Ankle Sprain
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Shoulder Sprain a Sprain Is a Stretch And/Or Tear of a Ligament, a Strong Band of Connective Tissue That Connect the End of One Bone with Another
INDUSTRYADVANTAGE THERAPY UPDATE April 2016 A Courtesy Publication for the Monett area HR/Safety Community Sprains & Strains: What’s the difference? Does seeing the term “shoulder injury” at a glance make you cringe? In the work comp world, shoulder injuries can turn into costly claims involving surgery and long-term rehabilitation. Often times, shoulder injuries begin as sprains or strains and can be treated with conservative, non-operative treatment. In this month’s Industry Update, we’ll review sprains and strains as well as other factors that can contribute to shoulder injuries in the workplace. Shoulder Sprain A sprain is a stretch and/or tear of a ligament, a strong band of connective tissue that connect the end of one bone with another. In the shoulder complex, common sprains involve the supporting ligaments of the joint between the end of the collar bone and the shoulder blade - the acromioclavicular (AC) joint. Shoulder sprains can occur during repetitive reaching or lifting activities, or with falls onto the shoulder. Treatment for mild sprains includes RICE (Rest, Ice, Compression, Elevation) and exercises to improve muscle balance, preserve joint mobility, and provide support for ligaments. Shoulder Strain A strain is an injury to a muscle and/or tendons. Tendons are fibrous cords of tissue that attach muscles to the bone. Typical symptoms of a strain include pain, muscle spasm, muscle weakness, swelling, inflammation, and cramping. Strains are common when a pushed, pulled, or lifted object suddenly gives way. They can also be wear-and- tear injuries or a result from reaching out during a fall. -

Total HIP Replacement Exercise Program 1. Ankle Pumps 2. Quad
3 sets of 10 reps (30 ea) 2 times a day Total HIP Replacement Exercise Program 5. Heel slides 1. Ankle Pumps Bend knee and pull heel toward buttocks. DO NOT GO Gently point toes up towards your nose and down PAST 90* HIP FLEXION towards the surface. Do both ankles at the same time or alternating feet. Perform slowly. 2. Quad Sets Slowly tighten thigh muscles of legs, pushing knees down into the surface. Hold for 10 count. 6. Short Arc Quads Place a large can or rolled towel (about 8”diameter) under the leg. Straighten knee and leg. Hold straight for 5 count. 3. Gluteal Sets Squeeze the buttocks together as tightly as possible. Hold for a 10 count. 7. Knee extension - Long Arc Quads Slowly straighten operated leg and try to hold it for 5 sec. Bend knee, taking foot under the chair. 4. Abduction and Adduction Slide leg out to the side. Keep kneecap pointing toward ceiling. Gently bring leg back to pillow. May do both legs at the same time. Copywriter VHI Corp 3 sets of 10 reps (30 ea) 2 times a day Total HIP Replacement Exercise Program 8. Standing Stair/Step Training: Heel/Toe Raises: 1. The “good” (non-operated) leg goes Holding on to an immovable surface. UP first. Rise up on toes slowly 2. The “bad” (operated) leg goes for a 5 count. Come back to foot flat and lift DOWN first. toes from floor. 3. The cane stays on the level of the operated leg. Resting positions: To Stretch your hip to neutral position: 1. -

Human Functional Anatomy 213 the Ankle and Foot In
2 HUMAN FUNCTIONAL ANATOMY 213 JOINTS OF THE FOOT THE ANKLE AND FOOT IN LOCOMOTION THE HINDFOOT -(JOINTS OF THE TALUS) THIS WEEKS LAB: Forearm and hand TROCHLEAR The ankle, and distal tibiofibular joints READINGS BODY The leg and sole of foot Subtalar joint (Posterior talocalcaneal) 1. Stern – Core concepts – sections 99, 100 and 101 (plus appendices) HEAD 2. Faiz and Moffat – Anatomy at a Glance – Sections 50 and 51 Talocalcaneonavicular 3. Grants Method:- The bones and sole of foot & Joints of the lower limb & Transverse tarsal joints or any other regional textbook - similar sections IN THIS LECTURE I WILL COVER: Joints related to the talus Ankle Subtalar Talocalcaneonavicular THE MID FOOT Transverse tarsal Other