Clinical Commissioning Group
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

74 Bus Time Schedule & Line Route
74 bus time schedule & line map 74 Rotherham - She∆eld View In Website Mode The 74 bus line (Rotherham - She∆eld) has 2 routes. For regular weekdays, their operation hours are: (1) Rotherham Town Centre <-> Waverley: 8:32 AM - 6:55 PM (2) Waverley <-> Rotherham Town Centre: 7:47 AM - 5:52 PM Use the Moovit App to ƒnd the closest 74 bus station near you and ƒnd out when is the next 74 bus arriving. Direction: Rotherham Town Centre <-> Waverley 74 bus Time Schedule 29 stops Rotherham Town Centre <-> Waverley Route VIEW LINE SCHEDULE Timetable: Sunday Not Operational Rotherham Interchange/B10, Rotherham Town Monday 8:32 AM - 6:55 PM Centre Tuesday 8:32 AM - 6:55 PM Corporation Street/Market Street, Rotherham Town Centre Wednesday 8:32 AM - 6:55 PM Corporation Street, Rotherham Thursday 8:32 AM - 6:55 PM Westgate/Unity Place, Rotherham Town Centre Friday 8:32 AM - 6:55 PM 28-32 Westgate, Rotherham Saturday 8:32 AM - 6:55 PM Canklow Road/Alma Road, Rotherham Town Centre Alma Road, Rotherham Canklow Road/Mill Street, Canklow 74 bus Info Direction: Rotherham Town Centre <-> Waverley Canklow Road/Jubilee Street, Canklow Stops: 29 Trip Duration: 21 min Canklow Road/Warden Street, Canklow Line Summary: Rotherham Interchange/B10, Rotherham Town Centre, Corporation Street/Market Canklow Road/Canklow Hill Road, Canklow Street, Rotherham Town Centre, Westgate/Unity Place, Rotherham Town Centre, Canklow Road/Alma Centenary Way/West Bawtry Road, Canklow Road, Rotherham Town Centre, Canklow Road/Mill Street, Canklow, Canklow Road/Jubilee Street, Bawtry -

