Propylene Oxide
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The PO Production Chain and Possibilities for Energy Saving
The PO production chain and possibilities for energy saving Public Summary Report Delft, January 2012 Author(s): Ewout Dönszelmann Ab de Buck Harry Croezen Lonneke Wielders Publication Data Bibliographical data: Ewout Dönszelmann, Ab de Buck, Harry Croezen, Lonneke Wielders The PO production chain and possibilities for energy saving Public Summary Delft, CE Delft, January 2012 Energy saving / Chain Management / Products / Chemical industry / Propylene Oxide / Styrene / Iso-butylene FT: Tert-butyl alcohol (TBA) Publication code: 12.2232.12 CE publications are available from www.cedelft.eu. Commissioned by: Agentschap NL Further information on this study can be obtained from the contact person, Ewout Dönszelmann. © copyright, CE Delft, Delft CE Delft Committed to the Environment CE Delft is an independent research and consultancy organisation specialised in developing structural and innovative solutions to environmental problems. CE Delft’s solutions are characterised in being politically feasible, technologically sound, economically prudent and socially equitable. 2 January 2012 2.232.3 – The PO production chain and possibilities for energy saving Contents 1 Introduction 5 1.1 General background 5 1.2 The project 5 1.3 Approach 6 1.4 Reading guide 6 2 The production chains 7 2.1 The two processes 7 2.2 Expanded polystyrene 9 2.3 Polyols 11 2.4 TBA/iso-butylene applications 13 3 Conclusions, recommendations 17 3.1 Conclusions 17 3.2 Recommendations 17 4 Background of the Long-term Agreement Energy Efficiency ETS enterprises (LEE) 19 References 21 3 January 2012 2.232.3 – The PO production chain and possibilities for energy saving 4 January 2012 2.232.3 – The PO production chain and possibilities for energy saving 1 Introduction 1.1 General background The Dutch Industry and the Dutch government have made long term agreements on energy efficiency (LEE) for companies that are under the European Trading Scheme (ETS). -

Understanding Pigments: the Third Step to Higher Quality And
Understanding Pigments: The Third Mark Harber October, 2000 Step to Higher Quality and Consistency Putting great color in your product is part of the pigments. However, they are less opaque and systems approach for resolving issues of sub- would have to be used at higher loading levels to standard properties and appearance. achieve similar whiteness and opacity. This article on pigments is the third in a four-part Titanium Dioxide is used in the majority of the series about the interrelationship of the material products made by the cast polymer industry. Tita- components used in marble and solid surface nium Dioxide-based colors include most whites, manufacturing. These AOC-authored articles re- pastels, earth tones and off-whites such as bone, spond to the challenge that the cast polymer in- ivory, beige or biscuit. As noted in Table 1, non- dustries aspire to higher standards of quality and white synthetic oxides are combined with Titani- consistency. Because resolving cast polymer is- um Dioxide to create pastels and earth tones for sues requires a systems approach, other articles cultured marble and solid surface applications. in this series address resins, gel coats and pro- cessing. All articles begin with background infor- Phthalocyanine pigments, or "Phthalos," impart mation on the main subject matter, followed by deep colors such as the automotive "Hunter ten related issues and guidelines. Green" of a sport utility vehicle or the high strength Blue used in ballpoint pens. Because A BACKGROUND ON COLORANTS they are so deep when used by themselves, In their natural state, cast polymer resins meet a Phthalo Blue and Phthalo Green are normally variety of performance requirements but are lack- blended with other pigments, many times Titani- ing in the color that draws the customer to the um Dioxide. -

