Fourth and Final Joint Technical Reporting up to July 31 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Districts of Ethiopia
Region District or Woredas Zone Remarks Afar Region Argobba Special Woreda -- Independent district/woredas Afar Region Afambo Zone 1 (Awsi Rasu) Afar Region Asayita Zone 1 (Awsi Rasu) Afar Region Chifra Zone 1 (Awsi Rasu) Afar Region Dubti Zone 1 (Awsi Rasu) Afar Region Elidar Zone 1 (Awsi Rasu) Afar Region Kori Zone 1 (Awsi Rasu) Afar Region Mille Zone 1 (Awsi Rasu) Afar Region Abala Zone 2 (Kilbet Rasu) Afar Region Afdera Zone 2 (Kilbet Rasu) Afar Region Berhale Zone 2 (Kilbet Rasu) Afar Region Dallol Zone 2 (Kilbet Rasu) Afar Region Erebti Zone 2 (Kilbet Rasu) Afar Region Koneba Zone 2 (Kilbet Rasu) Afar Region Megale Zone 2 (Kilbet Rasu) Afar Region Amibara Zone 3 (Gabi Rasu) Afar Region Awash Fentale Zone 3 (Gabi Rasu) Afar Region Bure Mudaytu Zone 3 (Gabi Rasu) Afar Region Dulecha Zone 3 (Gabi Rasu) Afar Region Gewane Zone 3 (Gabi Rasu) Afar Region Aura Zone 4 (Fantena Rasu) Afar Region Ewa Zone 4 (Fantena Rasu) Afar Region Gulina Zone 4 (Fantena Rasu) Afar Region Teru Zone 4 (Fantena Rasu) Afar Region Yalo Zone 4 (Fantena Rasu) Afar Region Dalifage (formerly known as Artuma) Zone 5 (Hari Rasu) Afar Region Dewe Zone 5 (Hari Rasu) Afar Region Hadele Ele (formerly known as Fursi) Zone 5 (Hari Rasu) Afar Region Simurobi Gele'alo Zone 5 (Hari Rasu) Afar Region Telalak Zone 5 (Hari Rasu) Amhara Region Achefer -- Defunct district/woredas Amhara Region Angolalla Terana Asagirt -- Defunct district/woredas Amhara Region Artuma Fursina Jile -- Defunct district/woredas Amhara Region Banja -- Defunct district/woredas Amhara Region Belessa -- -

COUNTRY Food Security Update
ETHIOPIA Food Security Outlook Update September 2013 Crops are at their normal developmental stages in most parts of the country Figure 1. Projected food security outcomes, KEY MESSAGES September 2013 • Following the mostly normal performance of the June to September Kiremt rains, most crops are at their normally expected developmental stage. A near normal Meher harvest is expected in most parts of the country. However, in places where Kiremt rains started late and in areas where some weather-related hazards occurred, some below normal production is anticipated. • Market prices of most staple cereals remain stable at their elevated levels compared to previous months, but prices are likely to fall slightly starting in October due to the expected near normal Meher production in most parts of the country, which, in turn, will also improve household-level food access from October to December. Source: FEWS NET Ethiopia • Overall, current nutritional status compared to June/July has slightly improved or remains the same with exceptions in Figure 2. Projected food security outcomes, some areas in northeastern Tigray and Amhara Regions as October to December 2013 well as some parts of East Hararghe Zone in Oromia Region. In these areas, there are indications of deteriorating nutritional status due to the well below average Belg harvest and the current absence of a green harvest from long-cycle Meher crops. CURRENT SITUATION • Cumulative Kiremt rainfall from June to September was normal to above normal and evenly distributed in all of Southern Nations, Nationalities, and Peoples’ Region (SNNPR), in most parts of Amhara, in central and western parts Oromia, and in the central parts of Tigray. -

