Human USP18 Deficiency Underlies Type 1 Interferonopathy Leading to Severe Pseudo-TORCH Syndrome Marije E.C
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Co-Opted ISG15-USP18 Binding Mechanism Normally Reserved for Deisgylation Controls Type I IFN Signalling
bioRxiv preprint doi: https://doi.org/10.1101/2021.06.01.446527; this version posted June 3, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. 1 A co-opted ISG15-USP18 binding mechanism normally reserved for deISGylation controls 2 type I IFN signalling 3 4 5 6 Andri Vasou1, Katie Nightingale2, Vladimíra Cetkovská 1, Connor G.G. Bamford3‡, Jelena 7 Andrejeva1, Richard E. Randall1, John McLauchlan3, Michael P. Weekes2, David J Hughes1* 8 9 10 11 1Biomedical Sciences Research Complex, School of Biology, University of St Andrews, St 12 Andrews, United Kingdom. 2Cambridge Institute for Medical Research, Hills Road, Cambridge, 13 United Kingdom 3MRC-University of Glasgow Centre for Virus Research, Glasgow, United 14 Kingdom. 15 16 17 ‡ Present addresses: Wellcome-Wolfson Institute for Experimental Medicine, Queen’s 18 University, Belfast UK. 19 20 21 22 * Corresponding author: [email protected]; Tel: +44 1334 467197 23 1 bioRxiv preprint doi: https://doi.org/10.1101/2021.06.01.446527; this version posted June 3, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. 24 Abstract 25 Type I interferon (IFN) signalling induces the expression of several hundred IFN-stimulated 26 genes that provide an unfavourable environment for viral replication. -

Type I IFN Signaling Infection by Up-Regulating Typhimurium
Enhanced Antibacterial Potential in UBP43-Deficient Mice against Salmonella typhimurium Infection by Up-Regulating Type I IFN Signaling This information is current as of September 24, 2021. Keun Il Kim, Oxana A. Malakhova, Kasper Hoebe, Ming Yan, Bruce Beutler and Dong-Er Zhang J Immunol 2005; 175:847-854; ; doi: 10.4049/jimmunol.175.2.847 http://www.jimmunol.org/content/175/2/847 Downloaded from References This article cites 45 articles, 21 of which you can access for free at: http://www.jimmunol.org/content/175/2/847.full#ref-list-1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication by guest on September 24, 2021 *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2005 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Enhanced Antibacterial Potential in UBP43-Deficient Mice against Salmonella typhimurium Infection by Up-Regulating Type I IFN Signaling1 Keun Il Kim,2* Oxana A. Malakhova,* Kasper Hoebe,† Ming Yan,* Bruce Beutler,† and Dong-Er Zhang3* ISG15 is an IFN-inducible ubiquitin-like protein and its expression and conjugation to target proteins are dramatically induced upon viral or bacterial infection. -

Genesis of Non-Coding RNA Genes in Human Chromosome 22—A Sequence Connection with Protein Genes Separated by Evolutionary Time
non-coding RNA Perspective Genesis of Non-Coding RNA Genes in Human Chromosome 22—A Sequence Connection with Protein Genes Separated by Evolutionary Time Nicholas Delihas Department of Microbiology and Immunology, Renaissance School of Medicine, Stony Brook University, Stony Brook, New York, NY 11794-5222, USA; [email protected] Received: 16 July 2020; Accepted: 1 September 2020; Published: 3 September 2020 Abstract: A small phylogenetically conserved sequence of 11,231 bp, termed FAM247, is repeated in human chromosome 22 by segmental duplications. This sequence forms part of diverse genes that span evolutionary time, the protein genes being the earliest as they are present in zebrafish and/or mice genomes, and the long noncoding RNA genes and pseudogenes the most recent as they appear to be present only in the human genome. We propose that the conserved sequence provides a nucleation site for new gene development at evolutionarily conserved chromosomal loci where the FAM247 sequences reside. The FAM247 sequence also carries information in its open reading frames that provides protein exon amino acid sequences; one exon plays an integral role in immune system regulation, specifically, the function of ubiquitin-specific protease (USP18) in the regulation of interferon. An analysis of this multifaceted sequence and the genesis of genes that contain it is presented. Keywords: de novo gene birth; gene evolution; protogene; long noncoding RNA genes; pseudogenes; USP18; GGT5; Alu sequences 1. Introduction The genesis of genes has been a major topic of interest for several decades [1,2]. One mechanism of gene formation is by duplication of existing genes [1,3]. -

