Common Arrhythmias� Disclosures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Unstable Angina with Tachycardia: Clinical and Therapeutic Implications
Unstable angina with tachycardia: Clinical and therapeutic implications We prospectively evaluated 19 patients with prolonged chest pain not evolving to myocardiai infarction and accompanied with reversible ST-T changes and tachycardia (heart rate >lOO beats/min) in order to correlate heart rate reduction with ischemic electrocardiographic (ECG) changes. Fourteen patients (74%) received previous long-term combined treatment with nifedipine and nitrates. Continuous ECG monitoring was carried out until heart rate reduction and at least one of the following occurred: (1) relief of pain or (2) resolution of ischemic ECG changes. The study protocol consisted of carotid massage in three patients (IS%), intravenous propranolol in seven patients (37%), slow intravenous amiodarone infusion in two patients (lo%), and intravenous verapamil in four patients (21%) with atrial fibrillation. In three patients (16%) we observed a spontaneous heart rate reduction on admission. Patients responded with heart rate reduction from a mean of 126 + 10.4 beats/min to 64 k 7.5 beats/min (p < 0.005) and an ST segment shift of 4.3 k 2.13 mm to 0.89 k 0.74 mm (p < 0.005) within a mean interval of 13.2 + 12.7 minutes. Fifteen (79%) had complete response and the other four (21%) had partial relief of pain. A significant direct correlation was observed for heart rate reduction and ST segment deviation (depression or elevation) (f = 0.7527 and 0.8739, respectively). These patients represent a unique subgroup of unstable angina, in which the mechanism responsible for ischemia is excessive increase in heart rate. Conventional vasodilator therapy may be deleterious, and heart rate reduction Is mandatory. -

Respiration Driven Excessive Sinus Tachycardia Treated with Clonidine Matthew Emile Li Kam Wa,1 Patricia Taraborrelli,1 Sajad Hayat,2 Phang Boon Lim1
Novel treatment (new drug/intervention; established drug/procedure in new situation) BMJ Case Reports: first published as 10.1136/bcr-2016-216818 on 28 April 2017. Downloaded from CASE REPORT Respiration driven excessive sinus tachycardia treated with clonidine Matthew Emile Li Kam Wa,1 Patricia Taraborrelli,1 Sajad Hayat,2 Phang Boon Lim1 1Department of Cardiology, SUMMARY no evidence of dual AV node physiology, accessory Imperial College Healthcare A 26-year-old man presented to our syncope service pathway or inducible supraventricular tachycardia. NHS Trust, London, UK 2Department of Cardiology, with debilitating daily palpitations, shortness of breath, A subsequent permanent pacemaker led to no University Hospitals Coventry presyncope and syncope following a severe viral further episodes of frank syncope. However his and Warwickshire NHS Trust, respiratory illness 4 years previously. Mobitz type II block ongoing debilitating exertional and respiratory- Coventry, UK had previously been identified, leading to a permanent driven palpitations with presyncope remained. pacemaker and no further episodes of frank syncope. Conservative measures including increased fluid Correspondence to Dr Phang Boon Lim, Transthoracic echocardiography, electophysiological study intake and compression stockings had no effect. [email protected] and repeated urine metanepherines were normal. His Trials of medication including fludrocortisone, fle- palpitations and presyncope were reproducible on deep cainide, β blockers and ivabradine were either not Accepted 18 December 2016 inspiration, coughing, isometric hand exercise and tolerated or had no significant effect on his passive leg raises. We demonstrated rapid increases in symptoms. heart rate with no change in morphology on his 12 lead During a simple active stand over 3 min, his ECG. -

