Self-Funded Plan In-Network Disclosure
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
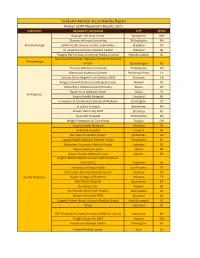
View 2021 Match Results
Graduate Medical Accountability Report Rowan SOM Placement Results 2021 SPECIALTY RESIDENCY PROGRAM CITY STATE Baystate Medical Center Springfield MA Thomas Jefferson University Philadelphia PA Anesthesiology SUNY Health Science Center at Brooklyn Brooklyn NY St. Josephs University Medical Center Paterson NJ Rutgers RW Johnson University Medical School New Brunswick NJ Hackensack Meridian Palisades University Medical Dermatology Center North Bergen NJ Thomas Jefferson University Philadelphia PA Memorial Healthcare System Pembroke Pines FL Carilion Clinic-Virginia Tech Carilion SOM Roanoke VA Rutgers Newark Beth Israel Medical Center Newark NJ Montefiore Medical Center/Einstein Bronx NY Baylor Univ Medical Center Dallas TX Emergency Inspira Health Network Vineland NJ University of Connecticut School of Medicine Farmington CT St Luke's Hospital Bethlehem PA Rowan University SOM Stratford NJ Nazareth Hospital Philadelphia PA Wright-Patterson Air Force Base Dayton OH Inspira Health Network Vineland NJ Overlook Hospital Summit NJ Bon Secours Health System Midlothian VA Capital Health Regional Medical Center Pennington NJ Hobocken University Medical Center Hoboken NJ Albany Medical Center Albany NY Crozer-Chester Medical Center Upland PA Rutgers Robert Wood Johnson Medical School- Centrastate Freehold NJ University of Texas Health San Antonio TX Penn State Hershey Medical Center Hershey PA Family Medicine Baylor College of Medicine Houston TX Bryn Mawr Hospital Bryn Mawr PA Christiana Care Newark DE Morristown Memorial Hospital Morristown NJ Rowan University SOM Stratford NJ Rutgers Robert Wood Johnson Medical School New Brunswick NJ Virtua Voorhees NJ NYP Hospital-Columbia University Medical Center New York NY Wright Center for GME Auburn WA Hunterdon Medical Center Flemington NJ Ocean Medical Center Brick NJ SPECIALTY RESIDENCY PROGRAM CITY STATE HCA Healthcare LGH-Montgomery/VCOM Blacksburg VA Kaiser Permanente-Fontana Fontana CA Lehigh Valley Hospital Allentown PA Palm Beach Consortium for GME Port St. -

Residency Match List 2021
PHILADELPHIA COLLEGE OF OSTEOPATHIC MEDICINE 2021 Residency List – Philadelphia Campus Anesthesiology (8) Family Medicine (con’t) Cook County Health and Hosp Sys, IL Jefferson Health - Northeast, PA (2) Hospital of the Univ of Pennsylvania, PA Lankenau Medical Center, PA Indiana University SOM, IN McLaren Health Care, MI Penn State Hershey Medical Center, PA Mike O'Callaghan Federal Hospital, Tower Health/Reading Hospital, PA (2) Nellis Air Force Base/Univ of Nevada UCLA Medical Center, CA School of Medicine, NV (2)* UPMC Pinnacle Hospitals, PA Naval Hospital Jacksonville, FL* NCC - Fort Belvoir Community Hosp, VA* Emergency Medicine (28) Northwestern McGaw Lake Forest, IL Albert Einstein Medical Center, PA (2) OhioHealth-Doctors Hospital, OH Capital Health Regional Medical Center, NJ OhioHealth-Grant Medical Center, OH Christiana Care, DE Penn Medicine-Lancaster General Hosp, PA CMSRU/Cooper University Hospital, NJ Penn State Hershey Medical Center, PA Crozer-Chester Medical Center, PA (3) Puyallup Tribal Health Authority, WA Florida Atlantic University Rowan University SOM, NJ (2) -Charles E. Schmidt COM, FL Rutgers-RWJUH Somerset, NJ Geisinger Health System, PA St. Lukes Hospital, PA Harbor-UCLA Medical Center, CA St. Lukes Hospital-Anderson, PA (2) HCA Healthcare/USF Morsani GME Suburban Community Hospital, PA -Oak Hill, FL Univ of Massachusetts Med School, MA Inspira Health Network, NJ (2) UPMC McKeesport, PA Jefferson Health - Northeast, PA (2) UPMC Presbyterian Shadyside, PA Jefferson Health NJ - Rowan SOM, NJ (2) UPMC Williamsport, -

