(TDA): Botswana Component Partial Report Key Public Health Issues
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

NGAMILAND SUSTAINABLE LAND MANAGEMENT PROJECT “Mainstreaming SLM in Rangeland Areas of Ngamiland- District Landscapes for Improved Livelihoods”
NGAMILAND SUSTAINABLE LAND MANAGEMENT PROJECT “Mainstreaming SLM in Rangeland Areas of Ngamiland- District Landscapes for Improved Livelihoods” Project Steering Committee (PSC) Meeting Thursday 5th July, 2018 Maun Lodge 0900 Hours BOARD DOCUMENTS Page 1 of 42 TABLE OF CONTENTS TABLE OF CONTENTS ..........................................................................................................................2 MEETING AGENDA ..............................................................................................................................3 LIST OF ACRONYMS ............................................................................................................................4 MINUTES OF 2018 QUARTER 1 PSC MEETING .......................................................................................6 ANNEX TO MINUTES ......................................................................................................................... 16 Annex 1: 2018 Quarter 1 Progress Report ....................................................................................... 16 2018 QUARTER 2 PROGRESS REPORT ................................................................................................. 26 Request for Increased ASL ............................................................................................................. 36 Approved Annual Workplan and Budget 2018................................................................................. 37 Page 2 of 42 MEETING AGENDA NGAMILAND SUSTAINABLE LAND MANAGEMENT -

IVIV VV VI Pretoria Pretoria Soweto Soweto 0 125 250 Kmiv IV V V VV V
Earthquake Green Shaking Alert M 6.5, Botswana Origin Time: Mon 2017-04-03 17:40:16 UTC (19:40:16 local) PAGER o o Location: 22.62 S 25.15 E Depth: 11 km Version 1 Created: 40 minutes, 53 seconds after earthquake Estimated Fatalities Green alert for shaking-related fatalities Estimated Economic Losses and economic losses. There is a low likelihood of casualties and damage. 65% 50% 30% 32% 15% 4% 3% 1 100 10,000 1 100 10,000 10 1,000 100,000 10 1,000 100,000 Fatalities USD (Millions) Estimated Population Exposed to Earthquake Shaking ESTIMATED POPULATION - -* 3,776k* 19,253k* 2,733k 54k 2k 0 0 0 EXPOSURE (k = x1000) ESTIMATED MODIFIED MERCALLI INTENSITY PERCEIVED SHAKING Not felt Weak Light Moderate Strong Very Strong Severe Violent Extreme Resistant none none none V. Light Light Moderate Moderate/Heavy Heavy V. Heavy POTENTIAL Structures DAMAGE Vulnerable Structures none none none Light Moderate Moderate/Heavy Heavy V. Heavy V. Heavy *Estimated exposure only includes population within the map area. Population Exposure population per ~1 sq. km from Landscan Structures: Overall, the population in this region resides in structures that are vulnerable to IV 21°E ShakaweShakaweShakawe 24°E HwangeHwange27°E earthquake shaking, though some resistant PandamatengaPandamatengaPandamatenga DeteDete structures exist. LupaneLupaneLupane Historical Earthquakes (with MMI levels): There were no earthquakes with significant NokanengNokaneng InyathiInyathiInyathi ShanganiShanganiShangani population exposure to shaking within a 400 MaunMaun MaunMaun SuaSuaSua -

Department of Road Transport and Safety Offices
DEPARTMENT OF ROAD TRANSPORT AND SAFETY OFFICES AND SERVICES MOLEPOLOLE • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Transport Inspectorate Tel: 5920148 Fax: 5910620 P/Bag 52 Molepolole Next to Molepolole Police MOCHUDI • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Transport Inspectorate P/Bag 36 Mochudi Tel : 5777127 Fax : 5748542 White House GABORONE Headquarters BBS Mall Plot no 53796 Tshomarelo House (Botswana Savings Bank) 1st, 2nd &3rd Floor Corner Lekgarapa/Letswai Road •Registration & Licensing of vehicles and drivers •Road safety (Public Education) Tel: 3688600/62 Fax : Fax: 3904067 P/Bag 0054 Gaborone GABORONE VTS – MARUAPULA • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Vehicle Examination Tel: 3912674/2259 P/Bag BR 318 B/Hurst Near Roads Training & Roads Maintenance behind Maruapula Flats GABORONE II – FAIRGROUNDS • Registration & Licensing of vehicles and drivers • Driver Examination : Theory Tel: 3190214/3911540/3911994 Fax : P/Bag 0054 Gaborone GABORONE - OLD SUPPLIES • Registration & Licensing of vehicles and drivers • Transport Permits • Transport Inspectorate Tel: 3905050 Fax :3932671 P/Bag 0054 Gaborone Plot 1221, Along Nkrumah Road, Near Botswana Power Corporation CHILDREN TRAFFIC SCHOOL •Road Safety Promotion for children only Tel: 3161851 P/Bag BR 318 B/Hurst RAMOTSWA •Registration & Licensing of vehicles and drivers •Driver Examination (Theory & Practical -