Species Composition, Relative Abundance and Habitat Association of Birds in Arbegona, Garemba Forest, Southern Ethiopia
Advances in Life Science and Technology www.iiste.org ISSN 2224-7181 (Paper) ISSN 2225-062X (Online) DOI: 10.7176/ALST Vol.75, 2019 Species Composition, Relative Abundance and Habitat Association of Birds in Arbegona, Garemba Forest, Southern Ethiopia Ziyad Jemal 1 Mustefa Sultan 2 1.Oromia Forest and Wildlife Enterprise, Ethiopia 2.Department of Forestry, College of Agriculture and Environmental Science, Arsi University, Asella, Ethiopia Abstract The present study was carried out in Arbegona Garemba forest from August June 2017 to February 2018 during wet and dry seasons. The study area was stratified based on vegetation composition. Accordingly, Modified habitat, Alpine bamboo forest, and Sub-Afro alpine /Ericaceous belt/ were considered. A line transects count aided by binocular was employed to investigate avian species diversity, relative abundance and Habitat association. Thus10 transect lines of 0.75km lengths with a width of 0.15km or less wereused to cover 30% of the area. A total of 74 bird species consisting of 5 near endemics, 2 globally threatened and 3 Palearctic migrants were recorded.Average vegetation height was a good predictor for total bird abundance and bird species richness during dry season. Altitude accounted more in total species richness and bird species abundance during wet season. Though, slope was a good predictor for bird species abundance during dry season. It can be concluded that the patch of forest and its surrounding is an important bird area for migratory, endemic, and global threatened species. Therefore, it should be conservation priority area; hence, the study suggests that conservation together with ecotourism development is needed for its sustainability. -

Determinants and Role of Farmers' Seed and Seedling
DETERMINANTS AND ROLE OF FARMERS’ SEED AND SEEDLING MULTIPLICATION IN THE SNNP REGION SEED SYSTEM M.Sc. Thesis GEZAHAGN WALELIGN April 2008 Haramaya University DETERMINANTS AND ROLE OF FARMERS’ SEED AND SEEDLING MULTIPLICATION IN THE SNNP REGION SEED SYSTEM A Thesis Submitted to the Department of Agricultural Economics, School of Graduate Studies Haramaya University In Partial Fulfillment of the Requirements for the Degree of MASTER OF SCIENCE IN AGRICULTURE (AGRICULTURAL ECONOMICS) By GEZAHAGN WALELIGN April 2008 Haramaya University ii School of Graduate Studies Haramaya University As Thesis Research advisor, I here by certify that I have read and evaluated this thesis prepared, under my guidance, by Gezahagn Walelign, entitled Determinants and Role of Farmers’ Seed and Seedling Multiplication in the SNNP Regional Seed System. I recommend that it be submitted as fulfillment of the Thesis requirement. Dawit Alemu(Ph D) ________________ _______________ Major Advisor Signature Date R.S.L.Srivastava (prof.) _________________ _______________ Co-advisor Signature Date As member of the Board of Examiners of the MSc Thesis Open Defense Examination, We certify that we have read, evaluated the Thesis prepared by Gezahagn Walelign and examined the candidate. We recommended that the Thesis is accepted as fulfilling the Thesis requirement for the Degree of Master of Science in Agriculture (Agricultural Economics). ______________________ _________________ _______________ Chairperson Signature Date ______________________ _________________ _______________ Internal Examiner Signature Date ______________________ _________________ _______________ External Examiner Signature Date iii DEDICATION I dedicated this thesis manuscript to my late wife Serkalem Chalachew whom I lost during my stay here for MSc. course and my beloved children Ruth and Tewodrose Gezahagn iv STATEMENT OF AUTHOR First, I declare that this thesis is the result of my own work and that all sources or materials used for this thesis have been duly acknowledged. -

October 27, 2005
Minutes of the 43rd Technical Information Management Exchange (TIME) Forum Meeting October 27,2005, 10:00 hrs DPPC Conference Room Chairperson: Ato Wegayehu Belew Agenda • Food Aid Task Force, Ato Mesfin Sheferaw • Situation Report, Early Warning Department (DPPC) • Food Aid Pipeline Report, World Food Programme (WFP) • EFSRA Stock Status Report, Ato Wegayehu Belew • AOB Food Aid Task Force: Ato Mesfin Sheferaw I. September Allocation and Dispatch Status by DPPC Region Allocation Dispatch (%) Afar 4,453.2 100 Amhara 1,903.7 100 Gambella 731.1 80 Oromia 12,823.6 100 Harari No beneficiaries SNNP Utilization report not submitted Somali Utilization report not submitted Tigray 4,520.3 90 Total 24,431.9 Due to late allocation to Tigray and Gambella Regions, dispatch for the month of September has not been completed. Meeting participants stated that withholding food aid allocation because of lack of utilization reports would be tantamount to punishing the needy. Therefore it was suggested that giving technical support to the concerned Regions on preparing utilization reports can be a solution. However the Disaster Prevention and Preparedness Agency (DPPA), taking note of the suggestion, assured concerned that for hot spot areas food aid is distributed with or out without utilization report. II. September Allocation and Dispatch Status by NGOs Region Allocation Oromia 8,033.82 Somali 1,263.00 SNN 951.7 DireDawa 596.04 Amhara 328.41 Afar 364.5 Tigray 6,690.76 Total 18,228.23 • FHI/ORDA has completed dispatch (Grain and Oil) • SC/UK has not transported the allocation to Dahana and Ziquala woreda in Amhara Region because woreda officials did not submit the beneficiary figure, which has decreased significantly from the previous months. -