Nemours/Alfred I. Dupont Hospital for Children Community Health Needs Assessment Implementation Plan
Nemours/Alfred I. duPont Hospital for Children Community Health Needs Assessment Implementation Plan Adopted on December 10, 2013 Wilmington, Delaware ©2013. The Nemours Foundation. Nemours is a registered trademark of The Nemours Foundation. 01195 Table of Contents About Nemours 2 Nutrition, Physical Activity & Weight 8 Access to Health Services 13 Mental & Emotional Health 20 Alcohol, Tobacco & Other Drugs 23 Health Education 25 Prenatal & Infant Health 32 Sexual Activity 34 Additional Efforts 35 1 About Nemours Nemours is the nation’s only integrated children’s health system, with two free-standing hospitals, Nemours/Alfred I. duPont Children’s Hospital in Wilmington, Del., and Nemours Children’s Hospital in Orlando, Fla. Nemours serves children and families from across the U.S. and other countries through 36 primary and specialty care clinics in Delaware, Florida, New Jersey and Pennsylvania. Nemours is putting its expertise to work in improving pediatric care in the Delaware Valley through coordinated patient- and family-centered care that includes medical services, biomedical research and graduate medical education, dedicated to a high standard of quality and safety outcomes. As a top tier, integrated children’s health system, Nemours continues to invest in addressing the needs of the whole child, connecting policy and prevention to the highest levels of specialized care for the most complex pediatric patients. Our mission at Nemours is to provide leadership, institutions and services to restore and improve the health of children. We do this through care and programs not readily available to children and families, and with one high standard of quality and distinction regardless of the recipient’s financial status. -

FACILITY IN-NETWORK DISCLOSURE Patient Name: Health Benefits Plan: • Inspira Heal
Inspira Health Center Bridgeton 333 Irving Avenue Bridgeton, New Jersey 08302 (856) 575-4500 www.inspirahealthnetwork.org FACILITY IN-NETWORK DISCLOSURE Patient name: _________________________ Health benefits plan: __________________ • Inspira Health is in-network for the health benefits plan named above and your financial responsibility to this facility will be no greater than your in-network copayment, deductible, and/or coinsurance amount. • You should contact the health care professional, such as your doctor, or the physician assistant or advance practice nurse who ordered the services, to determine if they are in•network or out-of-network for your health benefits plan. • In some cases, health care professionals other than the one ordering the service may provide and bill for care in this facility. You may expect services to be provided by any of the following groups: 1. Cooper University Hospital – Hospitalist Program* ALL INSPIRA SITES One Cooper Plaza, Dorrance Building Suite 237B Camden, NJ 08103 Contact: Lauren Simon – (856) 968-7449 2. Vineland/Bridgeton/Elmer ER Physicians* South Jersey Health System Emergency Physician Services c/o TeamHealth PO Box 7975 Lancaster, PA 17604-7975. National Patient Call Center: 888-952-6772 3. Mullica Hill ER Physicians* Emergency Care Services of NJ PA c/o TeamHealth PO Box 636086 Cincinnati, Ohio 45263-6086 National Patient Call Center: 888-952-6772 4. Mullica Hill Anesthesia Group South Jersey Anesthesia and Pain Physicians IMCMH - Dept. of Anesthesiology 700 Mullica Hill Road Mullica Hill, NJ Mark Cooper - [email protected] (856-508-1000 Ext. 81268) Inspira Health Center Bridgeton 333 Irving Avenue Bridgeton, New Jersey 08302 (856) 575-4500 www.inspirahealthnetwork.org 5. -