The Hydrology of the Okavango Delta, Botswana—Processes, Data and Modelling
Regional review: the hydrology of the Okavango Delta, Botswana—processes, data and modelling Christian Milzow & Lesego Kgotlhang & Peter Bauer-Gottwein & Philipp Meier & Wolfgang Kinzelbach Abstract The wetlands of the Okavango Delta accom- Introduction modate a multitude of ecosystems with a large diversity in fauna and flora. They not only provide the traditional The Okavango wetlands, commonly called the Okavango livelihood of the local communities but are also the basis Delta, are spread on top of an alluvial fan located in of a tourism industry that generates substantial revenue for northern Botswana, in the western branch of the East the whole of Botswana. For the global community, the African Rift Valley. Waters forming the Okavango River wetlands retain a tremendous pool of biodiversity. As the originate in the highlands of Angola, flow southwards, upstream states Angola and Namibia are developing, cross the Namibian Caprivi-Strip and eventually spread however, changes in the use of the water of the Okavango into the terminal wetlands on Botswanan territory cover- River and in the ecological status of the wetlands are to be ing the alluvial fan (Fig. 1). Whereas the climate in the expected. To predict these impacts, the hydrology of the headwater region is subtropical and humid with an annual Delta has to be understood. This article reviews scientific precipitation of up to 1,300 mm, it is semi-arid in Botswana work done for that purpose, focussing on the hydrological with precipitation amounting to only 450 mm/year in the modelling of surface water and groundwater. Research Delta area. High potential evapotranspiration rates cause providing input data to hydrological models is also over 95% of the wetland inflow and local precipitation to be presented. -