Acute Exposure Guideline Levels for Selected Airborne Chemicals: Volume 11
This PDF is available from The National Academies Press at http://www.nap.edu/catalog.php?record_id=13374 Acute Exposure Guideline Levels for Selected Airborne Chemicals: Volume 11 ISBN Committee on Acute Exposure Guideline Levels; Committee on 978-0-309-25481-6 Toxicology; National Research Council 356 pages 6 x 9 PAPERBACK (2012) Visit the National Academies Press online and register for... Instant access to free PDF downloads of titles from the NATIONAL ACADEMY OF SCIENCES NATIONAL ACADEMY OF ENGINEERING INSTITUTE OF MEDICINE NATIONAL RESEARCH COUNCIL 10% off print titles Custom notification of new releases in your field of interest Special offers and discounts Distribution, posting, or copying of this PDF is strictly prohibited without written permission of the National Academies Press. Unless otherwise indicated, all materials in this PDF are copyrighted by the National Academy of Sciences. Request reprint permission for this book Copyright © National Academy of Sciences. All rights reserved. Acute Exposure Guideline Levels for Selected Airborne Chemicals: Volume 11 Committee on Acute Exposure Guideline Levels Committee on Toxicology Board on Environmental Studies and Toxicology Division on Earth and Life Studies Copyright © National Academy of Sciences. All rights reserved. Acute Exposure Guideline Levels for Selected Airborne Chemicals: Volume 11 THE NATIONAL ACADEMIES PRESS 500 FIFTH STREET, NW WASHINGTON, DC 20001 NOTICE: The project that is the subject of this report was approved by the Governing Board of the National Research Council, whose members are drawn from the councils of the National Academy of Sciences, the National Academy of Engineering, and the Insti- tute of Medicine. The members of the committee responsible for the report were chosen for their special competences and with regard for appropriate balance. -

Nitrogen Dioxide
Common Name: NITROGEN DIOXIDE CAS Number: 10102-44-0 RTK Substance number: 1376 DOT Number: UN 1067 Date: May 1989 Revision: April 2000 ----------------------------------------------------------------------- ----------------------------------------------------------------------- HAZARD SUMMARY * Nitrogen Dioxide can affect you when breathed in. * If you think you are experiencing any work-related health * Nitrogen Dioxide may cause mutations. Handle with problems, see a doctor trained to recognize occupational extreme caution. diseases. Take this Fact Sheet with you. * Contact can irritate and burn the skin and eyes with * Exposure to hazardous substances should be routinely possible eye damage. evaluated. This may include collecting personal and area * Breathing Nitrogen Dioxide can irritate the nose and air samples. You can obtain copies of sampling results throat. from your employer. You have a legal right to this * Breathing Nitrogen Dioxide can irritate the lungs causing information under OSHA 1910.1020. coughing and/or shortness of breath. Higher exposures can cause a build-up of fluid in the lungs (pulmonary edema), a medical emergency, with severe shortness of WORKPLACE EXPOSURE LIMITS breath. OSHA: The legal airborne permissible exposure limit * High levels can interfere with the ability of the blood to (PEL) is 5 ppm, not to be exceeded at any time. carry Oxygen causing headache, fatigue, dizziness, and a blue color to the skin and lips (methemoglobinemia). NIOSH: The recommended airborne exposure limit is Higher levels can cause trouble breathing, collapse and 1 ppm, which should not be exceeded at any even death. time. * Repeated exposure to high levels may lead to permanent lung damage. ACGIH: The recommended airborne exposure limit is 3 ppm averaged over an 8-hour workshift and IDENTIFICATION 5 ppm as a STEL (short term exposure limit). -

Emerging Technology
INDUSTRY NEWS EMERGING TECHNOLOGY Iron-based superconductors reinforce link to magnetism BRIEFS A new class of iron-oxyarsenide-based superconductors discovered earlier this year shares IDES Inc., a plastic similar unusual magnetic properties with previously known high-temperature superconductors materials information based on copper-oxide materials, report researchers at the National Institute of Standards and management company, Technology, Gaithersburg, Md. The work emphasizes a critical but as yet unexplained link be- and Firehole Technologies Inc., a tween magnetism and high-temperature superconductors. developer of innovative The importance of magnetism to high-temperature superconductors is remarkable because simulation technologies magnetism strongly interferes with conventional, low-temperature superconductors, but now for composite materials may prove to be an integral element of such materials. and structures, have The team used neutron beams to demonstrate that, like copper-oxide superconductors, the entered into a strategic new iron-oxyarsenide HTc materials discovered by Japanese researchers share an unusual partnership to develop a magnetic structure with magnetically active layers interspersed with layers of nonmagnetic searchable composite material. materials database. For more information: Qingzhen Huang, National Institute of Standards & Technology, 100 www.ides.com Bureau, Gaithersburg, MD 20899; tel: 301/ 975-6164; [email protected]; www.nist.gov. Intel Corp., Samsung Electronics, Copper nanowire arrays grown on different surfaces and Taiwan A simple process to grow upright copper nanowires on a variety of materials is under develop- Semiconductor ment by researchers at the University of Illinois in Urbana Champaign. The nanowire arrays Manufacturing could be suitable for field-emission displays, a new type of display technology that promises to pro- Company (TSMC) vide brighter, more vivid pictures than ex- have reached agreement on the need for industry- isting flat-panel displays. -