2020 New Jersey Provider Directory Directorio De Proveedores De New Jersey
34144908 2020 New Jersey Provider Directory Directorio de Proveedores de New Jersey This directory is updated as of 9/5/2020. Cape May, Cumberland, Gloucester, Salem CAD_63716M State Approved 10152019 ©WellCare 2020 NJ0JMDDIR63716M_0006 34144908 34144908 TABLE OF CONTENTS Provider Directory Introduction ......................................................................................................................................................................................................... I How to Read Our Provider Listings .......................................................................................................................................................... II Icon Guide ............................................................................................................................................................................................................ II List of Plan Providers Primary Care Physicians Cape May .........................................................................................................................................................................................................1 Cumberland ...................................................................................................................................................................................................5 Gloucester .................................................................................................................................................................................................... -

Inspira Health Network Community Health Needs Assessment 2019-2020-2021
Inspira Health Network Community Health Needs Assessment 2019-2020-2021 The size of each word represents the frequency of use in the transcripts of focus groups and interviews. 1 I. Introduction II. Community Health Needs Assessment: Community Context III. Community Health Needs Assessment: Process and Methods IV. Community Health Needs Assessment: Findings Theme 1: Obesity Theme 2: Substance Abuse Theme 3: Mental & Behavioral Health Theme 4: Access to Clinical Care Theme 5: Transportation Theme 6: Existing Strengths Emergency Room Findings V. Community Health Needs Assessment: Community Voice VI. Community Health Needs Assessment: Dissemination Plan VII. Community Health Needs Assessment: Prioritization VIII. Then and Now: Evaluating the Progress Made in Addressing Previous Priority Areas IX. Appendices Appendix A: Selected Expanded Survey Responses Appendix B: Research Tools 2 I. Introduction of how we integrated the community voice into the CHNA (Section This report provides a summary of the findings of the Community Health V), a plan for the dissemination of the current CHNA (Section VI), an Needs Assessment (CHNA) for Gloucester, Cumberland, and Salem explanation of how health needs were prioritized (Section VII), and an Counties; the CHNA was conducted by The Walter Rand Institute for evaluation of how Inspira Health Network has integrated the results Public Affairs (WRI) at Rutgers University-Camden on behalf of Inspira of the previous CHNA (Section VIII). The demographics of survey Health Network. participants are included in the process and methods section (Section III). We conducted the CHNA with one main goal: fulfilling the IRS requirements for tax-exempt hospitals by carefully characterizing Note to community members: The Findings Section (Section community members’ views on the health needs in their communities. -

Department of Cardiovascular Disease/Cooper Heart Institute
Cooper Heart Institute | DEPARTMENT OF CARDIOVASCULAR DISEASE DISEASE / Cooper Heart Institute OF CARDIOVASCULAR DEPARTMENT __________________________________________________________________________________________ Philip A. Koren, MD, Medical Director, Cooper Heart Institute Fredric L. Ginsberg, Co-Medical Director, Cooper Heart Institute Perry J. Weinstock, MD, Head, Division of Cardiology Division Office: Administrative Contact: One Cooper Plaza Carol Dempsey Third Floor/Dorrance t. (856) 342-2448 Camden, NJ 08103 f. (856) 361-1278 As of January 2017, Cooper University Health Care and Inspira Health Network have integrated the cardiac service lines from both organizations to form a new collaborative called Cardiac Partners at Cooper and Inspira. Scheduling for Office Appointments & Diagnostic Studies at offices listed below: 1.800.8.COOPER • CAMDEN • VOORHEES Three Cooper Plaza, Suites 311 & 318 The Ripa Center for Women’s Health Camden, NJ 08103 and Wellness at Cooper t. (856) 342-2683 6100 Main Street Complex f. (856) 342-6608 901 Centennial Boulevard (GPS Address) Voorhees, NJ 08043 • CHERRY HILL t. (856) 673-4912 1210 Brace Road, Suite 103 f. (856) 673-4497 Cherry Hill, NJ 08034 t. (856) 938-2052 • WASHINGTON TWP. f. (856) 795-2284 400 Medical Center Drive • EGG HARBOR TWP. Suite B 303 Central Ave., Suite 4 Sewell, NJ 08080 Egg Harbor Twp., NJ 08234 t. (856) 374-5820 t. (856) 536-1810 f. (856) 374-3120 f. (856) 536-1815 • WOODSTOWN 66 East Avenue • VOORHEES First Floor, Suite A 900 Centennial Blvd., Building 2, Suite 201 Woodstown, NJ 08098 Voorhees, NJ 08043 t. (856) 935-6700 t. (856) 325-6700 f. (856) 935-6772 f. (856) 325-6702 • WILLINGBORO 218C Sunset Road (Take Hospital Drive) Willingboro, NJ 08046 t. -

