107,423 NIG REFUGEES IN RURAL AREAS 26,305 URBAN REFUGEES 9,688 ASYLUM SEEKERS 950,263 INTERNALLY DISPLACED PERSONS (IDPs) Kousseri LOGONE 347,923 RETURNEES ET CHARI Waza Limani Magdeme Number of refugees EXTRÊME-NORD MAYO SAVA < 3,000 Mora Mokolo Maroua CHAD > 5,000 Minawao DIAMARÉ MAYO TSANAGA MAYO KANI > 20,000 MAYO DANAY MAYO LOUTI Number of IDPs < 2,000 > 5,000 NIGERIA BÉNOUÉ > 20,000 Number of returnees NORD < 2,000 FARO MAYO REY > 5,000 Touboro > 20,000 FARO ET DÉO Beke chantier Ndip Beka VINA Number of asylum seekers Djohong DONGA < 5,000 ADAMAOUA Borgop MENCHUM MANTUNG Meiganga Ngam NORD-OUEST MAYO BANYO DJEREM Alhamdou MBÉRÉ BOYO Gbatoua BUI Kounde MEZAM MANYU MOMO NGO KETUNJIA CENTRAL Bamenda NOUN BAMBOUTOS AFRICAN LEBIALEM OUEST Gado Badzere MIFI MBAM ET KIM MENOUA KOUNG KHI REPUBLIC LOM ET DJEREM KOUPÉ HAUTS PLATEAUX NDIAN MANENGOUBA HAUT NKAM SUD-OUEST NDÉ Timangolo MOUNGO MBAM ET HAUTE SANAGA MEME Bertoua Mbombe Pana INOUBOU CENTRE Batouri NKAM Sandji Mbile Buéa LITTORAL KADEY Douala LEKIÉ MEFOU ET Lolo FAKO AFAMBA YAOUNDE Mbombate Yola SANAGA WOURI NYONG ET MARITIME MFOUMOU MFOUNDI NYONG EST Ngarissingo ET KÉLLÉ MEFOU ET HAUT NYONG AKONO Mboy LEGEND Refugee location NYONG ET SO’O Refugee Camp OCÉAN MVILA UNHCR Representation DJA ET LOBO BOUMBA Bela SUD ET NGOKO Libongo UNHCR Sub-Office VALLÉE DU NTEM UNHCR Field Office UNHCR Field Unit Region boundary Departement boundary Roads GABON EQUATORIAL 100 Km CONGO ± GUINEA The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Sources: Esri, USGS, NOAA Source: IOM, OCHA, UNHCR – Novembre 2019 Pour plus d’information, veuillez contacter Jean Luc KRAMO ([email protected]). -