tarsal joints THE FOREFOOT Toe joints METATARSAL AND PHALANGEAL Ligaments of the foot JOINTS (same as in the hand) Arches of the foot Except 1st metatarsal and Hallux Movements of the foot & Compartments of the leg No saddle joint at base is 1st metatarsal The ankle in Locomotion Metatarsal head is bound by deep Ankle limps transverse metatarsal ligament 1. Flexor limp Toes are like fingers 2. Extensor limp Same joints, Lumbricals, Interossei, Extensor expansion Axis of foot (for abduction-adduction) is the 2nd toe. 3 4 JOINTS OF THE FOOT JOINTS OF THE FOOT (2 joints that allow inversion and eversion) DISTAL TIBIOFIBULAR SUBTALAR (Posterior talocalcaneal) JOINT Syndesmosis (fibrous joint like interosseous membrane) Two (or three) talocalcaneal joints Posterior is subtalar Fibres arranged to allow a little movement Anterior (and middle) is part of the talocalcaneonavicular. With a strong interosseus ligament running between them (tarsal sinus) THE TALOCALCANEONAVICULAR JOINT The head of the talus fits into a socket formed from the: The anterior talocalcaneal facets. -
The 7 Step Shin Splints Treatment System
The Step SShhiinn SSpplliinnttss Treatment System By Brad Walker TM The 7 Step Shin Splints Treatment System Fix Your Shin Splints Once and For All and get back to Pain Free Running Quickly and Safely. Walker, Bradley E., 1971 7 Step Shin Splints Treatment System™ Copyright © 2012 The Stretching Institute™ All rights reserved. Except under conditions described in the copyright act, no part of this publication may in any form or by any means (electronic, mechanical, micro copying, photocopying, recording or otherwise) be reproduced, stored in a retrieval system or transmitted without prior written permission from the copyright owner. Inquires should be addressed to the publisher. Disclaimers The exercises presented in this publication are intended as an educational resource and are not intended as a substitute for proper medical advice. Please consult your physician, physical therapist or sports coach before performing any of the exercises described in this publication, particularly if you are pregnant, elderly or have any chronic or recurring muscle or joint pain. Discontinue any exercise that causes you pain or severe discomfort and consult a medical expert. Cover picture/s supplied by iStockphoto. The Stretching Institute has purchased the non-exclusive, non-transferable, non-sub licensable right to reproduce the cover picture/s an unlimited number of times in online and electronic publications, and web advertisements. Exercise graphics used with permission from the Physigraphe V2 Pro Clip Art CD-ROM available at ExRx.net. Copyright -

Shoulder Conditions Diagnosis and Treatment Guideline
Shoulder Conditions Diagnosis and Treatment Guideline TABLE OF CONTENTS I. Review Criteria for Shoulder Surgery II. Introduction III. Establishing Work-Relatedness A. Shoulder Conditions as Industrial Injuries B. Shoulder Conditions as Occupational Diseases IV. Making the Diagnosis A. History and Clinical Exam B. Diagnostic Imaging V. Treatment A. Conservative Treatment B. Surgical Treatment VI. Specific Conditions A. Rotator Cuff Tears B. Subacromial Impingement Syndrome without a Rotator Cuff Tear C. Calcific tendonitis D. Labral tears including superior labral anterior-posterior (SLAP) tears E. Acromioclavicular dislocation F. Acromioclavicular arthritis G. Glenohumeral dislocation H. Tendon rupture or tendinopathy of the long head of the biceps I. Glenohumeral arthritis and arthropathy J. Manipulation under anesthesia K. Diagnostic arthroscopy VII. Post-operative Treatment and Return to Work VIII. Specific Shoulder Tests IX. Functional Disability Scales for Shoulder Conditions X. References 1 Hyperlink update September 2016 I. REVIEW CRITERIA FOR SHOULDER SURGERY Criteria for Shoulder Surgery A request may be AND this has been done If the patient has AND the diagnosis is supported by these clinical findings: appropriate for (if recommended) Surgical Procedure Diagnosis Subjective Objective Imaging Non-operative care Rotator cuff tear repair Acute full-thickness Report of an acute Patient will usually have Conventional x-rays, AP and May be offered but not rotator cuff tear traumatic injury within 3 weakness with one or true lateral or axillary view required Note: The use of allografts months of seeking care more of the following: and xenografts in rotator Forward elevation AND cuff tear repair is not AND Internal/external MRI, ultrasound or x-ray covered. -