Basic Rhythm Recognition
Electrocardiographic Interpretation Basic Rhythm Recognition William Brady, MD Department of Emergency Medicine Cardiac Rhythms Anatomy of a Rhythm Strip A Review of the Electrical System Intrinsic Pacemakers Cells These cells have property known as “Automaticity”— means they can spontaneously depolarize. Sinus Node Primary pacemaker Fires at a rate of 60-100 bpm AV Junction Fires at a rate of 40-60 bpm Ventricular (Purkinje Fibers) Less than 40 bpm What’s Normal P Wave Atrial Depolarization PR Interval (Normal 0.12-0.20) Beginning of the P to onset of QRS QRS Ventricular Depolarization QRS Interval (Normal <0.10) Period (or length of time) it takes for the ventricles to depolarize The Key to Success… …A systematic approach! Rate Rhythm P Waves PR Interval P and QRS Correlation QRS Rate Pacemaker A rather ill patient……… Very apparent inferolateral STEMI……with less apparent complete heart block RATE . Fast vs Slow . QRS Width Narrow QRS Wide QRS Narrow QRS Wide QRS Tachycardia Tachycardia Bradycardia Bradycardia Regular Irregular Regular Irregular Sinus Brady Idioventricular A-Fib / Flutter Bradycardia w/ BBB Sinus Tach A-Fib VT PVT Junctional 2 AVB / II PSVT A-Flutter SVT aberrant A-Fib 1 AVB 3 AVB A-Flutter MAT 2 AVB / I or II PAT PAT 3 AVB ST PAC / PVC Stability Hypotension / hypoperfusion Altered mental status Chest pain – Coronary ischemic Dyspnea – Pulmonary edema Sinus Rhythm Sinus Rhythm P Wave PR Interval QRS Rate Rhythm Pacemaker Comment . Before . Constant, . Rate 60-100 . Regular . SA Node Upright in each QRS regular . Interval =/< leads I, II, . Look . Interval .12- .10 & III alike .20 Conduction Image reference: Cardionetics/ http://www.cardionetics.com/docs/healthcr/ecg/arrhy/0100_bd.htm Sinus Pause A delay of activation within the atria for a period between 1.7 and 3 seconds A palpitation is likely to be felt by the patient as the sinus beat following the pause may be a heavy beat. -

Basic Cardiac Rhythms – Identification and Response Module 1 ANATOMY, PHYSIOLOGY, & ELECTRICAL CONDUCTION Objectives
Basic Cardiac Rhythms – Identification and Response Module 1 ANATOMY, PHYSIOLOGY, & ELECTRICAL CONDUCTION Objectives ▪ Describe the normal cardiac anatomy and physiology and normal electrical conduction through the heart. ▪ Identify and relate waveforms to the cardiac cycle. Cardiac Anatomy ▪ 2 upper chambers ▪ Right and left atria ▪ 2 lower chambers ▪ Right and left ventricle ▪ 2 Atrioventricular valves (Mitral & Tricuspid) ▪ Open with ventricular diastole ▪ Close with ventricular systole ▪ 2 Semilunar Valves (Aortic & Pulmonic) ▪ Open with ventricular systole ▪ Open with ventricular diastole The Cardiovascular System ▪ Pulmonary Circulation ▪ Unoxygenated – right side of the heart ▪ Systemic Circulation ▪ Oxygenated – left side of the heart Anatomy Coronary Arteries How The Heart Works Anatomy Coronary Arteries ▪ 2 major vessels of the coronary circulation ▪ Left main coronary artery ▪ Left anterior descending and circumflex branches ▪ Right main coronary artery ▪ The left and right coronary arteries originate at the base of the aorta from openings called the coronary ostia behind the aortic valve leaflets. Physiology Blood Flow Unoxygenated blood flows from inferior and superior vena cava Right Atrium Tricuspid Valve Right Ventricle Pulmonic Valve Lungs Through Pulmonary system Physiology Blood Flow Oxygenated blood flows from the pulmonary veins Left Atrium Mitral Valve Left Ventricle Aortic Valve Systemic Circulation ▪ Blood Flow Through The Heart ▪ Cardiology Rap Physiology ▪ Cardiac cycle ▪ Represents the actual time sequence between -

Acute Non-Specific Pericarditis R
Postgrad Med J: first published as 10.1136/pgmj.43.502.534 on 1 August 1967. Downloaded from Postgrad. med. J. (August 1967) 43, 534-538. CURRENT SURVEY Acute non-specific pericarditis R. G. GOLD * M.B., B.S., M.RA.C.P., M.R.C.P. Senior Registrar, Cardiac Department, Brompton Hospital, London, S.W.3 Incidence neck, to either flank and frequently through to the Acute non-specific pericarditis (acute benign back. Occasionally pain is experienced on swallow- pericarditis; acute idiopathic pericarditis) has been ing (McGuire et al., 1954) and this was the pre- recognized for over 100 years (Christian, 1951). In senting symptom in one of our own patients. Mild 1942 Barnes & Burchell described fourteen cases attacks of premonitory chest pain may occur up to of the condition and since then several series of 4 weeks before the main onset of symptoms cases have been published (Krook, 1954; Scherl, (Martin, 1966). Malaise is very common, and is 1956; Swan, 1960; Martin, 1966; Logue & often severe and accompanied by listlessness and Wendkos, 1948). depression. The latter symptom is especially com- Until recently Swan's (1960) series of fourteen mon in patients suffering multiple relapses or patients was the largest collection of cases in this prolonged attacks, but is only partly related to the country. In 1966 Martin was able to collect most length of the illness and fluctuates markedly from of his nineteen cases within 1 year in a 550-bed day to day with the patient's general condition. hospital. The disease is thus by no means rare and Tachycardia occurs in almost every patient at warrants greater attention than has previously some stage of the illness. -

