Boards' Fodder
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Skin Lesions in Diabetic Patients
Rev Saúde Pública 2005;39(4) 1 www.fsp.usp.br/rsp Skin lesions in diabetic patients N T Foss, D P Polon, M H Takada, M C Foss-Freitas and M C Foss Departamento de Clínica Médica. Faculdade de Medicina de Ribeirão Preto. Universidade de São Paulo. Ribeirão Preto, SP, Brasil Keywords Abstract Skin diseases. Dermatomycoses. Diabetes mellitus. Metabolic control. Objective It is yet unknown the relationship between diabetes and determinants or triggering factors of skin lesions in diabetic patients. The purpose of the present study was to investigate the presence of unreported skin lesions in diabetic patients and their relationship with metabolic control of diabetes. Methods A total of 403 diabetic patients, 31% type 1 and 69% type 2, underwent dermatological examination in an outpatient clinic of a university hospital. The endocrine-metabolic evaluation was carried out by an endocrinologist followed by the dermatological evaluation by a dermatologist. The metabolic control of 136 patients was evaluated using glycated hemoglobin. Results High number of dermophytosis (82.6%) followed by different types of skin lesions such as acne and actinic degeneration (66.7%), pyoderma (5%), cutaneous tumors (3%) and necrobiosis lipoidic (1%) were found. Among the most common skin lesions in diabetic patients, confirmed by histopathology, there were seen necrobiosis lipoidic (2 cases, 0.4%), diabetic dermopathy (5 cases, 1.2%) and foot ulcerations (3 cases, 0.7%). Glycated hemoglobin was 7.2% in both type 1 and 2 patients with adequate metabolic control and 11.9% and 12.7% in type 1 and 2 diabetic patients, respectively, with inadequate metabolic controls. -

Training Available: in 2012, Lorenzo Kunze, M.E
2013 Derma-Lo - offers the 2013 Thermo-Lo - offers the reduction of: sun/age spot, milia, reduction of: sun/age spot, milia, telangiectasia / epidermal spider telangiectasia / epidermal spider veins, cherry hemangiomas, veins, cherry hemangiomas and Thermolysis (AC) and Electrolysis Thermolysis (AC) hair removal. (DC) hair removal. Also: active acne, acne scarring, sebaceous hyperplasia, and skin tags. Training Available: In 2012, Lorenzo Kunze, M.E. Includes: Hydro-Lo - treatment IN DENVER ONCE A MONTH developed Chromos, Inc. - which of fine lines and wrinkles, TRAINING AVAILABLE AT in Greek, can be interpreted as enlarged pore reduction, boosts YOUR LOCATION ASK ABOUT “color” or “light” – in essence, the penetration of product into COST without light we have no color. the skin and tightens loose skin. “Dedicated to Excellence” Also: select your choice of (1 of Continuing to provide a professional & positive attitude in the medical 2) LED’s – both are non invasive and aesthetic field. hand-held light probes: BLUE for CHROMOS, Inc. the treatment of acne or Lorenzo Kunze, M.E. Chromos strives to be a guiding INFRARED to increase collagen [email protected] “light” that assists medical and and elastin, Rosacea, increased www.DermaLo.com aesthetic professionals in finding healing properties, minor muscle www.Thermo-Lo.com and pursuing proper education and moderate joint pain. 888-499-8991 / 303-994-7236 and accurate knowledge. Lorenzo Kunze, M.E. Lorenzo is a true visionary - 40 years in the medical and aesthetic field Medical Electrologist / medical educator 1st non-medical professional to provide electrolysis treatments in an OR Treated over 20,000 patients - last 16 years 1st in the U.S. -

Dermatology DDX Deck, 2Nd Edition 65