USP18 Is a Key Regulator of the Interferon-Driven Gene Network Modulating Pancreatic Beta Cell Inflammation and Apoptosis
Citation: Cell Death and Disease (2012) 3, e419; doi:10.1038/cddis.2012.158 & 2012 Macmillan Publishers Limited All rights reserved 2041-4889/12 www.nature.com/cddis USP18 is a key regulator of the interferon-driven gene network modulating pancreatic beta cell inflammation and apoptosis I Santin*,1, F Moore1, FA Grieco1, P Marchetti2, C Brancolini3 and DL Eizirik1 Type 1 diabetes (T1D) is an autoimmune disease targeting pancreatic beta cells. Genome-wide association studies and gene expression analysis identified interferon (IFN)-driven gene networks as crucial pathways in the pathogenesis of T1D. IFNs are linked to the response to viral infections and might contribute to the initiation of the autoimmune process in T1D. We presently analyzed the role of ubiquitin-specific peptidase 18 (USP18), an interferon-stimulated gene 15-specific protease, on IFN-induced pancreatic beta cell inflammation and apoptosis. Our findings indicate that USP18 inhibition induces inflammation by increasing the STAT signaling and exacerbates IFN-induced beta cell apoptosis by the mitochondrial pathway of cell death. USP18 regulates activation of three BH3-only proteins, namely, DP5, Bim and PUMA in pancreatic beta cells, suggesting a direct link between regulators of the type I IFN signaling pathway and members of the BCL-2 family. USP18 depletion increases the expression of the T1D candidate gene MDA5, leading to an upregulation of double-stranded RNA-induced chemokine production. These data suggest a cross talk between the type I IFN signaling pathway and a candidate gene for T1D to increase pro-inflammatory responses in beta cells. The present study shows that USP18 is a key regulator of IFN signaling in beta cells and underlines the importance of this pathway in beta cell inflammation and death. -

STAT2 Is an Essential Adaptor in USP18-Mediated Suppression of Type I Interferon Signaling
ARTICLES STAT2 is an essential adaptor in USP18-mediated suppression of type I interferon signaling Kei-ichiro Arimoto1,8, Sara Löchte2,8, Samuel A Stoner1, Christoph Burkart1, Yue Zhang3, Sayuri Miyauchi1, Stephan Wilmes2, Jun-Bao Fan1, Jürgen J Heinisch2, Zhi Li4, Ming Yan1, Sandra Pellegrini4, Frédéric Colland5,7, Jacob Piehler2 & Dong-Er Zhang1,3,6 Type I interferons (IFNs) are multifunctional cytokines that regulate immune responses and cellular functions but also can have detrimental effects on human health. A tight regulatory network therefore controls IFN signaling, which in turn may interfere with medical interventions. The JAK–STAT signaling pathway transmits the IFN extracellular signal to the nucleus, thus resulting in alterations in gene expression. STAT2 is a well-known essential and specific positive effector of type I IFN signaling. Here, we report that STAT2 is also a previously unrecognized, crucial component of the USP18-mediated negative-feedback control in both human and mouse cells. We found that STAT2 recruits USP18 to the type I IFN receptor subunit IFNAR2 via its constitutive membrane-distal STAT2-binding site. This mechanistic coupling of effector and negative-feedback functions of STAT2 may provide novel strategies for treatment of IFN-signaling-related human diseases. Type I interferon (IFN) signaling has emerged as a highly complex thereby resulting in formation of the DNA-binding STAT1–STAT2– regulatory network coordinating the host’s defense against pathogens IRF9 ternary complex IFN-stimulated gene factor 3 (ISGF3). ISGF3 and cancer via expression of over 300 IFN-stimulated genes (ISGs)1,2. promotes expression of genes with an IFN-stimulated response ele- Proteins encoded by ISGs include cytokines and chemokines that mod- ment in their promoters12,13. -