Compression Garments for Leg Lymphoedema
Compression garments for leg lymphoedema You have been fitted with a compression garment to help reduce the lymphoedema in your leg. Compression stockings work by limiting the amount of fluid building up in your leg. They provide firm support, enabling the muscles to pump fluid away more effectively. They provide most pressure at the foot and less at the top of the leg so fluid is pushed out of the limb where it will drain away more easily. How do I wear it? • Wear your garment every day to control the swelling in your leg. • Put your garment on as soon as possible after getting up in the morning. This is because as soon as you stand up and start to move around extra fluid goes into your leg and it begins to swell. • Take the garment off before bedtime unless otherwise instructed by your therapist. We appreciate that in hot weather garments can be uncomfortable, but unfortunately this is when it is important to wear it as the heat can increase the swelling. If you would like to leave off your garment for a special occasion please ask the clinic for advice. What should I look out for? Your garment should feel firm but not uncomfortable: • If you notice the garment is rubbing or cutting in, adjust the garment or remove it and reapply it. • If your garment feels tight during the day, try and think about what may have caused this. If you have been busy, sit down and elevate your leg and rest for at least 30 minutes. -

Elbow Rehab UCL Sprain Non Operative.Pages
Conservative Treatment Following Ulnar Collateral Ligament Sprains Of the Elbow Phase I Immediate Motion Phase Post-Injury days 0 - 7 Goals 1. Increase ROM 2. Promote healing of ulnar collateral ligament 3. Retard muscular atrophy 4. Decrease pain and inflammation 5. 1 week post-injury initiate cardiovascular conditioning program with modifications for injury per the ClevelandIndians Physical Development Program (start at Week 1 in manual) Activities 1. Brace (optional) - non-painful ROM (20 →90 degrees) 2. AAROM, PROM elbow, wrist and shoulder (non-painful ROM and no shoulder ER stretching) 3. Initiate Isometrics - wrist and elbow musculature, gripping exercises 4. Ice, compression 5. Initiate shoulder strengthening ( no internal rotation ) - CAUTION: avoid stressing medial elbow Phase II Intermediate Phase Post-Injury Weeks 2 - 4 Goals 1. Increase ROM 2. Improve strength and endurance 3. Decrease pain and inflammation 4. Promote stability 5. 2 weeks post-injury initiate upper/lower body strength program with modifications for injury per the Cleveland Indians Physical Development Program (start at Week 1 in manual) Criteria to Progress to Phase II 1. No Swelling 2. Acute pain is diminished Activities 1. ROM exercises - gradual increase in motion ( 0 → 135 degrees) • 5 degrees of extension, 10 degrees of flexion 2. Initiate isotonic exercises • wrist curls • wrist extension • pronation/supination • biceps/triceps 3. Advance shoulder strengthening • external rotation • internal rotation (Week 3) • supraspinatus 4. Ice, compression Phase III Advanced Strengthening phase Post-Injury Weeks 5 - 6 Criteria to progress to Phase III 1. Full AROM 2. No pain or tenderness 3. No increase in laxity 4. Strength 4/5 in the elbow flexors/extensors Goals 1. -

Sports Ankle Injuries Assessment and Management
