Lymphedema Faqs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bilateral Lower Extremity Hyperkeratotic Plaques: a Case Report of Ichthyosis Vulgaris
Faculty & Staff Scholarship 2015 Bilateral lower extremity hyperkeratotic plaques: a case report of ichthyosis vulgaris Hayley Leight Zachary Zinn Omid Jalali Follow this and additional works at: https://researchrepository.wvu.edu/faculty_publications Clinical, Cosmetic and Investigational Dermatology Dovepress open access to scientific and medical research Open Access Full Text Article CASE REPORT Bilateral lower extremity hyperkeratotic plaques: a case report of ichthyosis vulgaris Hayley Leight Abstract: Here, we report a case of a middle-aged woman presenting with severe, long-standing, Zachary Zinn hyperkeratotic plaques of the lower extremities unrelieved by over-the-counter medications. Omid Jalali Initial history and clinical findings were suggestive of an inherited ichthyosis. Ichthyoses are genetic disorders characterized by dry scaly skin and altered skin-barrier function. A diagnosis Department of Dermatology, West Virginia University, of ichthyosis vulgaris was confirmed by histopathology. Etiology, prevalence, and treatment Morgantown, WV, USA options are discussed. Keywords: filaggrin gene, FLG, profilaggrin, keratohyalin granules, hyperkeratosis Introduction For personal use only. Inherited ichthyoses are a diverse group of genetic disorders characterized by dry, scaly skin; hyperkeratosis; and altered skin-barrier function. While these disorders of cutaneous keratinization are multifaceted and varying in etiology, disruption in the stratum corneum with generalized scaling is common to all.1–4 Although not entirely known -

1 the Physiological and Pathological Functions of VEGFR3 in Cardiac And
Manuscript The physiological and pathological functions of VEGFR3 in cardiac and lymphatic development and related diseases Richard M. Monaghan, Donna J. Page, Pia Ostergaard and Bernard D. Keavney Downloaded from https://academic.oup.com/cardiovascres/advance-article/doi/10.1093/cvr/cvaa291/5926966 by guest on 21 October 2020 Abstract Vascular endothelial growth factor receptors (VEGFRs) are part of the evolutionarily conserved VEGF signalling pathways that regulate the development and maintenance of the body’s cardiovascular and lymphovascular systems. VEGFR3, encoded by the FLT4 gene, has an indispensable and well-characterised function in development and establishment of the lymphatic system. Autosomal dominant VEGFR3 mutations, that prevent the receptor functioning as a homodimer, cause one of the major forms of hereditary primary lymphoedema; Milroy disease. Recently, we and others have shown that FLT4 variants, distinct to those observed in Milroy disease cases, predispose individuals to Tetralogy of Fallot, the most common cyanotic congenital heart disease, demonstrating a novel function for VEGFR3 in early cardiac development. Here, we examine the familiar and emerging roles of VEGFR3 in the development of both lymphovascular and cardiovascular systems, respectively, compare how distinct genetic variants in FLT4 lead to two disparate human conditions, and highlight the research still required to fully understand this multifaceted receptor. key words: angiogenesis and lymphangiogenesis; primary lymphoedema; heart development; vascular endothelial growth factor receptors; congenital heart disease © The Author(s) 2019. Published by Oxford University Press on behalf of the European Society of Cardiology. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted reuse, distribution, and reproduction in any medium, provided the original work is properly cited. -