A History of Leprosy and Coercion in Hawai’I
THE PURSE SEINE AND EURYDICE: A HISTORY OF LEPROSY AND COERCION IN HAWAI’I A THESIS SUBMITTED TO THE GRADUATE DIVISION OF THE UNIVERSITY OF HAWAIʻI AT MĀNOA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF ARTS IN ANTHROPOLOGY DECEMBER 2012 By David James Ritter Thesis Committee: Chairperson Eirik Saethre Geoffrey White Noelani Arista Keywords: Leprosy, Capitalism, Hansen’s Disease, Hawaiʻi, Molokaʻi, Kalaupapa, Political Economy, Medical Anthropology Acknowledgements I would like to extend my sincere gratitude to a number of individuals without whom this research would not have been possible. First, I would like to thank each of my committee members- Eirik Saethre, Geoff White, and Noelani Arista- for consistently finding time and energy to commit to my project. I would like to thank the staff and curators of the Asia Pacific collection at the Hamilton Library for their expertise University of Hawai`i at Mānoa. I would also like to thank my friend and office mate Aashish Hemrajani for consistently providing thought provoking conversation and excellent reading suggestions, both of which have in no small way influenced this thesis. Finally, I would like to extend my greatest gratitude to my parents, whose investment in me over the course this thesis project is nothing short of extraordinary. ii Abstract In 1865, the Hawai`i Board of Health adopted quarantine as the primary means to arrest the spread of leprosy in the Kingdom of Hawai`i. In Practice, preventing infection entailed the dramatic expansion of medical authority during the 19th century and included the establishment of state surveillance networks, the condemnation by physicians of a number of Hawaiian practices thought to spread disease, and the forced internment of mainly culturally Hawaiian individuals. -
CAMEROON Situation Report Last Updated: 8 Oct 2020
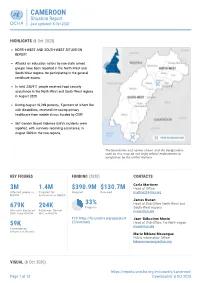
CAMEROON Situation Report Last updated: 8 Oct 2020 HIGHLIGHTS (8 Oct 2020) NORTH-WEST AND SOUTH-WEST SITUATION REPORT Attacks on education actors by non-state armed groups have been reported in the North-West and South-West regions for participating in the general certificate exams. In total 245,911 people received food security assistance in the North-West and South-West regions in August 2020. During August 10,249 patients, 5 percent of whom live with disabilities, received life-saving primary healthcare from mobile clinics funded by CERF. 567 Gender Based Violence (GBV) incidents were reported, with survivors receiving assistance, in August 2020 in the two regions. The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations. KEY FIGURES FUNDING (2020) CONTACTS Carla Martinez 3M 1.4M $390.9M $130.7M Head of Office Affected people in Targeted for Required Received [email protected] NWSW assistance in NWSW ! j e r d n , A y James Nunan r r o S 33% Head of Sub-Office North-West and 679K 204K Progress South-West regions Internally displaced Returnees (former [email protected] (IDP) from NWSW IDP) in NWSW FTS: https://fts.unocha.org/appeals/9 Jean-Sébastien Munie 27/summary Head of Sub-Office, Far-North region 59K [email protected] Cameroonian refugees in Nigeria Marie Bibiane Mouangue Public information Officer [email protected] VISUAL (8 Oct 2020) https://reports.unocha.org/en/country/cameroon/ Page 1 of 13 Downloaded: 8 Oct 2020 CAMEROON Situation Report Last updated: 8 Oct 2020 Map of IDP, Returnees and Refugees from the North-West and South-West Regions of Cameroon Source: OCHA, UNHCR, IOM The boundaries and names shown, and the designations used on this map do not imply official endorsement or acceptance by the United Nations. -

A Descriptive Study from Patients' Perspective in Sri Lanka
Scientific Research Journal (SCIRJ), Volume V, Issue IX, September 2017 10 ISSN 2201-2796 Stigmatization in Leprosy: A descriptive study from patients’ perspective in Sri Lanka M.A.J.D. Mallawa Arachchi, A.G.D. Kumari Leprosy Hospital Hendala, Sri Lanka R. Wickramasinghe Dept. of Basic Sciences The Open University of Sri Lanka Nawala, Nugegoda [email protected] N.R. Kuruppu, A.V. Pramuditha Madhavi Dept. of Nursing The Open University of Sri Lanka Nawala, Nugegoda [email protected], [email protected] Abstract- The stigma of leprosy is a real phenomenon in many period from year 2000 to 2013. Six new leprosy patients are people’s lives that affects their physical, psychological, social and being detected in Sri Lanka daily [4]. economic well-being. The objective of the study is to investigate People with leprosy and related deformities suffer from the stigma in leprosy from patient’s perspective. Further this social stigma and discrimination leading to economic loss [5]. study help to determine how stigmatization affect the social life of Stigma is not a single phenomenon and can be define as “an patients with leprosy, how stigmatization affect the psychological aspect of patient’s life and identify the coping mechanisms attribute that is deeply discrediting, and the stigmatized employed by patients to manage the stigma. This study was individual is one who is not accepted and is not accorded the conducted in the central leprosy clinic in National Hospital in Sri respect and regard of his peers; one who is disqualified from Lanka. The data were collected from hundred and thirty two full social acceptance” [8]. -

Interrogating Leprosy 'Stigma'
Lepr Rev (2011) 82, 91–97 EDITORIAL Interrogating leprosy ‘stigma’: why qualitative insights are vital JAMES STAPLES Brunel University, Uxbridge, Middlesex UB8 3PH Accepted for publication 24 April 2011 I was initially in two minds about editing a special issue on ‘stigma’. The term, it seemed to me, was one too often applied uncritically to bodily conditions – especially in relation to leprosy – as a vague gloss for a qualitatively diverse range of negative social reactions and attitudes, as well as a description of how they might be experienced. As such, ‘stigma’ can become a lazy shortcut for the multiple ‘social aspects’ of leprosy, preventing deeper scrutiny of the complex and sometimes contradictory experiences that are characteristic of living with the disease. At the same time, however, devoting a special issue to the topic also offers a valuable opportunity to address precisely those issues: to interrogate how, if at all, ‘stigma’ might remain a conceptually useful notion through which to analyse the experience of those whose lives are touched by leprosy, whether as sufferers, family members or those working in the leprosy field. It also provides a chance to showcase alternative approaches to understanding attitudes towards the disease that go beyond the conventional, taken for granted wisdom which states, a) that leprosy is a uniformly stigmatised disease, and b) that education about its causes and treatments is necessarily the appropriate response to managing that stigma. A critical focus on stigma allows us to ask, for example, questions about the socio-cultural, historical, economic and political contexts in which stigma is produced. -