Recurrent Takotsubo Cardiomyopathy: a Rare Diagnosis with a Common Emergency Department Presentation Emily M Miner, Harini Gurram, Tennie Renkens and Julie L
Case Report iMedPub Journals ARCHIVES OF MEDICINE 2017 http://www.imedpub.com/ Vol.9 No.4:8 ISSN 1989-5216 DOI: 10.21767/1989-5216.1000229 Recurrent Takotsubo Cardiomyopathy: A Rare Diagnosis with a Common Emergency Department Presentation Emily M Miner, Harini Gurram, Tennie Renkens and Julie L. Welch* Department of Emergency Medicine, Indiana University School of Medicine, Indianapolis, Indiana, USA *Corresponding author: Julie L Welch, Department of Emergency Medicine, Indiana University School of Medicine, Indianapolis, Indiana, USA, Tel: 317-962-8880; E-mail: [email protected] Received date: August 08, 2017; Accepted date: August 14, 2017; Published date: August 16, 2017 Citation: Miner EM, Gurram H, Renkens T, Welch JL. Recurrent Takotsubo Cardiomyopathy: A Rare Diagnosis with a Common Emergency Department Presentation. Arch Med. 2017, 9:4 Copyright: © 2017 Miner EM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. The incidence of recurrent Takotsubo cardiomyopathy after initial diagnosis is about 5% at 6 years with recurrence being Abstract more common when the initial episode has more severe left ventricular dysfunction [4]. While the long-term prognosis of Takotsubo cardiomyopathy is a non-ischemic Takotsubo is favorable in >95% of cases, acute symptoms of an cardiomyopathy that is often triggered by a physical or episode can be life-threatening and lead to cardiogenic shock emotional stressor and commonly affects post-menopausal [5]. Proper diagnosis is crucial in these life-threatening women. A 57 year old female with a significant past medical history for atrial fibrillation, anxiety, and Takotsubo situations. -