Lippia Adoensis, Implication for Access and Benefit Sharing Agreement in Sidama and Westarsi Zones, SNNPR and Oromia Regions, Ethiopia
MOJ Ecology & Environmental Sciences Research Article Open Access Economic Valuation of Lippia adoensis, implication for Access and Benefit Sharing agreement in Sidama and WestArsi Zones, SNNPR and Oromia Regions, Ethiopia Abstract Volume 4 Issue 5 - 2019 Biodiversity has major economic value. Most of these values are often not captured by the market. Hence, the potential of biodiversity is often underestimated. Such an Amare Seifu, Tesfaye Bekele, Manaye underestimation is considered as one of the factors for rapid depletion of biodiversity Misganawand, Ashenafi Ayenew and loss of habitats and species. Valuation of bio-resources would facilitate in identifying Ethiopian Biodiversity Institute, Genetic Resources Access and the real value of genetic resources and obtaining a reasonably better share of the overall Benefit Sharing Directorate, Ethiopia benefits of genetic materials to the local communities, who are involved in its management. Accordingly, the Economic Valuation of Lippia adoensis was conducted implication for Correspondence: Amare Seifu, Ethiopian Biodiversity Institute, ABS. The result of this study identified the direct and indirect use values ofLippia adoensis. Genetic Resources Access and Benefit Sharing Directorate, Ethiopia, Tel +251916595709, Email Majority of the respondents (98.33%) were willing to pay for use values of Lippia adoensis. Moreover, (80.8%) of the respondents were willingness to pay for Conservation of Lippia Received: October 09, 2019 | Published: October 30, 2019 adoensis. Furthermore, 95(79.2%) of the respondents were willingness to pay for non-use value of Lippia adoensis in the study areas. The cumulative estimates of willingness to pay for use of values Lippia adoensis were 30,437.50 birr with an average annual willingness to pay of 253.64±275.63 birr for Lippia adoensis. -
Ecx Semi-Washedcoffee Contracts: Details And
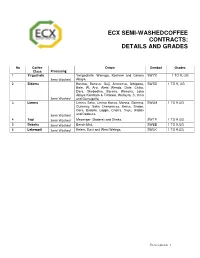
ECX SEMI -WASHED COFFEE CONTRACTS: DETAILS AND GRADES No Coffee Origin Symbol Grades Class Processing 1 Yir gachefe Yerigachefe, Wenago, Kochere and Gelana SWYC 1 TO 9, UG Semi Washed Abaya. 2 Sidama Borena, Benssa, Guji, Arroressa, Arbigona, SWSD 1 TO 9, UG Bale, W. Arsi. Aleta Wendo, Dale, Chiko, Dara, Shebedino, Borena, Wensho, Loko Abaya Kembata & Timbaro, Wellayta, S. Omo Semi Washed and Gamugoffa. 3 Limmu Limmu Seka, Limmu Kossa, Manna, Gomma, SWLM 1 TO 9,UG Gummay, Seka Chekoressa, Kersa, Shebe, Gera, Bedelle, Loppa, Chorra, Yayu, Alididu Semi Washed and Dedessa. 4 Tepi Semi Washed Mezenger (Godere) and Sheka. SWTP 1 TO 9,UG 5 Bebeka Semi Washed Bench Maji. SWBB 1 TO 9,UG 6 Lekempti Semi Washed Kelem, East and West Welega. SWLK 1 TO 9,UG _______________________________________________________________________________________________________________________________ ECX Contracts 1 ECX SEMI-WASHED COFFEE CONTRACTS: GRADES AND STANDARDS General requirements The moisture content of semi-washed coffee shall not be more than 11.5% by weight. DEFINITIONS Semi -washed Coffee Coffee that is pulped but unfermented. Cherries are washed and sorted as in the washed method but are not placed in the fermentation tanks. Moisture Content The moisture content, expressed on a wet weight bases, shall be determined using an approved moisture meter. Raw Value The sum of points of Shape & Make, Colour and Odour. Cup Quality Value The sum of points of Cup Cleanness, Acidity, Body and Flavour. Liquoring (Cup testing) The organoleptic examination of brewed coffee by professionals to determine acidity, body and flavor, detection of defects and characters. Cup Defect The number of cup defects out of five cups. -