The Oxidation of Carbon Monoxide Using a Tin Oxide
THE OXIDATION OF CARBON MONOXIDE USING A TIN OXIDE CATALYST Christopher F. Sampson and Nicholas J. Gudde United Kingdom Atomic Energy Authority A.E.R.E. Harwell, Didcot, Oxon. United Kingdom SUMMARY This paper outlines some of the steps involved in the development by the United Kingdom Atomic Energy Authority (UKAEA) of a catalytic device for the recombination of carbon monoxide and oxygen in a C02 laser system. It contrasts the differences between CO oxidation for air purification and for laser environmental control, but indicates that there are similarities between the physical specifications. The principal features of catalytic devices are outlined and some experimental work described. This includes measurements concerning the structure and mechanical properties of the artifact, the preparation of the catalyst coating and its interaction with the gaseous environment. The paper concludes with some speculation about the method by which the reaction actually occurs. INTRODUCTION During the late 1970's, the United Kingdom Atomic Energy Authority at Harwell became involved in sol-gel technology as a result of oxide fuel development. The sol-gel method was found to be suitable for the preparation of catalytic materials which eventually led to their use in car exhaust catalytic converters and for air purification catalysts. Such catalysts were usually in the form of coatings applied to supporting artifacts such as monoliths, formed from either cordierite or from a corrosion resistant metal such as Fecralloy steel (R). The UKAEA has experience in the use of sol-gel catalysts for CO removal from air and so has a technological link to a system intended to recombine O2 and CO formed in sealed C02 lasers. -

Zinc Oxide Sulfide Scavenger Contains a High-Quality Zinc Oxide
ZINC OXIDE ZINC OXIDE sulfide scavenger contains a high-quality ZINC OXIDE. The very fine particle-size of ZINC OXIDE scavenger results in a maximum amount of surface area for fast, efficient sulfide scavenging. It reacts with sulfides (see APPLICATIONS below) to form ZnS. This precipitate is an insoluble, inert, fine solid that remains harmlessly in the mud system or is removed by the solids-control equipment. Typical Physical Properties Physical appearance ������������������������������������������������������������������������������������������������������������������������������������������������������������������������������ White to off-white powder Specific gravity .......................................................................................................................................................................................................................... 5.4 – 5.6 Bulk density ........................................................................................................................................................................................................ 164 lb/ft3 (2627 kg/m3) Applications Under operating conditions, ZINC OXIDE scavenger reacts with sulfides to form ZnS, as shown in these equations: Zn2+ + HS- + OH- → ZnS ↓ + 2+ 2- H2O Zn + S → ZnS ↓ INC XIDE Z O scavenger is effective at the pH levels found in drilling fluids. It is recommended that a pH above 11 be maintained whenever H2S is - 2- expected. This high alkalinity converts the dangerous H2S gas to less toxic bisulfide -
HPPO Process Technology a Novel Route to Propylene Oxide Without Coproducts
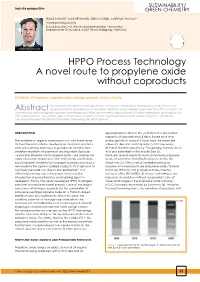
sustainability/ Industry perspective GREEN CHEMISTRy FRANZ SCHMIDT, MAIK BERNHARD, HEIKO MORELL, MATTHIAS PASCALy* *Corresponding author Evonik Industries AG, Advanced Intermediates – Innovation, Rodenbacher Chaussee 4, 63457 Hanau-Wolfgang, Germany Matthias Pascaly HPPO Process Technology A novel route to propylene oxide without coproducts KEYWORDS: HPPO process, propylene oxide, hydrogen peroxide, titanium silicalite. The common industrial technologies for the conversion of propylene to propylene oxide have been Abstract compared with a special focus on the direct oxidation using hydrogen peroxide. The HPPO process is an economically and ecologically superior technology since there are no market dependencies of other coproducts and water is the only waste product. The catalyst used in this process is a partly titanium substituted silica based zeolite called TS-1. The article summarizes the most important information concerning the HPPO process. INTRODUCTION approximately 7 Mt/a in the year 2010 at a production capacity of approximately 8 Mt/a. Based on a total The oxidation of organic compounds is of vital importance market growth of around 5 % per year, the expected for the chemical industry. Besides basic oxidation reactions values for demand and capacity in 2015 are nearly such as bleaching processes (e.g. paper or laundry) also at 9 and 10 Mt/a respectively. The growing markets are in oxidation reactions of chemicals are important: Epoxides Asia and potentially in the Middle East (1). - especially ethylene and propylene oxide – are among the There are several industrial routes to produce propylene major chemicals. Replacement of traditionally used halide- oxide, of which the chlorohydrin process (CH) is the based oxidants (chlorine) by hydrogen peroxide provided a oldest one (2). -