Inappropriate Sinus Tachycardia Following Viral Illness
Case Report Inappropriate Sinus Tachycardia Following Viral Illness Khalid Sawalha 1,* , Fuad Habash 2 , Srikanth Vallurupalli 2 and Hakan Paydak 3 1 Internal Medicine Division, White River Health System, Batesville, AR 72501, USA 2 Cardiology Division, University of Arkansas for Medical Sciences, Little Rock, AR 72205, USA; [email protected] (F.H.); [email protected] (S.V.) 3 Electrophysiology Division, University of Arkansas for Medical Sciences, Little Rock, AR 72205, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-984-364-1158 Abstract: A 67-year-old female patient with a past medical history of menopause, migraines, and gastro-esophageal disease presented with palpitation, fatigue, and shortness of breath. One month prior to her presentation, she reported having flu-like symptoms. Her EKG showed sinus tachycar- dia with no other abnormality. Laboratory findings, along with imaging, showed normal results. The event monitor failed to detect any arrythmias. We report a case of inappropriate sinus tachycardia secondary to viral infection as a diagnosis of exclusion. Keywords: inappropriate sinus tachycardia; viral infection; palpitations 1. Introduction Inappropriate sinus tachycardia, also called chronic non-paroxysmal sinus tachycardia, is an unusual condition that occurs in individuals without apparent heart disease or other cause of sinus tachycardia, such as hyperthyroidism or fever, and is generally considered a diagnosis of exclusion [1–4]. Inappropriate sinus tachycardia is defined as a resting heart Citation: Sawalha, K.; Habash, F.; rate >100 beats per minute associated with highly symptomatic palpitations [5,6]. Vallurupalli, S.; Paydak, H. Commonly used criteria to define inappropriate sinus tachycardia include [7] P-wave Inappropriate Sinus Tachycardia axis and morphology similar to sinus rhythm, and a resting heart rate of 100 beats per Following Viral Illness. -
ACLS Rhythms for the ACLS Algorithms
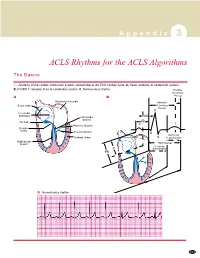
A p p e n d i x 3 ACLS Rhythms for the ACLS Algorithms The Basics 1. Anatomy of the cardiac conduction system: relationship to the ECG cardiac cycle. A, Heart: anatomy of conduction system. B, P-QRS-T complex: lines to conduction system. C, Normal sinus rhythm. Relative Refractory A B Period Bachmann’s bundle Absolute Sinus node Refractory Period R Internodal pathways Left bundle AVN branch AV node PR T Posterior division P Bundle of His Anterior division Q Ventricular Purkinje fibers S Repolarization Right bundle branch QT Interval Ventricular P Depolarization PR C Normal sinus rhythm 253 A p p e n d i x 3 The Cardiac Arrest Rhythms 2. Ventricular Fibrillation/Pulseless Ventricular Tachycardia Pathophysiology ■ Ventricles consist of areas of normal myocardium alternating with areas of ischemic, injured, or infarcted myocardium, leading to chaotic pattern of ventricular depolarization Defining Criteria per ECG ■ Rate/QRS complex: unable to determine; no recognizable P, QRS, or T waves ■ Rhythm: indeterminate; pattern of sharp up (peak) and down (trough) deflections ■ Amplitude: measured from peak-to-trough; often used subjectively to describe VF as fine (peak-to- trough 2 to <5 mm), medium-moderate (5 to <10 mm), coarse (10 to <15 mm), very coarse (>15 mm) Clinical Manifestations ■ Pulse disappears with onset of VF ■ Collapse, unconsciousness ■ Agonal breaths ➔ apnea in <5 min ■ Onset of reversible death Common Etiologies ■ Acute coronary syndromes leading to ischemic areas of myocardium ■ Stable-to-unstable VT, untreated ■ PVCs with -

The Pattern of Cardiac Arrhythmias in Acute ST Elevated Myocardial
University Heart Journal Vol. 16, No. 1, January 2020 The Pattern of Cardiac Arrhythmias in Acute ST Elevated 16 Myocardial Infarction and their in-hospital Outcome MOHAMMAD KHURSHADUL ALAM, MANZOOR MAHMOOD, DIPAL KRISHNA ADHIKARY, FAKHRUL ISLAM 01 - V KHALED, MSI TIPU CHOWDHURY, AMANAT HASAN, SAMI NAZRUL ISLAM, MD. ASHRAF UDDIN SULTAN, SAJAL KRISHNA BANERJEE Department of Cardiology, Bangabandhu Sheikh Mujib Medical University, Dhaka,Bangladesh. ol. 16, No. 1, Address of Correspondence: Dr. Muhammad Khurshadul Alam, Department of Cardiology,Bangabandhu Sheikh MujibMedical University,Dhaka,Bangladesh. Email: [email protected] Abstract: Background: Acute myocardial infarction (AMI) is a major cause of death worldwide with arrhythmia being JANUAR the most common determinant in the post-infarction period. Identification and management of arrhythmias at an early period of acute MI has both short term and long term significance.Objective: The aim of the study is to evaluate the pattern of arrhythmias in acute STEMI in the first 48 hours of hospitalization and their in- hospital outcome. Methods: A total of 50 patients with acute STEMI were included in the study after considering Y 2020 BSMMU H.J. the inclusion and exclusion criteria. The patients were observed for the first 48 hours of hospitalization for detection of arrhythmia with baseline ECG at admission and continuous cardiac monitoring in the CCU. The pattern of the arrhythmias during this period & their in-hospital outcome were recorded in predesigned structured data collection sheet.Result: The mean age was 53.38 ± 10.22 years ranging from 29 to 70 years. Most of the patients were male 42(84%). -