63. Herpes simplex (cold sores, fever blisters) PREMALIGNANT AND MALIGNANT NON- 64. Varicella (chicken pox) MELANOMA SKIN TUMORS Dermatology DDX Deck, 2nd Edition 65. Herpes zoster (shingles) 126. Basal cell carcinoma 66. Hand, foot, and mouth disease 127. Actinic keratosis TOPICAL THERAPY 128. Squamous cell carcinoma 1. Basic principles of treatment FUNGAL INFECTIONS 129. Bowen disease 2. Topical corticosteroids 67. Candidiasis (moniliasis) 130. Leukoplakia 68. Candidal balanitis 131. Cutaneous T-cell lymphoma ECZEMA 69. Candidiasis (diaper dermatitis) 132. Paget disease of the breast 3. Acute eczematous inflammation 70. Candidiasis of large skin folds (candidal 133. Extramammary Paget disease 4. Rhus dermatitis (poison ivy, poison oak, intertrigo) 134. Cutaneous metastasis poison sumac) 71. Tinea versicolor 5. Subacute eczematous inflammation 72. Tinea of the nails NEVI AND MALIGNANT MELANOMA 6. Chronic eczematous inflammation 73. Angular cheilitis 135. Nevi, melanocytic nevi, moles 7. Lichen simplex chronicus 74. Cutaneous fungal infections (tinea) 136. Atypical mole syndrome (dysplastic nevus 8. Hand eczema 75. Tinea of the foot syndrome) 9. Asteatotic eczema 76. Tinea of the groin 137. Malignant melanoma, lentigo maligna 10. Chapped, fissured feet 77. Tinea of the body 138. Melanoma mimics 11. Allergic contact dermatitis 78. Tinea of the hand 139. Congenital melanocytic nevi 12. Irritant contact dermatitis 79. Tinea incognito 13. Fingertip eczema 80. Tinea of the scalp VASCULAR TUMORS AND MALFORMATIONS 14. Keratolysis exfoliativa 81. Tinea of the beard 140. Hemangiomas of infancy 15. Nummular eczema 141. Vascular malformations 16. Pompholyx EXANTHEMS AND DRUG REACTIONS 142. Cherry angioma 17. Prurigo nodularis 82. Non-specific viral rash 143. Angiokeratoma 18. Stasis dermatitis 83. -

Acral Compound Nevus SJ Yun S Korea
University of Pennsylvania, Founded by Ben Franklin in 1740 Disclosures Consultant for Myriad Genetics and for SciBase (might try to sell you a book, as well) Multidimensional Pathway Classification of Melanocytic Tumors WHO 4th Edition, 2018 Epidemiologic, Clinical, Histologic and Genomic Aspects of Melanoma David E. Elder, MB ChB, FRCPA University of Pennsylvania, Philadelphia, PA, USA Napa, May, 2018 3rd Edition, 2006 Malignant Melanoma • A malignant tumor of melanocytes • Not all melanomas are the same – variation in: – Epidemiology – risk factors, populations – Cell/Site of origin – Precursors – Clinical morphology – Microscopic morphology – Simulants – Genomic abnormalities Incidence of Melanoma D.M. Parkin et al. CSD/Site-Related Classification • Bastian’s CSD/Site-Related Classification (Taxonomy) of Melanoma – “The guiding principles for distinguishing taxa are genetic alterations that arise early during progression; clinical or histologic features of the primary tumor; characteristics of the host, such as age of onset, ethnicity, and skin type; and the role of environmental factors such as UV radiation.” Bastian 2015 Epithelium associated Site High UV Low UV Glabrous Mucosa Benign Acquired Spitz nevus nevus Atypical Dysplastic Spitz Borderline nevus tumor High Desmopl. Low-CSD Spitzoid Acral Mucosal Malignant CSD melanoma melanoma melanoma melanoma melanoma 105 Point mutations 103 Structural Rearrangements 2018 WHO Classification of Melanoma • Integrates Epidemiologic, Genomic, Clinical and Histopathologic Features • Assists -

Rosacea: an Update
REVIEW JONELLE K. MCDONNELL, MD KENNETH J. TOMECKI, MD Department of Dermatology, Cleveland Clinic Department of Dermatology, Cleveland Clinic Rosacea: An update • ABSTRACT | >1 OSACEA is a chronic and recurrent LAM inflammatory skin disease characterized Rosacea is a common inflammatory skin disease affecting by erythema, papules, pustules, telangiectasia, the central face of adults. Its etiology is unknown. Early and occasionally sebaceous hyperplasia, which diagnosis and appropriate treatment, usually with topical or primarily affects the central face. The disease systemic antibiotics or both, minimizes symptoms and helps evolves in stages and affects middle-aged to prevent complications. adults. Early diagnosis and thoughtful manage- ment help to control the disease and to mini- • KEY POINTS mize the patient's discomfort and emotional distress. Historically, rosacea has been a mis- Rosacea has a spectrum of cutaneous clinical findings: understood disorder, often attributed to alco- facial erythema, papules, pustules, telangiectasia, and holism and acne.1 rhinophyma. • INCIDENCE Common triggers are sunlight, stress, exposure to