NHS Rotherham GP Commissioning Localities - January 2011
NHS Rotherham GP Commissioning Localities - January 2011 PA Rep STUART LAKIN Central North GP Lead Other GP's with in the practice Practice Name Practice Manager Address Telephone List Size Kirsty Gillgrass Dr Everett, Brynes, Jones, Bhattacharya, Woodstock Bower Group PracticeBernadette Conway Kimberworth Road, Rotherham, South 0844 8151956 11524 Adrian Cole, Rihal, Saeed Yorkshire, S61 1AH Naresh PATEL Dr Stott, Martin, Cullen, Sanders, Kacker, Broom Lane Medical PracticeMartyn Heeley 70 Broom Lane, Rotherham, S60 3EW 0844 477 39 79 12574 George, Thomas Shrinivas Ravula Dr M Husain Greasbrough Medical Centre Claire Astbury Greasbrough, Greenside, Rotherham, South 01709 559955 3269 Yorkshire, S61 4PT Charles Collinson Dr Myers, Barragry, Evans Greenside Surgery Carole Dalling Munsbrough Rise, Greasborough, 0845 1240887 5187 Rotherham, South Yorkshire, S61 4RB Total 32554 PA Rep GOVINDER BHOGAL RICHARD RUSSELL Central Two Practice Practice Name Practice Manager Address Telephone List Size Tariq Ahmed Dr Nazir, Jubb, Ghaebi and Chikthimmah Kilnhurst Surgery Steve Hindle Magna Lane, Dalton, Rotherham, South 0845 1244746 7011 (Deputy) Yorkshire, S65 4HH Nayyer Ishaque Dr Iqbal Dalton Health Centre Angela Madden Magna Lane, Dalton, Rotherham, South 0845 1266430 2040 Yorkshire, S65 4HH Hilal Jarjis Badsley Moor Lane Surgery Julie Gibson 292 Badsley Moor Lane, Rotherham, South 0845 1222276 2464 Yorkshire, S65 2QW Saheel BATT Dr A Goni and Dr M S Chauhdry Shakespeare Road Surgery Diane Batham 50 Shakespeare Road, Eastwood, 0845 1213122 4879 -
Valid From: 01 September 2019 Bus Service(S) What's Changed Areas
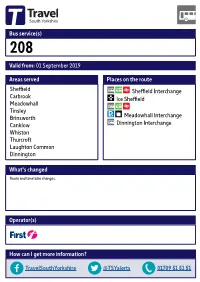
Bus service(s) 208 Valid from: 01 September 2019 Areas served Places on the route Sheffield Sheffield Interchange Carbrook Ice Sheffield Meadowhall Tinsley Brinsworth Meadowhall Interchange Canklow Dinnington Interchange Whiston Thurcroft Laughton Common Dinnington What’s changed Route and timetable changes. Operator(s) How can I get more information? TravelSouthYorkshire @TSYalerts 01709 51 51 51 Bus route map for service 208 01/02/2019 Scholes Parkgate Dalton Thrybergh Braithwell Ecclesfield Ravenfield Common Kimberworth East Dene Blackburn ! Holmes Meadowhall, Interchange Flanderwell Brinsworth, Hellaby Bonet Lane/ Bramley Wincobank Brinsworth Lane Maltby ! Longley ! Brinsworth, Meadowhall, Whiston, Worrygoose Lane/Reresby Drive ! Ñ Whitehill Lane/ Meadowhall Drive/ Hooton Levitt Bawtry Road Meadowhall Way 208 Norwood ! Thurcroft, Morthen Road/Green Lane Meadowhall, Whiston, ! Meadowhall Way/ Worrygoose Lane/ Atterclie, Vulcan Road Greystones Road Thurcroft, Katherine Road/Green Arbour Road ! Pitsmoor Atterclie Road/ Brinsworth, Staniforth Road Comprehensive School Bus Park ! Thurcroft, Katherine Road/Peter Street Laughton Common, ! ! Station Road/Hangsman Lane ! Atterclie, AtterclieDarnall Road/Shortridge Street ! ! ! Treeton Dinnington, ! ! ! Ulley ! Doe Quarry Lane/ ! ! ! Dinnington Comp School ! Sheeld, Interchange Laughton Common, Station Road/ ! 208! Rotherham Road 208 ! Aughton ! Handsworth ! 208 !! Manor !! Dinnington, Interchange Richmond ! ! ! Aston database right 2019 Swallownest and Heeley Todwick ! Woodhouse yright p o c Intake North Anston own r C Hurlfield ! data © y Frecheville e Beighton v Sur e South Anston c ! Wales dnan ! r O ! ! ! ! Kiveton Park ! ! ! ! ! ! Sothall ontains C 2019 ! = Terminus point = Public transport = Shopping area = Bus route & stops = Rail line & station = Tram route & stop 24 hour clock 24 hour clock Throughout South Yorkshire our timetables use the 24 hour clock to avoid confusion between am and pm times. -

Rotherham Primary Care Estates Strategy V8
Rotherham Clinical Commissioning Group gy Amended November 2020 Intentionally Left Blank Rotherham Primary Care Estates Strategy 1 1. EXECUTIVE SUMMARY 1. EXECUTIVE SUMMARY 6.4.2. Key Issues from Appraisal and Mapping 6.4.3. Central North Locality Estates Prioritisation 2. INTRODUCTION 6.5. Health Village / Central Locality 6.5.1. Property Assessment 3. STRATEGIC CONTEXT 6.5.2. Key Issues from Appraisal and Mapping 3.1. National Policy Context 6.5.3. Health Village / Central Locality Estate Prioritisation 3.2. Five Year Forward View 6.6. Maltby & Wickersley Locality 3.3. Delivering the Five Year Forward View 6.6.1. Premises Assessment 3.4. General Practice Forward View 6.6.2. Key Issues from Appraisal and Mapping 3.5. Next Steps on Five Year Forward View 6.6.3. Maltby & Wickersley Locality Estates Prioritisation 6.7. Wentworth South Locality 4. ROTHERHAM COMMISSIONING PRIORITIES, ORGANISATIONS AND 6.7.1. Premises Assessment STRATEGIC PARTNERS 6.7.2. Key Issues from Appraisal and Mapping 4.1. Health and Social Pen Picture of Rotherham 6.7.3. Wentworth South Locality Estates Prioritisation 4.1.1. Socio-economic Profile 6.8. Wath / Swinton Locality 4.1.2. Housing 6.8.1. Premises Assessment 4.1.3. Demographic Profile 6.8.2. Key Issues from Appraisal and Mapping 4.1.4. Health Needs 6.8.3. Wath / Swinton Locality Estates Prioritisation 4.2. Clinical Commissioning Groups 4.3. Local Authorities 7. FINANCIAL SUMMARY 4.4. Providers / Third Sector 4.5. South Yorkshire & Bassetlaw Integrated Care System (STP) 8. 2020 UPDATE 5. REVIEW OF THE PRIMARY CARE ESTATE ACROSS ROTHERHAM 5.1. -