Skin Brief Articles
SKIN BRIEF ARTICLES Nab-paclitaxel/gemcitabine Induced Acquired Ichthyosis Adriana Lopez BAa, Joel Shugar MDb, and Mark Lebwohl MDc aColumbia University Vagelos College of Physicians and Surgeons, New York, NY bIcahn School of Medicine at Mount Sinai, Department of Otolaryngology, New York, NY cIcahn School of Medicine at Mount Sinai, Department of Dermatology, New York, NY ABSTRACT The ichthyoses are a diverse group of cutaneous disorders characterized by abnormalities in cornification. The majority of ichthyoses are inherited with childhood presentation and new onset ichthyosis in adulthood warrants further medical evaluation. Though most well recognized for its association with Hodgkin’s disease, acquired ichthyosis (AI) has been linked to a number of inflammatory, autoimmune, and endocrine processes. However, drug- induced AI is exceedingly rare and remains a poorly understood entity. Here we report a case of a male patient who developed AI while receiving nab-paclitaxel plus gemcitabine for treatment of pancreatic adenocarcinoma. months prior, the patient was first seen for INTRODUCTION recurrent, self-healing, pruritic erythematous Acquired ichythyosis (AI) is an uncommon papules. Punch biopsy was performed which non-inherited cutaneous disorder of showed an atypical cellular infiltrate of abnormal keratinization that is most scattered large CD30+ cells with clonal T-cell frequently associated with underlying receptor-β gene rearrangement. Though the malignancy. Drug induced AI is uncommon clinicopathologic diagnosis was most and has been rarely linked to consistent with lymphomatoid papulosis chemotherapeutic agents. Herein, we report (LyP), imaging was pursued to exclude the case of a man with pancreatic extracutaneous lymphoproliferative disease. adenocarcinoma who developed an CT scan incidentally detected a mass in the ichthyosiform eruption upon starting body of the pancreas and biopsy was chemotherapy with nab-paclitaxel plus concordant with pancreatic adenocarcinoma. -

Lymphatic Complaints in the Dermatology Clinic: an Osteopathic
Volume 35 JAOCDJournal Of The American Osteopathic College Of Dermatology Lymphatic Complaints in the Dermatology Clinic: An Osteopathic Approach to Management A five-minute treatment module makes lymphatic OMT a practical option in busy practices. Also in this issue: A Case of Acquired Port-Wine Stain (Fegeler Syndrome) Non-Pharmacologic Interventions in the Prevention of Pediatric Atopic Dermatitis: What the Evidence Says Inflammatory Linear Verrucous Epidermal Nevus Worsening in Pregnancy last modified on June 9, 2016 10:54 AM JOURNAL OF THE AMERICAN OSTEOPATHIC COLLEGE OF DERMATOLOGY Page 1 JOURNAL OF THE AMERICAN OSTEOPATHIC COLLEGE OF DERMATOLOGY 2015-2016 AOCD OFFICERS PRESIDENT Alpesh Desai, DO, FAOCD PRESIDENT-ELECT Karthik Krishnamurthy, DO, FAOCD FIRST VICE-PRESIDENT Daniel Ladd, DO, FAOCD SECOND VICE-PRESIDENT John P. Minni, DO, FAOCD Editor-in-Chief THIRD VICE-PRESIDENT Reagan Anderson, DO, FAOCD Karthik Krishnamurthy, DO SECRETARY-TREASURER Steven Grekin, DO, FAOCD Assistant Editor TRUSTEES Julia Layton, MFA Danica Alexander, DO, FAOCD (2015-2018) Michael Whitworth, DO, FAOCD (2013-2016) Tracy Favreau, DO, FAOCD (2013-2016) David Cleaver, DO, FAOCD (2014-2017) Amy Spizuoco, DO, FAOCD (2014-2017) Peter Saitta, DO, FAOCD (2015-2018) Immediate Past-President Rick Lin, DO, FAOCD EEC Representatives James Bernard, DO, FAOCD Michael Scott, DO, FAOCD Finance Committee Representative Donald Tillman, DO, FAOCD AOBD Representative Michael J. Scott, DO, FAOCD Executive Director Marsha A. Wise, BS AOCD • 2902 N. Baltimore St. • Kirksville, MO 63501 800-449-2623 • FAX: 660-627-2623 • www.aocd.org COPYRIGHT AND PERMISSION: Written permission must be obtained from the Journal of the American Osteopathic College of Dermatology for copying or reprinting text of more than half a page, tables or figures. -