Thursday 26 November 2020 the First Meeting of the Second Session of the Twelfth Parliament English Version
THE FIRST MEETING OF THE SECOND SESSION OF THE TWELFTH PARLIAMENT THURSDAY 26 NOVEMBER 2020 ENGLISH VERSION HANSARD NO: 200 THE NATIONAL ASSEMBLY SPEAKER The Hon. Phandu T. C. Skelemani PH, MP. DEPUTY SPEAKER The Hon. Mabuse M. Pule, MP. (Mochudi East) Clerk of the National Assembly - Ms B. N. Dithapo Deputy Clerk of the National Assembly - Mr L. T. Gaolaolwe Learned Parliamentary Counsel - Ms M. Mokgosi Assistant Clerk (E) - Mr R. Josiah CABINET His Excellency Dr M. E. K. Masisi, MP. - President His Honour S. Tsogwane, MP. (Boteti West) - Vice President Minister for Presidential Affairs, Governance and Public Hon. K. N. S. Morwaeng, MP. (Molepolole South) - Administration Hon. K. T. Mmusi, MP. (Gabane-Mmankgodi) - Minister of Defence, Justice and Security Hon. Dr L. Kwape, MP. (Kanye South) - Minister of International Affairs and Cooperation Hon. E. M. Molale, MP. (Goodhope-Mabule ) - Minister of Local Government and Rural Development Hon. K. S. Gare, MP. (Moshupa-Manyana) - Minister of Agricultural Development and Food Security Minister of Environment, Natural Resources Conservation Hon. P. K. Kereng, MP. (Specially Elected) - and Tourism Hon. Dr E. G. Dikoloti MP. (Mmathethe-Molapowabojang) - Minister of Health and Wellness Hon. T.M. Segokgo, MP. (Tlokweng) - Minister of Transport and Communications Hon. K. Mzwinila, MP. (Specially Elected) - Minister of Land Management, Water and Sanitation Services Minister of Youth Empowerment, Sport and Culture Hon. T. M. Rakgare, MP. (Mogoditshane) - Development Hon. A. M. Mokgethi, MP. (Gaborone Bonnington North) - Minister of Nationality, Immigration and Gender Affairs Hon. Dr T. Matsheka, MP. (Lobatse) - Minister of Finance and Economic Development Hon. F. M. M. -
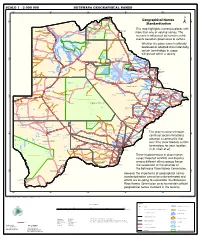
Geographical Names Standardization BOTSWANA GEOGRAPHICAL
SCALE 1 : 2 000 000 BOTSWANA GEOGRAPHICAL NAMES 20°0'0"E 22°0'0"E 24°0'0"E 26°0'0"E 28°0'0"E Kasane e ! ob Ch S Ngoma Bridge S " ! " 0 0 ' ' 0 0 ° Geographical Names ° ! 8 !( 8 1 ! 1 Parakarungu/ Kavimba ti Mbalakalungu ! ± n !( a Kakulwane Pan y K n Ga-Sekao/Kachikaubwe/Kachikabwe Standardization w e a L i/ n d d n o a y ba ! in m Shakawe Ngarange L ! zu ! !(Ghoha/Gcoha Gate we !(! Ng Samochema/Samochima Mpandamatenga/ This map highlights numerous places with Savute/Savuti Chobe National Park !(! Pandamatenga O Gudigwa te ! ! k Savu !( !( a ! v Nxamasere/Ncamasere a n a CHOBE DISTRICT more than one or varying names. The g Zweizwe Pan o an uiq !(! ag ! Sepupa/Sepopa Seronga M ! Savute Marsh Tsodilo !(! Gonutsuga/Gonitsuga scenario is influenced by human-centric Xau dum Nxauxau/Nxaunxau !(! ! Etsha 13 Jao! events based on governance or culture. achira Moan i e a h hw a k K g o n B Cakanaca/Xakanaka Mababe Ta ! u o N r o Moremi Wildlife Reserve Whether the place name is officially X a u ! G Gumare o d o l u OKAVANGO DELTA m m o e ! ti g Sankuyo o bestowed or adopted circumstantially, Qangwa g ! o !(! M Xaxaba/Cacaba B certain terminology in usage Nokaneng ! o r o Nxai National ! e Park n Shorobe a e k n will prevail within a society a Xaxa/Caecae/Xaixai m l e ! C u a n !( a d m a e a a b S c b K h i S " a " e a u T z 0 d ih n D 0 ' u ' m w NGAMILAND DISTRICT y ! Nxai Pan 0 m Tsokotshaa/Tsokatshaa 0 Gcwihabadu C T e Maun ° r ° h e ! 0 0 Ghwihaba/ ! a !( o 2 !( i ata Mmanxotae/Manxotae 2 g Botet N ! Gcwihaba e !( ! Nxharaga/Nxaraga !(! Maitengwe -

SABONET Report No 18
ii Quick Guide This book is divided into two sections: the first part provides descriptions of some common trees and shrubs of Botswana, and the second is the complete checklist. The scientific names of the families, genera, and species are arranged alphabetically. Vernacular names are also arranged alphabetically, starting with Setswana and followed by English. Setswana names are separated by a semi-colon from English names. A glossary at the end of the book defines botanical terms used in the text. Species that are listed in the Red Data List for Botswana are indicated by an ® preceding the name. The letters N, SW, and SE indicate the distribution of the species within Botswana according to the Flora zambesiaca geographical regions. Flora zambesiaca regions used in the checklist. Administrative District FZ geographical region Central District SE & N Chobe District N Ghanzi District SW Kgalagadi District SW Kgatleng District SE Kweneng District SW & SE Ngamiland District N North East District N South East District SE Southern District SW & SE N CHOBE DISTRICT NGAMILAND DISTRICT ZIMBABWE NAMIBIA NORTH EAST DISTRICT CENTRAL DISTRICT GHANZI DISTRICT KWENENG DISTRICT KGATLENG KGALAGADI DISTRICT DISTRICT SOUTHERN SOUTH EAST DISTRICT DISTRICT SOUTH AFRICA 0 Kilometres 400 i ii Trees of Botswana: names and distribution Moffat P. Setshogo & Fanie Venter iii Recommended citation format SETSHOGO, M.P. & VENTER, F. 2003. Trees of Botswana: names and distribution. Southern African Botanical Diversity Network Report No. 18. Pretoria. Produced by University of Botswana Herbarium Private Bag UB00704 Gaborone Tel: (267) 355 2602 Fax: (267) 318 5097 E-mail: [email protected] Published by Southern African Botanical Diversity Network (SABONET), c/o National Botanical Institute, Private Bag X101, 0001 Pretoria and University of Botswana Herbarium, Private Bag UB00704, Gaborone. -