Army Worm Infestation in SNNP and Oromia Regions As of 24 May
Army worm infestation in SNNP and Oromia Regions As of 24 May, some 8,368 hectares of belg cropland was reportedly destroyed by army worms in Wolayita zone of SNNPR - an area that suffered from late onset of the 2013 belg rains and subsequent heavy rains that damaged belg crops. The damage caused by the army worms will further reduce the expected harvest this season. Similar incidents were also reported from Boricha, Bona Zuria, Dara, Dale, Hawassa Zuria and Loko Abaya woredas of Sidama zone; Loma and Mareka woredas of Dawro zone (SNNPR), as well as from drought prone areas of East and West Hararge zones of Oromia Region; and quickly spreading to neighbouring areas. In Boricha woreda, for example, more than 655 hectares of belg cropland was destroyed in the course of one week, this is indicative of the speed that damage is being caused. Immediate distribution of spraying containers and chemicals to the farmers is required to prevent further loss of belg crops. For more information, contact: [email protected] Health Update The number of meningitis cases has gradually declined since the outbreak was declared in January. To date, 1,371 cases were reported from 24 woredas in five zones of SNNP and Oromia Regions. The Government, with support from health partners, is conducting a reactive vaccination in the affected areas, with 1, 678,220 people vaccinated so far. Next week, the number of people vaccinated during the Addis Ababa City Administration meningitis vaccination campaign, conducted from 20 to 26 May, will be released. Meanwhile, the number of kebeles reporting cases of Yellow Fever in South Ari, Benatsemay and Selmago woredas of South Omo zone, SNNPR, increased. -

Survey of Medicinal Plants Used to Treat Malaria by Sidama People of Boricha District, Sidama Zone, South Region of Ethiopia
Hindawi Publishing Corporation Evidence-Based Complementary and Alternative Medicine Volume 2016, Article ID 9690164, 9 pages http://dx.doi.org/10.1155/2016/9690164 Research Article Survey of Medicinal Plants Used to Treat Malaria by Sidama People of Boricha District, Sidama Zone, South Region of Ethiopia Solomon Asnake,1 Tilahun Teklehaymanot,2 Ariaya Hymete,3 Berhanu Erko,2 and Mirutse Giday2 1 Medicine and Health Science College, Hawassa University, P.O. Box 1560, Hawassa, Ethiopia 2Aklilu Lemma Institute of Pathobiology, Addis Ababa University, P.O. Box 1176, Addis Ababa, Ethiopia 3SchoolofPharmacy,AddisAbabaUniversity,P.O.Box1176,AddisAbaba,Ethiopia Correspondence should be addressed to Mirutse Giday; [email protected] Received 7 November 2015; Revised 10 January 2016; Accepted 26 January 2016 Academic Editor: Ulysses P. Albuquerque Copyright © 2016 Solomon Asnake et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In Ethiopia, malaria control has been complicated due to resistance of the parasite to the current drugs. Thus, new drugs are required against drug-resistant Plasmodium strains. Historically, many of the present antimalarial drugs were discovered from plants. This study was, therefore, conducted to document antimalarial plants utilized by Sidama people of Boricha District, Sidama Zone, South Region of Ethiopia. An ethnobotanical survey was carried out from September 2011 to February 2012. Data were collected through semistructured interview and field and market observations. Relative frequency of citation (RFC) was calculated and preference ranking exercises were conducted to estimate the importance of the reported medicinal plants in Boricha District. -