extreme Rosacea is a common and chronic disease that heat or cold, alcohol, hot beverages, and spicy foods. affects approximately 13 million Americans, or about 1 in 20 people. Because rosacea fre- Rosacea can resemble other diseases, including acne, quently affects people of northern European seborrheic dermatitis, systemic lupus erythematosus, and heritage, it is often called the "curse of the sarcoidosis. Celts."2 In contrast, it is rarely seen in dark- skinned individuals.3 In most patients, the Ocular involvement occurs in more than 50% of patients onset occurs between the ages of 30 and 50. with rosacea. The early stages affect women more often than men at a ratio of 3 to 1, but men more often Oral tetracycline and topical metronidazole are the develop disfiguring rhinophyma. -

Topical Treatments for Seborrheic Keratosis: a Systematic Review
SYSTEMATIC REVIEW AND META-ANALYSIS Topical Treatments for Seborrheic Keratosis: A Systematic Review Ma. Celina Cephyr C. Gonzalez, Veronica Marie E. Ramos and Cynthia P. Ciriaco-Tan Department of Dermatology, College of Medicine and Philippine General Hospital, University of the Philippines Manila ABSTRACT Background. Seborrheic keratosis is a benign skin tumor removed through electrodessication, cryotherapy, or surgery. Alternative options may be beneficial to patients with contraindications to standard treatment, or those who prefer a non-invasive approach. Objectives. To determine the effectiveness and safety of topical medications on seborrheic keratosis in the clearance of lesions, compared to placebo or standard therapy. Methods. Studies involving seborrheic keratosis treated with any topical medication, compared to cryotherapy, electrodessication or placebo were obtained from MEDLINE, HERDIN, and Cochrane electronic databases from 1990 to June 2018. Results. The search strategy yielded sixty articles. Nine publications (two randomized controlled trials, two non- randomized controlled trials, three cohort studies, two case reports) covering twelve medications (hydrogen peroxide, tacalcitol, calcipotriol, maxacalcitol, ammonium lactate, tazarotene, imiquimod, trichloroacetic acid, urea, nitric-zinc oxide, potassium dobesilate, 5-fluorouracil) were identified. The analysis showed that hydrogen peroxide 40% presented the highest level of evidence and was significantly more effective in the clearance of lesions compared to placebo. Conclusion. Most of the treatments reviewed resulted in good to excellent lesion clearance, with a few well- tolerated minor adverse events. Topical therapy is a viable option; however, the level of evidence is low. Standard invasive therapy remains to be the more acceptable modality. Key Words: seborrheic keratosis, topical, systematic review INTRODUCTION Description of the condition Seborrheic keratoses (SK) are very common benign tumors of the hair-bearing skin, typically seen in the elderly population. -

Optimal Management of Common Acquired Melanocytic Nevi (Moles): Current Perspectives
Clinical, Cosmetic and Investigational Dermatology Dovepress open access to scientific and medical research Open Access Full Text Article REVIEW Optimal management of common acquired melanocytic nevi (moles): current perspectives Kabir Sardana Abstract: Although common acquired melanocytic nevi are largely benign, they are probably Payal Chakravarty one of the most common indications for cosmetic surgery encountered by dermatologists. With Khushbu Goel recent advances, noninvasive tools can largely determine the potential for malignancy, although they cannot supplant histology. Although surgical shave excision with its myriad modifications Department of Dermatology and STD, Maulana Azad Medical College and has been in vogue for decades, the lack of an adequate histological sample, the largely blind Lok Nayak Hospital, New Delhi, Delhi, nature of the procedure, and the possibility of recurrence are persisting issues. Pigment-specific India lasers were initially used in the Q-switched mode, which was based on the thermal relaxation time of the