FOCUS Sports injuries Sports ankle injuries Drew Slimmon Peter Brukner Assessment and management Background Case study Lucia is a female, 16 years of age, who plays netball with the Sports ankle injuries present commonly in the general state under 17s netball team. She presents with an ankle injury practice setting. The majority of these injuries are inversion sustained at training the previous night. She is on crutches and plantar flexion injuries that result in damage to the and is nonweight bearing. Examination raises the possibility of lateral ligament complex. a fracture, but X-ray is negative. You diagnose a severe lateral Objective ligament sprain and manage Lucia with ice, a compression The aim of this article is to review the assessment and bandage and a backslab initially. She then progresses through management of sports ankle injuries in the general practice a 6 week rehabilitation program and you recommend she wear setting. an ankle brace for at least 6 months. Discussion Assessment of an ankle injury begins with a detailed history to determine the severity, mechanism and velocity of the injury, what happened immediately after and whether there is a past history of inadequately rehabilitated ankle injury. Examination involves assessment of weight bearing, inspection, palpation, movement, and application of special examination tests. Plain X-rays may be helpful to exclude a fracture. If the diagnosis is uncertain, consider second The majority of ankle injuries are inversion and plantar line investigations including bone scan, computerised flexion injuries that result in damage to the lateral tomography or magnetic resonance imaging, and referral to a ligament complex (Figure 1). -
Intramedullary Nailing for Femur Fracture Management a Guide for Parents
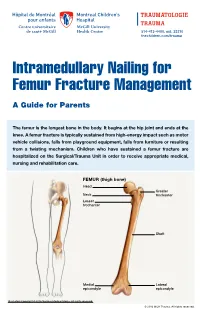
514-412-4400, ext. 23310 thechildren.com/trauma Intramedullary Nailing for Femur Fracture Management A Guide for Parents The femur is the longest bone in the body. It begins at the hip joint and ends at the knee. A femur fracture is typically sustained from high-energy impact such as motor vehicle collisions, falls from playground equipment, falls from furniture or resulting from a twisting mechanism. Children who have sustained a femur fracture are hospitalized on the Surgical/Trauma Unit in order to receive appropriate medical, nursing and rehabilitation care. FEMUR (thigh bone) Head Greater Neck trochanter Lesser trochanter Shaft Medial Lateral epicondyle epicondyle Illustration Copyright © 2016 Nucleus Medical Media, All rights reserved. © 2016 MCH Trauma. All rights reserved. FEMUR FRACTURE MANAGEMENT The pediatric Orthopedic Surgeon will assess your child in order to determine the optimal treatment method. Treatment goals include: achieving proper bone realignment, rapid healing, and the return to normal daily activities. The treatment method chosen is primarily based on the child’s age but also taken into consideration are: fracture type, location and other injuries sustained if applicable. Prior to the surgery, your child may be placed in skin traction. This will ensure the bone is in an optimal healing position until it is surgically repaired. Occasionally, traction may be used for a longer period of time. The surgeon will determine if this management is needed based on the specific fracture type and/or location. ELASTIC/FLEXIBLE INTRAMEDULLARY NAILING This surgery is performed by the Orthopedic Surgeon in the Operating Room under general anesthesia. The surgeon will usually make two small incisions near the knee joint in order to insert two flexible titanium rods (intramedullary nails) Flexible through the femur. -

Mcilroy's Ankle Injury Explained
McIlroy’s Ankle Injury Explained By Eva Nugent MISCP The Anterior Talofibular Ligament is big news this week because of world number 1 golf player Rory McIlroy’s injury sustained while having a football “kick about” with friends. McIlroy reports sustaining a “total rupture of his left ATFL and damage to the associated ankle joint capsule”. This unfortunate injury has put his golf season in doubt with the Open Championship starting just next week the 16th of July. But what exactly is the ATFL? And what does the rehabilitation for this injury involve? The Anterior Talofibular Ligament is one of three ligaments that make of the lateral ligament complex of the ankle joint. It originates at the fibular malleoulus of the lateral shin bone (fibula) and