Type I IFN Is Siloed in Endosomes BRIEF REPORT Jennie B
Type I IFN is siloed in endosomes BRIEF REPORT Jennie B. Altmana, Justin Tafta, Tim Wedekingb, Conor N. Grubera, Michael Holtmannspötterb,c, Jacob Piehlerb,d, and Dusan Bogunovica,e,f,g,1 aDepartment of Microbiology, Icahn School of Medicine at Mount Sinai, New York, NY 10029; bDivision of Biophysics, Department of Biology, Osnabrück University, 49076 Osnabrück, Germany; cIntegrated Bioimaging Facility, Osnabrück University, 49076 Osnabrück, Germany; dCenter for Cellular Nanoanalytics, Osnabrück University, 49076 Osnabrück, Germany; eDepartment of Pediatrics, Icahn School of Medicine at Mount Sinai, New York, NY 10029; fPrecision Immunology Institute, Icahn School of Medicine at Mount Sinai, New York, NY 10029; and gMindich Child Heath and Development Institute, Icahn School of Medicine at Mount Sinai, New York, NY 10029 Edited by Tak W. Mak, University of Toronto, Toronto, ON, Canada, and approved June 16, 2020 (received for review December 6, 2019) Type I IFN (IFN-I) is thought to be rapidly internalized and degraded ISGs in ISG15- and USP18-deficient cells, but not control cells following binding to its receptor and initiation of signaling. How- (Fig. 1B). Thus, transcription occurs long after the elimination of ever, many studies report the persistent effects mediated by IFN-I IFN-I in ISG15- and USP18-deficient cells. for days or even weeks, both ex vivo and in vivo. These long- We investigated molecules acting farther upstream and de- lasting effects are attributed to downstream signaling molecules tected pSTAT1 and pSTAT2 (mediators of IFN-I proximal sig- or induced effectors having a long half-life, particularly in specific naling) (9) in ISG15- and USP18-deficient cells, but not control cell types. -

USP18 Is Differentially Expressed in SARS and MERS Coronavirus
1 USP18 is differentially expressed in SARS and MERS coronavirus infection models. 2 Shahan Mamoor1 1Thomas Jefferson School of Law 3 East Islip, NY 11730 4 [email protected] 5 COVID19 is caused by infection with the seventh virus of the coronavirus family capable of infecting humans, now known as Severe Acute Respiratory Syndrome 2, or SARS-CoV-2 (1-3). 6 We mined published and public microarray data from coronavirus infection models to identify genes whose expression changed most significantly following infection with coronaviruses 7 (4-9). In two in vivo mouse models of SARS coronavirus infection, the ubiquitin-specific 8 protease USP18 was among the genes whose expression changed most significantly in the lungs of mice infected with SARS-CoV-1. In the blood of ferrets after intranasal infection with 9 SARS-CoV-1, and in human cells in vitro after infection with the Middle Eastern Respiratory Syndrome (MERS) coronavirus, Usp18 was also found to be differentially expressed when 10 compared to mock-infected tissues or uninfected cells. Differential expression of Usp18 following infection with coronaviruses can be observed in experimental models in vivo and in 11 vitro, and across species. 12 13 14 15 16 17 18 19 20 21 22 23 24 Keywords: COVID19, Usp18, SARS-CoV-2, systems biology of viral infection, coronaviruses. 25 26 27 28 1 OF 18 1 Coronavirus infection is a global health crisis (2) and over 80,000 people in the United 2 States have thus far lost their lives after infection with the novel coronavirus SARS-CoV-2 (10). -