Travel Advice for Pupils Of: WALES HIGH
School Bus Timetables and Travel Advice for pupils of: WALES HIGH SCHOOL 20112/132/13 ACADEMIC YEAR 1 Bus services to/from School School services are listed below and full timetables can be found on the following pages. Please note details are correct as at 9th July, should any changes take place prior to the start of term these will be communicated via the school. Service Route details Operator Number 632 Worksop – Lindrick – South Anston – School 633 South Anston - School 634 Norwood – Killamarsh – Upperthorpe – High Moor – Woodall – Harthill – School 635 Carlton - Gateford – Shireoaks – Netherthorpe - Thorpe Salvin – Harthill – School 636 Laughton village – Dinnington – North Anston – Todwick – School 637 School – Harthill – Todwick – North Anston – Dinnington – Thurcroft (LATE Bus) 638 Thurcroft – Brampton en le Morthen - School 639 Thurcroft – Laughton Common - School Other services which pass within 400 metres of the school are listed below and full timetables of these services are available from the Travel Information Centre in Rotherham, Sheffield or Dinnington Interchange or can be downloaded at www.travelsouthyorkshire.com/timetables . Service Route details Operator Number 27 Rotherham - Waterthorpe - Killamarsh - Norwood - School - Todwick - Dinnington 29 Rotherham – Swallownest – School – Harthill X5 Sheffield - Swallownest – School – South Anston – North Anston - Dinnington Operator Contact Details: BrightBus – 01909 550480 – www.brightbus.co.uk First – 01709 566000 – www.firstgroup.com/ukbus/south_yorkshire/ Should you need any further advice on anything in this pack then please call Traveline on 01709 515151. NB: SYPTE accept no responsibility for information provided on any other providers websites. 2 Service change details From September significant changes will be made to services to/from the school. -

INSPECTION REPORT SWALLOWNEST PRIMARY SCHOOL Swallownest, Sheffield LEA Area: Rotherham Unique Reference Number: 106860 Headteac
INSPECTION REPORT SWALLOWNEST PRIMARY SCHOOL Swallownest, Sheffield LEA area: Rotherham Unique reference number: 106860 Headteacher: Mrs S Hudson Reporting inspector: Mr S Hill 21277 Dates of inspection: 4th to 6th March 2002 Inspection number: 197736 Short inspection carried out under section 10 of the School Inspections Act 1996 © Crown copyright 2002 This report may be reproduced in whole or in part for non-commercial educational purposes, provided that all extracts quoted are reproduced verbatim without adaptation and on condition that the source and date thereof are stated. Further copies of this report are obtainable from the school. Under the School Inspections Act 1996, the school must provide a copy of this report and/or its summary free of charge to certain categories of people. A charge not exceeding the full cost of reproduction may be made for any other copies supplied. INFORMATION ABOUT THE SCHOOL Type of school: Infant and Junior School category: Community Age range of pupils: 3 to 11 Gender of pupils: Mixed School address: Rotherham Road Swallownest Sheffield South Yorkshire Postcode: S26 4UR Telephone number: 0114 287 2484 Fax number: 0114 287 6374 Appropriate authority: The governing body Name of chair of governors: Dr R U Watson Date of previous inspection: September 1997 Swallownest Primary School - 3 INFORMATION ABOUT THE INSPECTION TEAM Team members 21277 Mr S Hill Registered inspector 9056 Mrs V Cain Lay inspector 25352 Mrs G Taujanskas Team inspector The inspection contractor was: Evenlode Associates Ltd 6 Abbey Close Alcester Warwickshire B49 5QW Any concerns or complaints about the inspection or the report should be raised with the inspection contractor. -