Shelter Cluster Dashboard NWSW052021
Shelter Cluster NW/SW Cameroon Key Figures Individuals Partners Subdivisions Cameroon 03 23,143 assisted 05 Individual Reached Trend Nigeria Furu Awa Ako Misaje Fungom DONGA MANTUNG MENCHUM Nkambe Bum NORD-OUEST Menchum Nwa Valley Wum Ndu Fundong Noni 11% BOYO Nkum Bafut Njinikom Oku Kumbo Belo BUI Mbven of yearly Target Njikwa Akwaya Jakiri MEZAM Babessi Tubah Reached MOMO Mbeggwi Ngie Bamenda 2 Bamenda 3 Ndop Widikum Bamenda 1 Menka NGO KETUNJIA Bali Balikumbat MANYU Santa Batibo Wabane Eyumodjock Upper Bayang LEBIALEM Mamfé Alou OUEST Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Fontem Nguti KOUPÉ HNO/HRP 2021 (NW/SW Regions) Toko MANENGOUBA Bangem Mundemba SUD-OUEST NDIAN Konye Tombel 1,351,318 Isangele Dikome value Kumba 2 Ekondo Titi Kombo Kombo PEOPLE OF CONCERN Abedimo Etindi MEME Number of PoC Reached per Subdivision Idabato Kumba 1 Bamuso 1 - 100 Kumba 3 101 - 2,000 LITTORAL 2,001 - 13,000 785,091 Mbongé Muyuka PEOPLE IN NEED West Coast Buéa FAKO Tiko Limbé 2 Limbé 1 221,642 Limbé 3 [ Kilometers PEOPLE TARGETED 0 15 30 *Note : Sources: HNO 2021 PiN includes IDP, Returnees and Host Communi�es The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Key Achievement Indicators PoC Reached - AGD Breakdouwn 296 # of Households assisted with Children 27% 26% emergency shelter 1,480 Adults 21% 22% # of households assisted with core 3,769 Elderly 2% 2% relief items including prevention of COVID-19 21,618 female male 41 # of households assisted with cash for rental subsidies 41 Households Reached Individuals Reached Cartegories of beneficiaries reported People Reached by region Distribution of Shelter NFI kits integrated with COVID 19 KITS in Matoh town. -

CMR-3W-Cash-Transfer-Partners V3.4
CAMEROON: 3W Operational Presence - Cash Programming [as of December 2016] Organizations working for cash 10 programs in Cameroon Organizations working in Organizations by Cluster Food security 5 International NGO 5 Multi-Sector cash 5 Government 2 Economic Recovery 3 Red Cross & Red /Livelihood 2 Crescent Movement Nutrition 1 UN Agency 1 WASH 1 Number of organizations Multi-Sector Cash by departments 15 5 distinct organizations 9 organizations conducting only emergency programs 1 organizations conducting only regular programs Number of organizations by departments 15 Economic Recovery/Livelihood Food security 3 distinct organizations 5 distinct organizations Number of organizations Number of organizations by department by department 15 15 Nutrition WASH 3 distinct organizations 1 organization Number of organizations Number of organizations by department by department 15 15 Creation: December 2016 Sources: Cash Working group, UNOCHA and NGOs More information: https://www.humanitarianresponse.info/en/operations/cameroon/cash )HHGEDFNRFKDFDPHURRQ#XQRUJ 7KHERXQGDULHVDQGQDPHVVKRZQDQGWKHGHVLJQDWLRQVXVHGRQWKLVPDSGRQRWLPSO\RI̙FLDOHQGRUVHPHQWRUDFFHSWDQFHE\WKH8QLWHG1DWLRQV CAMEROON:CAMEROON: 3W Operational Presence - Cash Programming [as of December 2016] ADAMAOUA FAR NORTH NORTH 4 distinct organizations 9 distinct organizations 1 organization DJEREM DIAMARE FARO MINJEC CRF MINEPAT CRS IRC MAYO-BANYO LOGONE-ET-CHARI MAYO-LOUTI MINEPAT MINEPAT WFP, PLAN CICR MMBERE MAYO-REY PLAN PUI MINEPAT CENTRE MAYO-DANAY 1 organization MINEPAT LITTORAL 1 organization -