runs forward to and attaches to the Talus (ankle bone). The other two ligaments are the Posterior talofibular ligament (PTFL) and the Calcaneofibular ligament (CFL). The function of these ligaments is to provide stability and support to the ankle joint. The ATFL specifically prevents the anterior translation of the shin in relation to the foot/ankle. The ATFL is the most commonly injured ankle ligament and is most vulnerable when the foot is pointing downwards and inwards as the body’s centre of gravity rolls over the ankle (plantarflexed and inverted position). This is commonly described as “going over on your ankle”. It is commonly injured in sports like football or GAA where unpredictable fast turns or cutting movements are involved. This is referred to as an ankle sprain and results in damage to the fibres of the ligament as they are overstretched. -

ANTERIOR KNEE PAIN Home Exercises
ANTERIOR KNEE PAIN Home Exercises Anterior knee pain is pain that occurs at the front and center of the knee. It can be caused by many different problems, including: • Weak or overused muscles • Chondromalacia of the patella (softening and breakdown of the cartilage on the underside of the kneecap) • Inflammations and tendon injury (bursitis, tendonitis) • Loose ligaments with instability of the kneecap • Articular cartilage damage (chondromalacia patella) • Swelling due to fluid buildup in the knee joint • An overload of the extensor mechanism of the knee with or without malalignment of the patella You may feel pain after exercising or when you sit too long. The pain may be a nagging ache or an occasional sharp twinge. Because the pain is around the front of your knee, treatment has traditionally focused on the knee itself and may include taping or bracing the kneecap, or patel- la, and/ or strengthening the thigh muscle—the quadriceps—that helps control your kneecap to improve the contact area between the kneecap and the thigh bone, or femur, beneath it. Howev- er, recent evidence suggests that strengthening your hip and core muscles can also help. The control of your knee from side to side comes from the glutes and core control; that is why those areas are so important in management of anterior knee pain. The exercises below will work on a combination of flexibility and strength of your knee, hip, and core. Although some soreness with exercise is expected, we do not want any sharp pain–pain that gets worse with each rep of an exercise or any increased soreness for more than 24 hours. -
How to Self-Bandage Your Leg(S) and Feet to Reduce Lymphedema (Swelling)
Form: D-8519 How to Self-Bandage Your Leg(s) and Feet to Reduce Lymphedema (Swelling) For patients with lower body lymphedema who have had treatment for cancer, including: • Removal of lymph nodes in the pelvis • Removal of lymph nodes in the groin, or • Radiation to the pelvis Read this resource to learn: • Who needs self-bandaging • Why self-bandaging is important • How to do self-bandaging Disclaimer: This pamphlet is for patients with lymphedema. It is a guide to help patients manage leg swelling with bandages. It is only to be used after the patient has been taught bandaging by a clinician at the Cancer Rehabilitation and Survivorship (CRS) Clinic at Princess Margaret Cancer Centre. Do not self-bandage if you have an infection in your abdomen, leg(s) or feet. Signs of an infection may include: • Swelling in these areas and redness of the skin (this redness can quickly spread) • Pain in your leg(s) or feet • Tenderness and/or warmth in your leg(s) or feet • Fever, chills or feeling unwell If you have an infection or think you have an infection, go to: • Your Family Doctor • Walk-in Clinic • Urgent Care Clinic If no Walk-in clinic is open, go to the closest hospital Emergency Department. 2 What is the lymphatic system? Your lymphatic system removes extra fluid and waste from your body. It plays an important role in how your immune system works. Your lymphatic system is made up of lymph nodes that are linked by lymph vessels. Your lymph nodes are bean-shaped organs that are found all over your body.