Alpina Way, Swallownest Sheffield
Alpina Way, Swallownest Sheffield welcome to Alpina Way,Swallownest Sheffield GUIDE PRICE- £195,000- £205,000. A TARDIS! Beautifully presented and deceptively spacious throughout, this family property offers generously proportioned accommodation over three floors and enjoys a fine position within the heart of the popular Swallownest village. Not to be missed! Call now! Entrance Hall First Floor Landing Bedroom With front facing sealed unit door, central heating A spacious landing area with feature spotlights and 18' 1" max x 13' ( 5.51m max x 3.96m ) radiator and tiled floor. The entrance hall gives access to bedrooms two and three and the family Having two rear facing double glazed skylights access to the dining kitchen and has stairs rising to bathroom. There are side and a front facing double providing an abundance of natural light, this first floor accommodation. glazed windows, a central heating and feature wall bedroom is stylishly decorated and benefits from a art that extends from the ground floor to the second built in storage cupboard in addition to fitted floor staircase. The first floor landing also has stairs wardrobes providing ample storage. There are Dining Kitchen rising to the second floor master suite. feature spotlights, a central heating radiator and loft 18’ x 9' 7" (5.49m x 2.92m) hatch complete with loft ladders. The master A superb room featuring a modern range of bedroom also has internal door leading to the matching wall and base units with coordinating roll Bedroom Two master ensuite. edge surfaces housing the 1 1/2 bowl stainless steel 12' 5" x 13' 1" (3.78m x 3.99m) sink and drainer with mixer tap. -

Former County of South Yorkshire
Archaeological Investigations Project 2002 Post-Determination & Non-Planning Related Projects Yorkshire & Humberside Region FORMER COUNTY OF SOUTH YORKSHIRE Doncaster 3/1690 (E.04.J004) SK 49409600 FIRSBY HALL FARM, CONISBROUGH. An Archaeological Watching Brief at Firsby Hall Farm, Conisbrough. South Yorkshire Davies, G. Sheffield : ARCUS, 2002, 26pp, figs, tabs, refs Work undertaken by: ARCUS A watching brief was carried out on the site. No undisturbed deposits and no in situ structures were identified. There were numerous fragments of burnt clay probably from kilns, suggesting there presence nearby. These remains were identified as likely to be related to the medieval pottery production site previously identified in Firsby. [Au(adp)] Archaeological periods represented: MD 3/1691 (E.04.J002) SE 62000410 MARKHAM MAIN RESTORATION PROJECTS, DONCASTER Markham Main Restration Project. Doncaster, South Yorkshire Archaeological Services WYAS Morley : Archaeological Services WYAS, 2002, 16pp, pls, figs, refs Work undertaken by: Archaeological Services WYAS An archaeological watching brief was maintained during part of the landscaping for the Markham Main Restoration Project. The Groundworks proved to be less intrusive than expected and no features or deposits of an archaeological origin were identified. [Au(abr)] 3/1692 (E.04.H001) SE 53691203 ST HELENS CHURCH, BURGHWALLIS St Helen's Church, Burghwallis, South Yorkshire Dennison, E Beverley : Ed Dennison Archaeological Services, 2002, 21pp, colour pls, figs, tabs Work undertaken by: Ed Dennison Archaeological Services An archaeological watching brief was carried out on groundworks at the site. A pit was recorded containing a childs stone coffin, covered by two undecorated stone slabs. The remains of a slightly curved wall just to the north of the coffin was also observed. -

Parish Natter Parish Natter
Parish Natter A publication by ASTON-CUM-AUGHTON PARISH COUNCIL Issue No 65 Winter 2019 COMMENTS FROM THE CHAIRPERSON Welcome to the Winter issue of ‘Parish Natter’ we hope the information and articles included are of a general interest to parishioners. Bonfire and Fireworks Display – A very successful and well supported event took place on 6 November. My thanks go to staff, stewards, security and members who assisted and ensured visitors enjoyed the occasion in safety. Also, I would like to say a big ‘Thank You’ to ‘You’ our parishioners for your incredible support. .Christmas Decorations – The Parish Council has once again provided Christmas lights around the Parish, which, along with the Nativity displays provide a festive look to the area. The Nativity display at Swallownest was the venue for this year’s annual blessing organised by ‘Aston Churches Together’. Thanks go to our employees who have worked hard to ensure provision of the displays. Grit Bins – The grit bins provided by the Parish Council (green ones) in addition to those provided by the Borough Council (yellow ones) have now been put out ready for any inclement winter weather that comes our way. PLEASE NOTE the salt in these bins is for use on the highway only and not for use on private driveways. Bin Collections – For re-scheduled refuse and recycling bin collection days over the Christmas and New Year period – see page 10. Finally, on behalf of all Parish Councillors and staff, may I wish all the community of Aston-cum-Aughton a Merry Christmas and a prosperous New Year. -