School of Osteopathic Medicine Graduate School of Biomedical Sciences
school of osteopathic medicine graduate school of biomedical sciences MAY 2020 Commencement 2020 3 More than Four Decades of Achievement, Service and Excellence 5 Improving Health Through Science 7 Commencement Ceremony 8 The Osteopathic Oath 8 Alma Mater 9 GRADUATE SCHOOL OF BIOMEDICAL SCIENCES Candidates for Graduation 11 SCHOOL OF OSTEOPATHIC MEDICINE Candidates for Graduation 14 SCHOOL OF OSTEOPATHIC MEDICINE Residency Location & Medical Specialty 22 Award Recipients 23 The Gonfalons 24 School of Osteopathic Medicine and Graduate School of Biomedical Sciences Administration COMMENCEMENT 2020 2 SCHOOL OF OSTEOPATHIC MEDICINE More than Four Decades of Achievement, Service and Excellence n 1976, the legislation to create a new medical Ischool in South Jersey was met with opposition from some who did not see the need for a third medical school in the state. But thanks to the energy and persistence of Sen. Joseph Maressa, Dr. Howard Levine and Dr. Joseph Riley, the legislation to create SOM was signed by Gov. Brendan Byrne. The inaugural class of 24 future physicians began their careers the following year at New Jersey’s only osteopathic medical school and the first four-year medical school in South Jersey. In 1986, SOM’s second decade welcomed the establishment of the New Jersey Institute In 1976, Gov. Brendan Byrne signed the Senate bill authorizing for Successful Aging (then called the Center In 1976, Gov. Brendan Byrne signed the Senate bill funding to create the School of Osteopathic Medicine in for Aging). A statewide center of excellence, authorizing funding to create the School of Osteopathic Stratford. From left, witnesses at the signing included the NJISA is dedicated to training health care Medicine in Stratford. -
2020-2021 Post Graduate Medical Education Brochure
2020 --2021 Postgraduate Medical Education Our mission: To Serve. To Heal. To Educate. Mission Our mission is To Serve. To Heal. To Educate. We accomplish our mission through innovative and effective systems of care and by bringing people and resources together, creating value for our patients and the community. Vision Cooper University Health Care will be the premier health care provider in the region, driven by our exceptional people delivering a world-class patient experience, one patient at a time, and through our commitment to educating the providers of the future. Contents Welcome Letter 1 Discover the Difference 2 Find Your Specialty 3 Explore Our Campus 4 Train in the Area’s Top Hospital 5 Delve Into Specialty Services 6 Venture Beyond the Hospital Walls 7 Enhance Your Learning Experience 8 Enjoy the Benefits 9 Residency/Fellowship Contact Information 10 Learn More 12 1887 First two residents 1889 Camden Training 1920 Dr. Vincent Del 1923 New children’s 1926 First motor at Cooper. School for Nurses Duca began ward opened. ambulance opened. pediatric residency to replace at Cooper. horse-drawn transportation. Welcome Cooper University Health Care takes pride in its ability to offer a comprehensive array of diagnostic and treatment services Cooper University Hospital serves as southern New Jersey’s major tertiary care referral hospital for specialized services Cooper Premier Institutes, Centers of Excellence, and programs include: MD Anderson Cancer Center at Cooper, Surgical Services Institute, Adult Health Institute, Cooper Heart -
Inspira Health Network, Inc
Inspira Health Network, Inc. Consolidated Financial Statements and Supplementary Information December 31, 2018 and 2017 Inspira Health Network, Inc. Table of Contents December 31, 2018 and 2017 Page Independent Auditors’ Report 1 Consolidated Financial Statements Consolidated Balance Sheets 3 Consolidated Statements of Operations and Changes in Net Assets 5 Consolidated Statements of Cash Flows 7 Notes to Consolidated Financial Statements 8 Supplementary Information Consolidating Schedules for 2018: Consolidating Schedule, Balance Sheet, including Balance Sheet for the Inspira Health Network Obligated Group 34 Consolidating Schedule, Statement of Operations and Changes in Net Assets, including Statement of Operations and Changes in Net Assets for the Inspira Health Network Obligated Group 35 Consolidating Schedules for 2017: Consolidating Schedule, Balance Sheet, including Balance Sheet for the Inspira Health Network Obligated Group 36 Consolidating Schedule, Statement of Operations and Changes in Net Assets, including Statement of Operations and Changes in Net Assets for the Inspira Health Network Obligated Group 37 Independent Auditors’ Report Board of Directors Inspira Health Network, Inc. Report on the Consolidated Financial Statements We have audited the accompanying consolidated financial statements of Inspira Health Network, Inc. (the "Network"), which comprise the consolidated balance sheets as of December 31, 2018 and 2017, and the related consolidated statements of operations and changes in net assets, and cash flows for the -