World Bank Document
Sample Procurement Plan (Text in italic font is meant for instruction to staff and should be deleted in the final version of the PP) Public Disclosure Authorized (This is only a sample with the minimum content that is required to be included in the PAD. The detailed procurement plan is still mandatory for disclosure on the Bank’s website in accordance with the guidelines. The initial procurement plan will cover the first 18 months of the project and then updated annually or earlier as necessary). I. General 1. Bank’s approval Date of the procurement Plan: Updated Procurement Plan, M 2. Date of General Procurement Notice: Dec 24, 2006 Public Disclosure Authorized 3. Period covered by this procurement plan: The procurement period of project covered from year June 2010 to December 2012 II. Goods and Works and non-consulting services. 1. Prior Review Threshold: Procurement Decisions subject to Prior Review by the Bank as stated in Appendix 1 to the Guidelines for Procurement: [Thresholds for applicable procurement methods (not limited to the list below) will be determined by the Procurement Specialist /Procurement Accredited Staff based on the assessment of the implementing agency’s capacity.] Public Disclosure Authorized Procurement Method Prior Review Comments Threshold US$ 1. ICB and LIB (Goods) Above US$ 500,000 All 2. NCB (Goods) Above US$ 100,000 First contract 3. ICB (Works) Above US$ 15 million All 4. NCB (Works) Above US$ 5 million All 5. (Non-Consultant Services) Below US$ 100,000 First contract [Add other methods if necessary] 2. Prequalification. Bidders for _Not applicable_ shall be prequalified in accordance with the provisions of paragraphs 2.9 and 2.10 of the Public Disclosure Authorized Guidelines. -

In Search of Shelter the Case of Hawassa, Ethiopia
In search of shelter The case of Hawassa, Ethiopia Emma Grant, Gemechu Desta, Yeraswork Admassie, Faraz Hassan, Sophie Stevens and Meheret Ayenew Working Paper Urban Keywords: January 2020 Urbanisation, Informal Settlements, Urban Poverty, Housing About the authors Emma Grant, senior expert, Social Development Direct Gemechu Desta, executive director, Econvalue Consult Yeraswork Admassie, former associate professor of sociology, Addis Ababa University Faraz Hassan, senior urban specialist, Social Development Direct Sophie Stevens, principal consultant, Social Development Direct Meheret Ayenew, senior public policy researcher Acknowledgements With special thanks to Kussia Bekele, senior civil society advisor and research assistant. All photos were taken by members of the Ethiopia research team. The research was funded by the UK Department for International Development’s East Africa Research Fund (EARF) and contributed to the EARF’s research programme: Shaping East African Cities as Systems to Work Better for All. This material has been funded by UK aid from the UK government. However, the views expressed do not necessarily reflect the UK government’s official policies. Produced by IIED’s Human Settlements group The Human Settlements Group works to reduce poverty and improve health and housing conditions in the urban centres of Africa, Asia and Latin America. It seeks to combine this with promoting good governance and more ecologically sustainable patterns of urban development and rural-urban linkages. About Econvalue Consult Econvalue Consult offers advanced policy research expertise on a range of social and economic topics. About Social Development Direct Social Development Direct (SDDirect) provides high-quality, innovative and expert social development assistance and research services. Published by IIED, January 2020 Grant, E, Desta, G, Admassie, Y, Hassan, F, Stevens, S and Ayenew, M (2019) In search of shelter: the case of Hawassa, Ethiopia. -

Assessment Report: IPMS – Farm Radio Participatory Agricultural Radio
Assessment Report: IPMS – Farm Radio Participatory Agricultural Radio Series’ in Ethiopia February, 2012 Evaluation report by: Eyob Mihretab (Development Consultant) Submitted To: IPMS / ILRI Submitted By: Farm Radio International Executive Summary In 2011, the Improving Productivity and Marketing Success (IPMS) project of the International Livestock Research Institute (ILRI) asked Farm Radio international to coordinate the planning and delivery of a series of radio programs related to two of the commodity value chains involved in IPMS: apiculture in the Tigray Region, and fruit tree production in Sidama. Farm Radio International accepted this invitation, and, after signing an agreement with ILRI-IPMS, proceeded with the development, implementation and evaluation of a new approach to agricultural radio: the Participatory Agricultural Radio Series – or PARS. The PARS was conceptualized as a weekly series of 6 episodes of 30-minute radio programs related to some aspect of the apiculture or fruit tree value chains. Planned with input from and the participation of intended beneficiaries, the PARS engages farmers as central players to design, develop and implement a series of radio programs around an agricultural practice they deem essential to their livelihoods and overall food security. It was anticipated that the PARS would be successful in raising the knowledge levels of communities reached by the programs, but that a 6-week series was probably inadequate to have a short-term measurable impact on the practices/behaviours of farmers. (FRI’s