Chobe District Integrated Land Use Plan
Wageningen Environmental Research The mission of Wageningen University and Research is “To explore the potential P.O. Box 47 of nature to improve the quality of life”. Under the banner Wageningen University Chobe District Integrated Land Use Plan 6700 AB Wageningen & Research, Wageningen University and the specialised research institutes of The Netherlands the Wageningen Research Foundation have joined forces in contributing to T +31 (0) 317 48 07 00 inding solutions to important questions in the domain of healthy food and living www.wur.eu/environmental-research environment. With its roughly 30 branches, 5,000 employees and 10,000 students, Wageningen University & Research is one of the leading organisations in its domain. Report 2813 The unique Wageningen approach lies in its integrated approach to issues and ISSN 1566-7197 the collaboration between diff erent disciplines. Theo van der Sluis, Lin Cassidy, Chris Brooks, Piotr Wolski, Cornelis VanderPost, Piet Wit, Rene Henkens, Michiel van Eupen, Keta Mosepele, Oggie Maruapula, Elmar Veenendaal Chobe District Integrated Land Use Plan Theo van der Sluis1, Lin Cassidy2, Chris Brooks2, Piotr Wolski2, Cornelis VanderPost2, Piet Wit2, Rene Henkens1, Michiel van Eupen1, Keta Mosepele4, Oggie Maruapula2, Elmar Veenendaal3 1 Wageningen Environmental Research (Alterra) 2 Independent consultant 3 Wageningen University & Research 4 ORI This research is funded by UNDP, Contract nr. PR005/2016. Wageningen Environmental Research Wageningen, July 2017 Report 2813 ISSN 1566-7197 Theo van der Sluis, Lin Cassidy, Chris Brooks, Piotr Wolski, Cornelis VanderPost, Piet Wit, Rene Henkens, Michiel van Eupen, Keta Mosepele, Oggie Maruapula, Elmar Veenendaal, 2017. Chobe District Integrated Land Use Plan. Wageningen, Wageningen Environmental Research, Report 2813. -
Lea Smme Directory 2016
www.lea.co.bw LEA SMME DIRECTORY 2016 Manufacturing Tourism Agriculture Services DISCLAIMER The information published in this document is for the sole purpose of marketing LEA registered SMME’s. LEA shall not be liable for any loss howsoever incurred as a result of use of content on this document in whole or in part. LEA further does not warrant that a business placing reliance on this document will generate certain results, nor does LEA guarantee any particular outcome of the application of the contents hereof to any situation. The clients and users hereby indemnifies and holds harmless LEA, its successors in title, agents and employees against any and all claims for loss or inconvenience arising out of the implementation by the user of the contents of this document or any annexure or addendum to it. www.lea.co.bw LEA SMME Directory 2016 LEA INCUBATORS NETWORK Vision To be the centre of excellence for entrepreneurship and sustainable SMME development in Botswana. LEA Mission To promote and facilitate entrepreneurship and SMME development through targeted interventions, in pursuit of economic diversification. Values Self-driven– We are passionate, eager to learn, persistent and determined to achieve personal goals so that the entire team achieves its desired results. Trasformational GABORONE LEATHER INDUSTRIES GLEN VALLEY HORTICULTURE leadership- We are inspired and self-led, motivated, INCUBATOR INCUBATOR innovative, innovative and Plot 4799 / 4800 Plot 63069 accountable to achieve Old Bedu Station Extension 67 maximum potential in a favourable environment. Macheng Way Private Bag X035 Private Bag 0301 Glen Valley Partnership- Through our Gaborone, Botswana Gaborone Botswana internal teamvork and Tel: (+267) 3105330 Tel: (+267) 3186309 effective partnership with stakeholders, our efforts are Fax: (+267) 3105334 Fax: (+267) 3186437 synergized resulting in the success of our clientele. -