From Migrants to Nationals, from Nationals To
International Journal of Latest Engineering and Management Research (IJLEMR) ISSN: 2455-4847 www.ijlemr.com || Volume 03 - Issue 06 || June 2018 || PP. 10-19 From Nomads to Nationals, From Nationals to Undesirable Elements: The Case of the Mbororo/Fulani in North West Cameroon 1916-2008 A Historical Investigation Jabiru Muhammadou Amadou (Phd) Higher Teacher Training College Department of History The University of Yaounde 1 Abstract: The Fulani (Mbororo) are a minority group perceived as migrants and strangers by local North West groups who consider themselves their hosts and landlords. They are predominantly nomadic people located almost exclusively within the savannah zone of West and Central Africa. Their original homeland is said to be the Senegambia region. From Senegal, the Fulani continued their movement along side their cattle and headed to Northern Nigeria. Uthman Dan Fodio‟s 19th century jihad movement and epidemic outbreaks force them to move from Northern Nigeria to Northern Cameroon. From Northern Cameroon they moved down South and started penetrating the North West Region in the early 20th century. This article critically examines and considers the case of the Fulani in the North West Region of Cameroon and their recent claims to regional citizenship and minority status. The paper begins by presenting the migration, settlement and ultimate acquisition of the status of nationals by the nomadic cattle Fulani in North West Cameroon. It also analysis the difficulties encountered by this nomadic group to fully integrate themselves into the region. In the early 20th century (more precisely 1916) when they arrived the North West Region, they were warmly received by their hosts. -

Cameroon:NW/SW Highlights Needs 690K 414K 63K1 52 $9.5M
Cameroon:NW/SW WASH Update April 2020 Hand washing sensitization of community members in the North West region. Photo by NRC Highlights Needs In order to contain the spread of COVID-19, WASH partners have scaled up community 690k People in need of WASH engagement activities. More than 116,000 services in NW/SW people were reached through COVID 19 sensitization sessions in April. 414k In response to the COVID 19 pandemic, Targeted ReachOut, with support from UNICEF, 1 installed 250 communal hand washing 63k IDPs & Returnees stations in Ekondo Titi. More than 12,500 people are expected to benefit. 52 More than 10,000 individuals received WASH partners WASH and hygiene kits from WASH partners in April. $9.5m In April, about 1,600 people benefitted from required for WASH improved water supply as a result of US$9.5M installation of water distribution systems by WASH partners. Reguired WASH partners provided improved sanitation facilities to 400 people. US$0.2M Funded 1 IDP Tracking Database, May 2020 (Note: This figure is the latest displacement figure as of 16 May 2020) Website: https://www.humanitarianresponse.info/en/operations/cameroon/water-sanitation-hygiene For more information contact Wash Cluster Coordinator: Nchunguye Festo Vyagusa Email: [email protected] WATER Plan International, in collaboration with UNICEF completed rehabilitation of a water distribution system in Fundong, Boyo division, reaching 1,650 individuals with safe drinking water. Rehabilitation of water systems in Bamenda 2 subdivision in Mezam is ongoing. Plan International, supported by UNICEF is planning to rehabilitate two water distribution systems in Babessi sub-division of Ngo- Ketunjia division in May. -