Rotherham Unique Reference Number
INSPECTION REPORT CANKLOW WOOD PRIMARY SCHOOL Canklow, Rotherham, South Yorkshire LEA area: Rotherham Unique reference number: 131696 Headteacher: Mr A Clark Lead inspector: Mr J R Francis Dates of inspection: 8th March 2004 Inspection number: 255705 Inspection carried out under section 10 of the School Inspections Act 1996 © Crown copyright 2004 This report may be reproduced in whole or in part for non-commercial educational purposes, provided that all extracts quoted are reproduced verbatim without adaptation and on condition that the source and date thereof are stated. Further copies of this report are obtainable from the school. Under the School Inspections Act 1996, the school must provide a copy of this report and/or its summary free of charge to certain categories of people. A charge not exceeding the full cost of reproduction may be made for any other copies supplied. Canklow Wood Primary School - 2 INFORMATION ABOUT THE SCHOOL Type of school: Primary School category: Community Age range of pupils: 3 – 11 years Gender of pupils: Mixed Number on roll: 177 plus 17 part-time in the nursery School address: Wood Lane Canklow Rotherham South Yorkshire Postcode: S60 2XJ Telephone number: 01709 828405 Fax number: 01709 837873 Appropriate authority: Governing Body Name of chair of governors: Mrs M Sheard Date of previous inspection: 22nd March 1999 CHARACTERISTICS OF THE SCHOOL This average sized primary school has 177 pupils in six classes and 17 children who attend the nursery part-time. There are a similar number of boys and girls. The school also houses a Learning Centre funded through the Excellence in Cities project1. -

Nnfoi 200 Nd
NNFOI_ND Property Address Liable Party Contact Address Rateable Value C/O Capa Audit & Property Advisors, Audit ., Poplar Way, Catcliffe, Rotherham, South Yorkshire, Woolworths P L C - In Department, Po Box 29416, Glasgow, S60 5TR Administration G67 1XU £1,220,000.00 ., Greasbrough Street, Rotherham, South Yorkshire, Oakgate House, 25 Market Street, S60 1LQ Oakgate Rotherham Llp Wetherby, LS22 6LQ £377,500.00 Building 36, Meadows Road, Wath Upon Dearne, Rotherham, South Yorkshire, S63 5DJ Lazarus Properties Ltd 3 Lazarus Court, Doncaster, DN1 3NF £320,000.00 C/O C B Richard Ellis Portfolio Management , 2nd Floor , St Martin'S Town Mills, Canklow Road, Rotherham, South Court, 10 Paternoster Row, London, Yorkshire, S60 2JG Premier Foods Group Ltd EC4M 7HP £305,000.00 C/O Pendragon Plc - Property Dept, Loxley House, 2 Oakwood Court Little ., Great Eastern Way, Parkgate, Rotherham, South Andre Baldet Ltd T/A Evans Oak Drive, Annesley, Nottingham, NG15 Yorkshire, S62 6JD Halshaw 0DR £300,000.00 Unit 1 - Mansells, Adwick Park, Wath Upon Dearne, Cert Octavian House, St Martins Road, Rotherham, South Yorkshire, S63 5NB Cert Octavian Plc Hoddesdon, Herts, EN11 0BT £285,000.00 M F I Group Ltd (In C/O M C R, 43/45 Portman Square, Unit 9, Beale Way, Parkgate, Rotherham, S62 6EJ Administration) London, W1H 6LY £272,500.00 27 29, College Street, Rotherham, South Yorkshire, Nations House, 103 Wigmore Street, S65 1AG G E P (North) Ltd London, W1U 1QS £209,000.00 C/O Robert Smith Financial Management Warehouse, (Former Gloystarne Ltd), Don Street, The -

Strategic Green Belt Review April 2012
Rotherham local plan Rotherham Strategic Green Belt Review April 2012 www.rotherham.gov.uk Rotherham Strategic Green Belt Review Contents 1. Introduction & Need for the Study ....................................................................................................2 2. Aim of the Study..................................................................................................................................2 3. Scope....................................................................................................................................................3 4. Planning Policy Context .....................................................................................................................4 5. Methodology ........................................................................................................................................7 6. Strategic Green Belt Review : Informing Local Plan Preparation .............................................12 7. Results................................................................................................................................................13 8. Conclusion..........................................................................................................................................13 Appendix 1 – Methodology Consultation...............................................................................................15 Appendix 2 – Stage 2: Criteria to assess parcels against Green Belt purposes 1-4 .....................22 Appendix 3