Negative Regulation of ACE2 by Interferons in Vivo and Its Genetic Control
medRxiv preprint doi: https://doi.org/10.1101/2020.04.26.20080408; this version posted June 8, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-NC-ND 4.0 International license . Negative regulation of ACE2 by interferons in vivo and its genetic control M. Azim Ansari1,2,3,4*, Emanuele Marchi1,2,3*, Narayan Ramamurthy1,2,3*, Dominik Aschenbrenner1,3, Carl-Philipp Hackstein2, STOP-HCV consortium, ISARIC-4C Investigators, Shang-Kuan Lin4, Rory Bowden4, Eshita Sharma4, Vincent Pedergnana5, Suresh Venkateswaran6, Subra Kugathasan6, Angela Mo7, Greg Gibson7, Graham Cooke8, John McLauchlan9, Eleanor Barnes1,2,3, John Kenneth Baillie10,11, Sarah Teichmann12, Alex Mentzer4, 4 4 1,3,13 1,2,3 John Todd , Julian Knight , Holm Uhlig , Paul Klenerman * 1. Translational Gastroenterology Unit, Nuffield Department of Medicine, University of Oxford, Oxford OX3 9DU, UK 2. Peter Medawar Building for Pathogen Research, Nuffield Department of Medicine, University of Oxford, Oxford OX1 3SY, UK 3. NIHR Biomedical Research Centre, John Radcliffe Hospital, Oxford, OX3 9DU 4. Wellcome Centre for Human Genetics, Roosevelt Dr, Headington, Oxford OX3 7BN 5. French National Centre for Scientific Research (CNRS), Laboratory MIVEGEC (CNRS, IRD, UM), Montpellier, France 6. Department of Pediatrics, Emory University School of Medicine and Children’s health care of Atlanta, Atlanta, USA 7. Center for Integrative Genomics, Georgia Institute of Technology, Atlanta, USA 8. Department of Infectious Disease, Faculty of Medicine, Imperial College London, London W2 1PG, UK 9. -
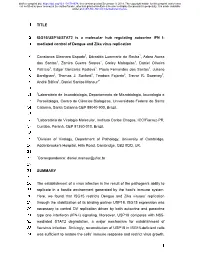
How New RNA Genes Are Born
Nicholas Delihas human FAM247 long intergenic non-coding RNA gene family Biology ︱ A model of gene formation involving these so-called pseudogenes has been presented by Dr Delihas whereby FAM247 forms human pseudogenes such as the FAM247 fragment serves as a POM121L9P nucleation element or a foundation site. Other sequence blocks from other parts of the genome are added How new RNA FAM247 spans evolutionary time to the FAM247 sequence to form the over 350 million years mature gene (see figure 2). These FAM247 fragments are in genomic regions that display evolutionarily conserved sequence signatures. The genes are born GGT5 –gamma-glutamyltransferase 5 protein gene found FAM247 sequence appears to carry in house mouse contains the 5’ half sequence of FAM247 the information for the attachment The study of gene birth and ene duplication, the formation Evolutionary scientists routinely survey of these extraneous sequences and evolution focuses on the of new genes from an exact the genetic architecture of human and it represents a focal point for the identification of ancestral Gcopy of existing ones, has long primate populations, along those of USP18 protein carboxy end sequence from FAM247: de novo genesis of this and other genetic sequences, highly been considered the major process other species, to find out the specific QETAYLLVYMKMEC372. A similar sequence is in zebrafish pseudogenes. These pseudogenes conserved during evolution, behind gene formation. However, it has roles that different genes play in the display RNA transcript expression, that can serve as a foundation been shown that genes may be born way different populations adapt to and several in a very broad and robust for gene development. -

Emerging Roles of USP18: from Biology to Pathophysiology
Review Emerging Roles of USP18: From Biology to Pathophysiology Ji An Kang 1,2 and Young Joo Jeon 1,2,* 1 Department of Biochemistry, Chungnam National University College of Medicine, Daejeon 35015, Korea; [email protected] 2 Department of Medical Science, Chungnam National University College of Medicine, Daejeon 35015, Korea * Correspondence: [email protected]; Tel: +82 42 280 6766, Fax: +82 42 280 6769 Received: 27 August 2020; Accepted: 14 September 2020; Published: 17 September 2020 Abstract: Eukaryotic proteomes are enormously sophisticated through versatile post-translational modifications (PTMs) of proteins. A large variety of code generated via PTMs of proteins by ubiquitin (ubiquitination) and ubiquitin-like proteins (Ubls), such as interferon (IFN)-stimulated gene 15 (ISG15), small ubiquitin-related modifier (SUMO) and neural precursor cell expressed, developmentally downregulated 8 (NEDD8), not only provides distinct signals but also orchestrates a plethora of biological processes, thereby underscoring the necessity for sophisticated and fine- tuned mechanisms of code regulation. Deubiquitinases (DUBs) play a pivotal role in the disassembly of the complex code and removal of the signal. Ubiquitin-specific protease 18 (USP18), originally referred to as UBP43, is a major DUB that reverses the PTM of target proteins by ISG15 (ISGylation). Intriguingly, USP18 is a multifaceted protein that not only removes ISG15 or ubiquitin from conjugated proteins in a deconjugating activity-dependent manner but also acts as a negative modulator of type I IFN signaling, irrespective of its catalytic activity. The function of USP18 has become gradually clear, but not yet been completely addressed. In this review, we summarize recent advances in our understanding of the multifaceted roles of USP18. -