List of Cities in Botswana
List of cities in Botswana The following is a list of cities and towns in Botswana with population of over 3,000 citizens. State capitals are shown in boldface. Population Female Rank Name District Census District [1] Male Population 2001. Population 1. Gaborone South-East District Gaborone 186,007 91,823 94,184 2. Francistown North-East District Francistown 83,023 40,134 42,889 3. Molepolole Kweneng District Kweneng East 62,739 28,617 34,122 4. Serowe Central District Central Serowe/Palapye 52,831 25,400 27,431 5. Selibe Phikwe Central District Selibe Phikwe 49,849 24,334 25,515 6. Maun North-West District Ngamiland East 49,822 23,714 26,108 7. Kanye Southern District Ngwaketse 48,143 22,451 25,692 8. Mahalapye Central District Central Mahalapye 43,538 21,120 22,418 9. Mogoditshane Kweneng District Kweneng East 40,753 20,972 19,781 10. Mochudi Kgatleng District Kgatleng 39,349 18,490 20,859 11. Lobatse South-East District Lobatse 29,689 14,202 15,487 12. Palapye Central District Central Serowe/Palapye 29,565 13,995 15,570 13. Ramotswa South-East District South East 25,738 12,027 13,711 14. Moshupa Southern District Ngwaketse 22,811 10,677 12,134 15. Tlokweng South-East District South East 22,038 10,568 11,470 16. Bobonong Central District Central Bobonong 21,020 9,877 11,143 17. Thamaga Kweneng District Kweneng East 20,527 9,332 11,195 18. Letlhakane Central District Central Boteti 19,539 9,848 9,691 19. -

January-December 2017 Report
BOTSWANA RED CROSS SOCIETY/BOTSWANA/SOUTHERN AFRICA JANUARY-DECEMBER 2017 REPORT Photo caption and credit: Moshupa First aid action team (Photo by BRCS) 2 I Botswana Red Cross Society Report– 04/01/2017 to 18/12/2017 TABLE OF CONTENTS 1.0 Programme purpose ..................................................................................................................................................... 5 2.0 Programmes summary .................................................................................................................................................. 5 2.1 Financial situation ..................................................................................................................................................... 5 2.2 No of people reached................................................................................................................................................... 5 2.3 Our partners ................................................................................................................................................................. 6 International including movement partners ....................................................................................................................... 6 3.0 Situation/Context Analysis ........................................................................................................................................... 6 4.0 Progress towards outcomes ......................................................................................................................................... -

Transboundary Diagnostic Analysis of the Okavango River Basin the Status of Tourism Development in the Okavango Delta, Botswan
EFA Namibia Irrigation Development. Transboundary Diagnostic Analysis of the Okavango River Basin The Status of Tourism Development in the Okavango Delta, Botswana Joseph E. Mbaiwa Harry Oppenheimer Okavango Research Centre May 2009 1 TDA Botswana Tourism Development Transboundary Diagnostic Analysis of the Okavango River Basin The Status of Tourism Development in the Okavango Delta, Botswana Joseph E. Mbaiwa, PhD Harry Oppenheimer Okavang o Research Centre University of Bot swana May 2009 2 TDA Botswana Tourism Development CONTENTS TABLES: .................................................................................................................................. 4 Executive Summary ................................................................................................................... 5 1. Introduction ................................................................................................................... 7 2. Objectives of the Study ..................................................................................................... 8 3. National Policies and Plans ................................................................................................ 9 3.1 The Tourism Policy of 1990 ....................................................................................... 9 3.2 The Wildlife Conservation Policy of 1986 .................................................................. 9 3.3 The CBNRM Policy of 2007 .....................................................................................