melanocyte (size 7 µm; 1 µsec), which is not the primary target in melanocytic nevus. The cluster of nevus cells (100 µm) probably lends itself to treatment with a millisecond laser rather than a nanosecond laser. Thus, normal mode pigment-specific lasers and pulsed ablative lasers (CO2/erbium [Er]:yttrium aluminum garnet [YAG]) are more suited to treat acquired melanocytic nevi. The complexities of treating this disorder can be overcome by following a structured approach by using lasers that achieve the appropriate depth to treat the three subtypes of nevi: junctional, compound, and dermal. Thus, junctional nevi respond to Q-switched/normal mode pigment lasers, where for the compound and dermal nevi, pulsed ablative laser (CO2/ Er:YAG) may be needed. -
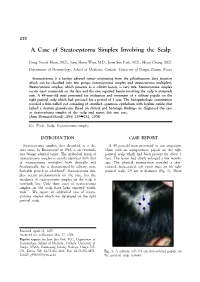
A Case of Steatocystoma Simplex Involving the Scalp
230 A Case of Steatocystoma Simplex Involving the Scalp Dong Nyeok Hyun, M.D., Jong Hoon Won, M.D., Joon Soo Park, M.D., Hyun Chung, M.D. Department of Dermatology, School of Medicine, Catholic University of Daegu, Daegu, Korea Steatocystoma is a benign adnexal tumor originating from the pilosebaceous duct junction which can be classified into two groups (steatocystoma simplex and steatocystoma multiplex). Steatocystoma simplex, which presents as a solitary lesion, is very rare. Steatocystoma simplex occurs most commonly on the face and the case reported herein involving the scalp is extremely rare. A 49-year-old man presented for evaluation and treatment of a solitary papule on the right parietal scalp which had persisted for a period of 1 year. The histopathologic examination revealed a thin-walled cyst consisting of stratified squamous epithelium with hyaline cuticle that lacked a stratum granulosum. Based on clinical and histologic findings, we diagnosed this case as steatocystoma simplex of the scalp and report this rare case. (Ann Dermatol (Seoul) 20(4) 230∼232, 2008) Key Words: Scalp, Steatocystoma simplex INTRODUCTION CASE REPORT Steatocystoma simplex, first described as a dis- A 49-year-old man presented to our outpatient tinct entity by Brownstein1 in 1982, is an extremely clinic with an asymptomatic papule on the right rare benign adnexal tumor. The individual lesion of parietal scalp which had been present for about 1 steatocystoma simplex is usually identical with that year. The lesion had slowly enlarged a few months of steatocystoma multiplex, both clinically and ago. The physical examination revealed a skin- histologically, but is characterized by solitary, non- colored, deep-seated, soft cystic mass on his right heritable growth in adulthood1. -

Pathogenesis of Rosacea Anetta E
REVIEW Pathogenesis of Rosacea Anetta E. Reszko, MD, PhD; Richard D. Granstein, MD Rosacea is a chronic, common skin disorder whose pathogenesis is incompletely understood. An inter- play of multiple factors, including genetic predisposition and environmental, neurogenic, and microbial factors, may be involved in the disease process. Rosacea subtypes, identified in the recently published standard classification system by the National Rosacea Society Expert Committee on the Classification and Staging of Rosacea, may in fact represent different disease processes, and identifying subtypes may allow investigators to pursue more precisely focused studies. New developments in molecular biology and genetics hold promise for elucidating the interplay of the multiple factors involved in the pathogen- esis of rosacea, as well as providing the bases for potential new therapies. osacea is a common, chronic skin disorder and secondary features needed for the clinical diagnosis primarily affecting the central and con- of rosacea. Primary features include flushing (transient vex areas of COSthe face. The nose, cheeks, DERM erythema), persistent erythema, papules and pustules, chin, forehead, and glabella are the most and telangiectasias. Secondary features include burn- frequently affected sites. Less commonly ing and stinging, skin dryness, plaque formation, dry affectedR sites include the