Isgylation and Inhibits TGF-Β1- Induced Fibronectin Expression
Original research J Investig Med: first published as 10.1136/jim-2019-001145 on 23 December 2019. Downloaded from FOXO3a is stabilized by USP18- mediated de- ISGylation and inhibits TGF-β1- induced fibronectin expression Ban Wang,1 Yanhui Li,2,3 Heather Wang,3 Jing Zhao,3 Yutong Zhao ,3 Zhonghui Liu,1 Haichun Ma2 1Department of Immunology, ABSTRact College of Basic Medical FOXO3a belongs to a family of transcription factors Significance of this study Sciences, Jilin University, Changchun, China characterized by a conserved forkhead box DNA- 2 What is already known about this subject? Department of Anesthesia, binding domain. It has been known to regulate Jilin University First Hospital, various cellular processes including cell proliferation, ► FOXO3a regulates various cellular Changchun, China and biological functions including cell 3 apoptosis and differentiation. Post- translational Department of Physiology modifications of FOXO3a and their roles in the proliferation and death. and Cell Biology, Ohio State ► FOXO3a can be post- translational modified University, Columbus, Ohio, regulation of FOXO3a activity have been well- USA documented. FOXO3a can be phosphorylated, by phosphorylation, ubiquitination and acetylated and ubiquitinated, however, the acetylation. Correspondence to ISGylation of FOXO3a has not been reported. ► Post- translational modification regulates Dr Zhonghui Liu; Protein overexpression, ISGylation and half-life FOXO3a’s stability and activity. liuzh@ jlu. edu. cn were measured to determine the post- translational Dr Haichun Ma; What are the new findings? modification of FOXO3a. Human fibroblast cells were mahc@ jlu. edu. cn ► FOXO3a can be ISGylated. treated with transforming growth factor (TGF)- 1 to β ► ISGylation of FOXO3a determines FOXO3a Accepted 26 November determine the role of FOXO3a ISGylation in TGF-β1 half- life. -
1 TITLE 1 2 ISG15/USP18/STAT2 Is a Molecular Hub Regulating Autocrine
bioRxiv preprint doi: https://doi.org/10.1101/784678; this version posted December 9, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 TITLE 2 3 ISG15/USP18/STAT2 is a molecular hub regulating autocrine IFN I- 4 mediated control of Dengue and Zika virus replication 5 6 Constanza Eleonora Espada1, Edroaldo Lummertz da Rocha1, Adara Aurea 7 dos Santos1, Zamira Guerra Soares1, Greicy Malaquias1, Daniel Oliveira 8 Patrício1, Edgar Gonzalez Kozlova1, Paula Fernandes dos Santos1, Juliano 9 Bordignon2, Thomas J. Sanford3, Teodoro Fajardo3, Trevor R. Sweeney3, 10 André Báfica1, Daniel Santos Mansur1* 11 12 1Laboratório de Imunobiologia, Departamento de Microbiologia, Imunologia e 13 Parasitologia, Centro de Ciências Biológicas, Universidade Federal de Santa 14 Catarina, Santa Catarina CEP 88040-900, Brazil. 15 16 2Laboratório de Virologia Molecular, Instituto Carlos Chagas, ICC/Fiocruz-PR, 17 Curitiba, Paraná, CEP 81350-010, Brazil. 18 19 3Division of Virology, Department of Pathology, University of Cambridge, 20 Addenbrooke's Hospital, Hills Road, Cambridge, CB2 0QQ, UK. 21 22 *Correspondence: [email protected] 23 24 SUMMARY 25 26 The establishment of a virus infection is the result of the pathogen’s ability to 27 replicate in a hostile environment generated by the host’s immune system. 28 Here, we found that ISG15 restricts Dengue and Zika viruses’ replication 29 through the stabilization of its binding partner USP18. ISG15 expression was 30 necessary to control DV replication driven by both autocrine and paracrine 31 type one interferon (IFN-I) signaling.