N I G E R I a C H a D Central African Republic Congo
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (September 2020) ! PERSONNES RELEVANT DE Maïné-Soroa !Magaria LA COMPETENCE DU HCR (POCs) Geidam 1,951,731 Gashua ! ! CAR REFUGEES ING CurAi MEROON 306,113 ! LOGONE NIG REFUGEES IN CAMEROON ET CHARI !Hadejia 116,409 Jakusko ! U R B A N R E F U G E E S (CENTRAL AFRICAN REPUBLIC AND 27,173 NIGERIAN REFUGEE LIVING IN URBAN AREA ARE INCLUDED) Kousseri N'Djamena !Kano ASYLUM SEEKERS 9,332 Damaturu Maiduguri Potiskum 1,032,942 INTERNALLY DISPLACED PERSO! NS (IDPs) * RETURNEES * Waza 484,036 Waza Limani Magdeme Number of refugees MAYO SAVA Mora ! < 10,000 EXTRÊME-NORD Mokolo DIAMARÉ Biu < 50,000 ! Maroua ! Minawao MAYO Bauchi TSANAGA Yagoua ! Gom! be Mubi ! MAYO KANI !Deba MAYO DANAY < 75000 Kaele MAYO LOUTI !Jos Guider Number! of IDPs N I G E R I A Lafia !Ləre ! < 10,000 ! Yola < 50,000 ! BÉNOUÉ C H A D Jalingo > 75000 ! NORD Moundou Number of returnees ! !Lafia Poli Tchollire < 10,000 ! FARO MAYO REY < 50,000 Wukari ! ! Touboro !Makurdi Beke Chantier > 75000 FARO ET DÉO Tingere ! Beka Paoua Number of asylum seekers Ndip VINA < 10,000 Bocaranga ! ! Borgop Djohong Banyo ADAMAOUA Kounde NORD-OUEST Nkambe Ngam MENCHUM DJEREM Meiganga DONGA MANTUNG MAYO BANYO Tibati Gbatoua Wum BOYO MBÉRÉ Alhamdou !Bozoum Fundong Kumbo BUI CENTRAL Mbengwi MEZAM Ndop MOMO AFRICAN NGO Bamenda KETUNJIA OUEST MANYU Foumban REPUBLBICaoro BAMBOUTOS ! LEBIALEM Gado Mbouda NOUN Yoko Mamfe Dschang MIFI Bandjoun MBAM ET KIM LOM ET DJEREM Baham MENOUA KOUNG KHI KOUPÉ Bafang MANENGOUBA Bangangte Bangem HAUT NKAM Calabar NDÉ SUD-OUEST -

Disability-Related Stigma and Discrimination in Sub-Saharan Africa and South Asia: a Systematic Literature Review May 2021
Disability-related stigma and discrimination in sub-Saharan Africa and south Asia: a systematic literature review May 2021 Report authors: Bhavisha Virendrakumar Cathy Stephen Emma Jolley Elena Schmidt Study contributors: Vladimir Pente Elizabeth Clery Acknowledgement: We would like to thank Irish Aid for the funding provided for this review. Many thanks to the systematic review Steering Committee, who provided valuable comments on the protocol and draft report. Recommended citation: Sightsavers. Disability-related stigma and discrimination in sub-Saharan Africa and South Asia: a systematic literature review. Haywards Heath, UK: Sightsavers, 2021. 2 Disability-related stigma and discrimination in sub-Saharan Africa and South Asia: a systematic literature review | May 2021 Contents Executive summary .............................................................................................................. 6 Introduction ........................................................................................................................ 6 Methods ............................................................................................................................. 7 Results ............................................................................................................................... 7 Characteristics of included studies ................................................................................. 7 Factors leading to stigma and discrimination ................................................................ -

Masculinity and Female Resistance in the Rice Economy in Meteh/Menchum Valley Bu, North West Cameroon, 1953 – 2005
Journal of Sustainable Development in Africa (Volume 15, No.7, 2013) ISSN: 1520-5509 Clarion University of Pennsylvania, Clarion, Pennsylvania MASCULINITY AND FEMALE RESISTANCE IN THE RICE ECONOMY IN METEH/MENCHUM VALLEY BU, NORTH WEST CAMEROON, 1953 – 2005 Henry Kam Kah University of Buea, Cameroon ABSTRACT Male chauvinism and female reaction in the rice economy in Bu, Menchum Division of North West Cameroon is the subject of this investigation. The greater focus of this paper is how and why this phobia has lessened over the years in favour of female dominion over the rice economy. The point d’appui of the masculine management of the economy and the accentuating forces which have militated against their continuous domination of women in the rice sector have been probed into. Incongruous with the situation hitherto, women have farms of their own bought with their own money accumulated from other economic activities. In addition, they now employ the services of men to execute some defined tasks in the rice economy. From the copious data consulted on the rice economy and related economic endeavours, it is a truism that be it collectively and/or individually, men and women in Bu are responding willingly or not, to the changing power relations between them in the rice economy with implications for sustainable development. Keywords: Masculinity, Female Resistance, Rice Economy, Cameroon, Sustainability 115 INTRODUCTION: RELEVANCE OF STUDY AND CONCEPT OF MASCULINITY Rice is a staple food crop in Cameroon like elsewhere in Africa and other parts of the world. It has become increasingly important part of African diets especially West Africa and where local production has been insufficient due to limited access to credit (Akinbode, 2013, p.