House Calls Brochure
Rowan Medicine House Calls currently serves the following communities: Mount Laurel Cherry Hill Stratford Please call 609-704-0106 for more information. House Calls Program Rowan Medicine health care providers are faculty members of the Rowan University School of Osteopathic Medicine. Kennedy Health is the principal hospital of Rowan Medicine. Other affiliated hospitals and health systems include: Lourdes Health System Inspira Health Network Cooper University Hospital Meridian Health System Christ Hospital and Atlantic Health System 9/16 rowanmedicine.com 609-704-0106 Rowan Medicine House Calls brings your health care provider to your home. We know that going to see patients where they live – in their own home – is good medicine. Our health care team will provide comprehensive, continuing care all in the comfort of the patient’s home. During the home visit, our physicians and nurse practitioners provide personalized attention to the patient, which is particularly important for patients with chronic illnesses or other health problems, as well as those who have experienced a recent hospitalization. How do House Calls differ from Services Do I qualify? office visits? The House Calls health care team provides You can qualify for House Calls if you House calls allow us to get to know our ongoing primary care and follow-up visits to cannot leave home without considerable patients, their home, their families and homebound patients. Services include: taxing effort. Some examples include: caregivers. We interact with home health nurses and other therapists involved in • In-home full medical evaluation • You require the aid of supportive the patient’s care when necessary. -

Alphabetical Index of Active Clients
PART III ALPHABETICAL INDEX OF REPRESENTED ENTITIES AND THEIR GOVERNMENTAL AFFAIRS AGENTS BY REGISTRATION NUMBER FOR THE SECOND QUARTER OF 2013 Represented Entity Name Registration Number 1500 Harbor Boulevard Partners LLC 1825 1868 Public Affairs LLC 1054 1868 Public Affairs/Wal-Mart 1666 21st Century Frontier Group Inc 337 21st Century Oncology 721 3419 Route 46 LLC 1741 346 Ridgefield Management LLC 939 3M Company 1966 431 Corp 721 650 Union Boulevard LLC 1234 7-Eleven Inc 433 92 Now 1607 AAA Clubs of NJ 1781 AARP NJ 1222 Abba/Clemente LLC 1786 Abbott Laboratories Inc 1479 ABC Bail Bonds 721 AbTech Industries 365 AC Beach Development Partners LLC 365 AC Nightlife LLC d/b/a Dusk 1510 Academy Express LLC** 1603 Access NJ 721 ACCESS NJ 1380 ACE Group - North America 721 ACE Group - North America 1920 Acelero Inc 365 ACLU of New Jersey 1618 ACRA Turf Club LLC 173 ** New Represented Entity included during this quarter Page 1 of 87 PART III ALPHABETICAL INDEX OF REPRESENTED ENTITIES AND THEIR GOVERNMENTAL AFFAIRS AGENTS BY REGISTRATION NUMBER FOR THE SECOND QUARTER OF 2013 Represented Entity Name Registration Number Actavis 2001 Actavis Inc 1234 Action Environmental Services 721 Acumark Inc 1895 Adam Levy/Demand Pooling Global Services 433 ADP Claims Services Group 1000 ADP Total Source 433 ADV LLC 2001 Advanced Drainage Systems Inc 365 Advanced Drainage Systems Inc 1745 Advocates for Children of NJ 365 Advocates for Children of NJ (ACNJ) 797 Aes/Red Oak 463 Aetna 1720 Aetna Health Inc 1832 Affiliated Computer Services Inc A Xerox Company