Inappropriate Sinus Tachycardia
Inappropriate Sinus Tachycardia: Focus on Ivabradine Hany S. Abed, MBBS PhD†; Jordan Fulcher, MBBS†; Michael J Kilborn, MBBS PhD†; Anthony C. Keech, MBBS, MClinEpi.† †Department of Cardiology, Royal Prince Alfred Hospital and NHMRC Clinical Trials Centre, University of Sydney, Sydney, NSW, Australia Address for correspondence: Professor Anthony C. Keech NHMRC Clinical Trials Centre K25 - Medical Foundation Building University of Sydney, NSW, Australia, 2006 Phone: +61 9562 5003 Fax: +61 9565 1863 Email: [email protected] Accepted Article This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record. Please cite this article as doi: 10.1002/imj.13093 This article is protected by copyright. All rights reserved. Abstract Inappropriate sinus tachycardia (IST) is an incompletely understood condition characterised by an elevation in heart rate (HR) accompanied by wide ranging symptoms, in the absence of an underlying physiological stimulus. The condition often takes a chronic course with significant adverse effects on quality of life. Currently there is no effective treatment for IST. Beta-blockers, generally considered the cornerstone of treatment, are often ineffective and poorly tolerated. Ivabradine is a novel sinus node If “funny current” inhibitor which reduces the HR. It has been approved for the treatment of beta-blocker refractory chronic systolic heart failure and chronic stable angina, but more recently shown promise in the treatment of IST. This review provides an overview of IST prevalence and mechanisms, followed by an examination of the evidence for the role and efficacy of ivabradine in the treatment of IST. -

Cardiac Arrhythmias in Acute Coronary Syndromes: Position Paper from the Joint EHRA, ACCA, and EAPCI Task Force
FOCUS ARTICLE Euro Intervention 2014;10-online publish-ahead-of-print August 2014 Cardiac arrhythmias in acute coronary syndromes: position paper from the joint EHRA, ACCA, and EAPCI task force Bulent Gorenek*† (Chairperson, Turkey), Carina Blomström Lundqvist† (Sweden), Josep Brugada Terradellas† (Spain), A. John Camm† (UK), Gerhard Hindricks† (Germany), Kurt Huber‡ (Austria), Paulus Kirchhof† (UK), Karl-Heinz Kuck† (Germany), Gulmira Kudaiberdieva† (Turkey), Tina Lin† (Germany), Antonio Raviele† (Italy), Massimo Santini† (Italy), Roland Richard Tilz† (Germany), Marco Valgimigli¶ (The Netherlands), Marc A. Vos† (The Netherlands), Christian Vrints‡ (Belgium), and Uwe Zeymer‡ (Germany) Document Reviewers: Gregory Y.H. Lip (Review Coordinator) (UK), Tatjania Potpara (Serbia), Laurent Fauchier (France), Christian Sticherling (Switzerland), Marco Roffi (Switzerland), Petr Widimsky (Czech Republic), Julinda Mehilli (Germany), Maddalena Lettino (Italy), Francois Schiele (France), Peter Sinnaeve (Belgium), Giueseppe Boriani (Italy), Deirdre Lane (UK), and Irene Savelieva (on behalf of EP-Europace, UK) Introduction treatment. Atrial fibrillation (AF) may also warrant urgent treat- It is known that myocardial ischaemia and infarction leads to severe ment when a fast ventricular rate is associated with hemodynamic metabolic and electrophysiological changes that induce silent or deterioration. The management of other arrhythmias is also based symptomatic life-threatening arrhythmias. Sudden cardiac death is largely on symptoms rather than to avert -

Inappropriate Sinus Tachycardia
Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families Inappropriate sinus tachycardia This information sheet from Great Ormond Street Hospital (GOSH) explains the causes, symptoms and treatment of inappropriate sinus tachycardia and where to get help. What is inappropriate sinus tachycardia? Inappropriate sinus tachycardia (IST) is a condition Normal resting heart rate ranges between 50 and that causes an abnormally high resting heart rate. 80 beats per minute for adolescents and adults but IST is thought to be caused by an abnormality in someone with IST will either have a resting heart the sinoatrial (SA) node, although other factors rate of 100 beats per minute or more, or their may also affect development of IST. heart rate will suddenly increase to over 100 beats The heart has an electrical system that makes it per minute for instance when moving from a lying pump. An electrical impulse starts in a specialised position to sitting. When asleep or at rest, their area of heart tissue in the right atrium called the heart rate returns to normal. SA Node. It then passes from the right atrium through to the ventricles via the AV node. As What causes inappropriate the impulse passes through the atrium it makes sinus tachycardia? it pump blood into the ventricle. It has the same There are many theories as to the cause of effect when it passes through the ventricle. inappropriate sinus tachycardia (IST) and more This electrical impulse travels through the heart research is needed to confirm the cause(s). One each time it beats.