Propylene Oxide
This report contains the collective views of an in- ternational group of experts and does not necessarily epresent the decisions or the stated policy of the United Nations Environment Programme, the Interna- tional Labour Organisation, or the World Health lOrganization Environmental Health Criteria 56 PROPYLENE OXIDE Published under the joint sponsorship of the United Nations Environment Programme, the International Labour Organisation, and the World Health Organization World Health Organization --'-- Geneva, 1985 The International Programme on Chemical Safety (IPCS) is a joint venture the United Nations Environment Programme, the International Labour Organis tion, and the World Health Organization. The main objective of the IPCS is carry Out and disseminate evaluations of the effects of chemicals on human hea' and the quality of the environment. Supporting activities include the developm of epidemiological, experimental laboratory, and risk-assessment methods that cou produce internationally comparable results, and the development of manpower the field of toxicology. Other activities carried out by 1PCS include the develo ment of know-how for coping with chemical accidents, coordination of laborato. testing and epidemiological studies, and promotion of research on the mechanisi of th biological action of chemicals ISBN 92 4 154196 2 \Vorld Health Organization 1985 Publications of the World Health Organization enjoy copyright protection in accordance with the provisions of Protocol 2 of the Universal Copyright Conven- tion. For rights -

Sulfur Dioxide Emissions
Report on the Environment https://www.epa.gov/roe/ Sulfur Dioxide Emissions Sulfur dioxide (SO2) belongs to the family of sulfur oxide (SOx) gases. These gases are formed when fuel containing sulfur (mainly coal and oil) is burned (e.g., for electricity generation) and during metal smelting and other industrial processes. High concentrations of SO2 are associated with multiple health and environmental effects. The highest concentrations of SO2 have been recorded in the vicinity of large industrial facilities. SO2 emissions are an important environmental issue because they are a major precursor to ambient PM2.5 concentrations. Short-term exposure to airborne SO2 has been associated with various adverse health effects (ATSDR, 1998; U.S. EPA, 2017). Multiple human clinical studies, epidemiological studies, and toxicological studies support a causal relationship between short-term exposure to airborne SO2 and respiratory morbidity. The observed health effects have included respiratory symptoms, airway inflammation, and increased emergency department visits and hospitalizations for all respiratory causes. These studies further suggest that asthmatics, children, older adults, and people who spend a lot of time outdoors at increased exertion levels are potentially susceptible or vulnerable to these health effects (U.S. EPA, 2017). In addition, SO2 reacts with other air pollutants to form sulfate particles, which are constituents of fine particulate matter (PM2.5). Inhalation exposure to PM2.5 has been associated with various cardiovascular and respiratory health effects (see PM Concentrations indicator). Many other environmental effects are associated with high concentrations of SO2. For example, airborne SO2, along with nitrogen oxides (NOx), contributes to acidic deposition (the Acid Deposition indicator); SO2 is a major precursor to PM2.5 (the PM Concentrations indicator); and SO2 contributes to impaired visibility (the Regional Haze indicator). -