infraorbital, submental, and ret- appearance, edema, ocular symptoms, extrafacial mani- roauricular areas, the V-shaped area of the chest, and the festations, and phymatous changes. One or more of the neck, the back, and theDo scalp. Notprimary Copy features is needed for diagnosis.1 The disease has a variety of clinical manifestations, Several authors have theorized that rosacea progresses including flushing, persistent erythema, telangiecta- from one stage to another.2-4 However, recent data, sias, papules, pustules, and tissue and sebaceous gland including data on therapeutic modalities of various sub- hyperplasia. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -
Cryosurgery Using the Cryopen®
Cryosurgery using the CryoPen® FAQ CRYOSURGERY What is cryosurgery? Cryosurgery is a procedure that uses extreme cold to destroy tissue. How can my practice benefit from using cryosurgery in my practice? Cryosurgery in the office offers an excellent modality for eliminating referral time while creating an added source of revenue. How can my patients benefit from having cryosurgery in my practice? Patients will appreciate the efficient use of their time and decreased cost of services by avoiding secondary visits to specialists. By keeping the procedure in house, patients will put a greater value on your practice. How is cryosurgery better than other methods of removing skin lesions? Cryosurgery requires no anesthesia and has less scarring than other techniques of skin lesion removal with minimal post-op care. What is the mechanism of cell destruction in cryosurgery? Cell destruction occurs when a cell is rapidly brought down to a very low temperature. When these two criteria are met (varies with cell type), ice crystals form, destroying the cell organelles and protein matrixes. Water then rushes into the surrounding area causing a blister and a disruption of the local blood supply. Cytologic evidence of cell destruction can be seen as soon as two hours after the procedure. What types of lesions are appropriate to freeze? Almost any unwanted skin lesions are appropriate such as warts, moles, actinic keratosis, seborrheic keratosis, keloids, lentigos, dermatofibromas, and hemangiomas to just name a few. In most practices, over 90% of unwanted lesions encountered are amenable to using cryosurgery. What types of lesions are not appropriate to freeze? All Melanomas and Recurrent Basal Cell Carcinomas are contraindicated for cryosurgery. -

What to Expect Following Cryosurgery “Freezing”
What to Expect Following CryoSurgery “Freezing” What is Cryosurgery? Cryosurgery is a technique for removing skin lesions that primarily involve the surface of the skin, such as warts, seborrheic keratosis, or actinic keratosis. It is a quick method of removing the lesions with minimal scarring. The liquid nitrogen needs to be applied long enough to freeze the affected skin. By freezing the skin, a blister is created underneath the lesion. Ideally, as the new skin forms underneath the blister, the abnormal skin on the roof of the blister peels off. Occasionally if the lesion is very thick (such as a large wart), only the surface is blistered off. The base or residual lesion may need to be frozen at another visit. What to Expect Over the Next Few Weeks? During Treatment – Area being treated will sting, burn and then possibly itch. Immediately After Treatment – Area will be red sore and swollen. Next Day- Blister or blood blister has formed, tenderness starts to subside. Apply a Band-Aid if necessary. 7 Days- Surface is dark red/brown and scab-like. Apply Vaseline or an antibacterial ointment if necessary. 2 to 4 Weeks- The surface starts to peel off. This may be encouraged gently during bathing, when the scab is softened. No makeup should be applied until area is fully healed. How to Take care of the Skin after Cryosurgery A Band-Aid can be used for larger blisters or blisters in areas that are more likely to be traumatized- such as fingers and toes. If the area becomes dry or crusted, an ointment (Vaseline, Aquaphor) can also be applied.