Reduction of Nitrogen Oxides by Carbon Monoxide Over an Iron Oxide Catalyst Under Dynamic Conditions
Applied Catalysis B: Environmental 17 (1998) 357±369 Reduction of nitrogen oxides by carbon monoxide over an iron oxide catalyst under dynamic conditions Harvey Randall, Ralf Doepper, Albert Renken* Institute of Chemical Engineering, Federal Institute of Technology, 1015 Lausanne, Switzerland Received 6 July 1997; received in revised form 23 November 1997; accepted 2 December 1997 Abstract The reduction of NO and N2O by CO over a silica-supported iron oxide catalyst was investigated by the transient response method, with different initial oxidation states of the catalyst, i.e. completely reduced (Fe3O4), or oxidised (Fe2O3). The in¯uence of CO pre-adsorption was also studied. From the material balance on the gas phase species, it was shown that the composition of the catalyst changes during relaxation to steady-state. The degree of reduction of the catalyst at steady-state could thus be estimated. During the transient period, CO was shown to inhibit N2O as well as NO reductions by adsorption on reduced sites. The activity of the reduced catalyst was found to be substantially higher as compared to the oxidised catalyst for both reactions. On this basis, it was attempted to keep the catalyst in a reduced state by periodically reducing it with CO. As a result, a signi®cant increase in the performance of the reactor with respect to steady-state operation could be achieved for N2O reduction by CO. Finally, the dynamic behaviour of the N2O±CO and NO±CO reactions made it possible to evidence reaction steps, the occurrence of which could not be shown during our previous investigations on the separate interactions of the reactants with the catalyst. -

Superconducting Properties of the Oxygen-Vacant Iron Oxyarsenide
Superconducting properties of the oxygen-vacant iron oxyarsenide TbFeAsO1- from underdoped to overdoped compositions Y.G. Sh i, 1,2,* S. Yu,3 A.A. Belik,1,2 Y. Mat sushi ta, 4 M. Tanaka,4 Y. Katsuya,5 K. Kobayashi,4 Y. Hata, 6 H. Yasuoka,6 K. Yamaura,2,3 E. Takayama-Muromachi1,2,3 1 International Center for Materials Nanoarchitectonics (MANA), National Institute for Materials Science, Tsukuba, Ibaraki 305-0044, Japan. 2 JST, Transformative Research-Project on Iron Pnictides (TRIP), Tsukuba, Ibaraki 305-0044, Japan. 3 Superconducting Materials Center, National Institute for Materials Science, 1-1 Namiki, Tsukuba, 305-0044 Ibaraki, Japan 4 NIMS Beamline Station at SPring-8, National Institute for Materials Science, 1-1-1 Kouto, Sayo-cho, Sayo-gun, Hyogo 679-5148, Japan 5 SPring-8 Service Co. Ltd., 1-1-1 Kouto, Sayo-cho, Sayo-gun, Hyogo 679-5148, Japan 6 Department of Applied Physics, National Defense Academy, 1-10-20 Hashirimizu, Yokosuka 239-8686, Japan. Abstract A wide-range doping was achieved by a high-pressure method for TbFeAsO1- from “under doped” to “over doped” superconducting compositions throughout the optimized superconductivity (Tc of 44 K). Tc vs. shows a dome-shaped feature, while Tc vs. the lattice constant likely follows a unique empirical curve over the doping range. The relatively large amount of oxygen vacancies up to ~0.3 per the formula unit was introduced possibly because of the smaller replacement Tb than the other Ln (rare-earth element) in the LnFeAsO1- system. PACS: 74.62.Bf, 74.25.Dw, 74.70.Dd 1 Introduction Discovery of high-Tc superconductivity in the iron oxypnictide LnFeAsO probably caused one of the highest impacts in materials science since 1986, the year copper oxide superconductor was discovered [1,2].