Cytoplasmic Plaque Formation in Hemidesmosome Development Is Dependent on Soxf Transcription Factor Function
Cytoplasmic Plaque Formation in Hemidesmosome Development Is Dependent on SoxF Transcription Factor Function Shelly Oommen1, Mathias Francois2, Maiko Kawasaki1, Melanie Murrell2, Katsushige Kawasaki1, Thantrira Porntaveetus1, Sarah Ghafoor1, Neville J. Young2, Yoshimasa Okamatsu3, John McGrath4, Peter Koopman2, Paul T. Sharpe1, Atsushi Ohazama1,3* 1 Craniofacial Development and Stem Cell Biology, and Biomedical Research Centre, Dental Institute, King’s College London, London, United Kingdom, 2 Institute for Molecular Bioscience, The University of Queensland, Brisbane, Australia, 3 Department of Periodontology, Showa University Dental School, Tokyo, Japan, 4 Genetic Skin Disease Group, St John’s Institute of Dermatology, Division of Skin Sciences, King’s College London, London, United Kingdom Abstract Hemidesmosomes are composed of intricate networks of proteins, that are an essential attachment apparatus for the integrity of epithelial tissue. Disruption leads to blistering diseases such as epidermolysis bullosa. Members of the Sox gene family show dynamic and diverse expression patterns during development and mutation analyses in humans and mice provide evidence that they play a remarkable variety of roles in development and human disease. Previous studies have established that the mouse mutant ragged-opossum (Raop) expresses a dominant-negative form of the SOX18 transcription factor that interferes with the function of wild type SOX18 and of the related SOXF-subgroup proteins SOX7 and 217. Here we show that skin and oral mucosa in homozygous Raop mice display extensive detachment of epithelium from the underlying mesenchymal tissue, caused by tearing of epithelial cells just above the plasma membrane due to hemidesmosome disruption. In addition, several hemidesmosome proteins expression were found to be dysregulated in the Raop mice. -

Brain-To-Cervical Lymph Node Signaling After Stroke
ARTICLE https://doi.org/10.1038/s41467-019-13324-w OPEN Brain-to-cervical lymph node signaling after stroke Elga Esposito1, Bum Ju Ahn1, Jingfei Shi1,2, Yoshihiko Nakamura 1,3, Ji Hyun Park1, Emiri T. Mandeville 1, Zhanyang Yu1, Su Jing Chan 1,4, Rakhi Desai1, Ayumi Hayakawa1, Xunming Ji2, Eng H. Lo1,5*& Kazuhide Hayakawa1,5* After stroke, peripheral immune cells are activated and these systemic responses may amplify brain damage, but how the injured brain sends out signals to trigger systemic inflammation remains unclear. Here we show that a brain-to-cervical lymph node (CLN) 1234567890():,; pathway is involved. In rats subjected to focal cerebral ischemia, lymphatic endothelial cells proliferate and macrophages are rapidly activated in CLNs within 24 h, in part via VEGF-C/ VEGFR3 signalling. Microarray analyses of isolated lymphatic endothelium from CLNs of ischemic mice confirm the activation of transmembrane tyrosine kinase pathways. Blockade of VEGFR3 reduces lymphatic endothelial activation, decreases pro-inflammatory macro- phages, and reduces brain infarction. In vitro, VEGF-C/VEGFR3 signalling in lymphatic endothelial cells enhances inflammatory responses in co-cultured macrophages. Lastly, surgical removal of CLNs in mice significantly reduces infarction after focal cerebral ischemia. These findings suggest that modulating the brain-to-CLN pathway may offer therapeutic opportunities to ameliorate systemic inflammation and brain injury after stroke. 1 Neuroprotection Research Laboratory, Departments of Radiology and Neurology, Massachusetts General Hospital and Harvard Medical School, Charlestown, MA, USA. 2 China-America Institute of Neuroscience, Xuanwu Hospital, Capital Medical University, Beijing, China. 3 Department of Emergency and Critical Care Medicine, Fukuoka University Hospital, Jonan, Fukuoka, Japan. -

Human Autoimmunity and Associated Diseases
Human Autoimmunity and Associated Diseases Human Autoimmunity and Associated Diseases Edited by Kenan Demir and Selim Görgün Human Autoimmunity and Associated Diseases Edited by Kenan Demir and Selim Görgün This book first published 2021 Cambridge Scholars Publishing Lady Stephenson Library, Newcastle upon Tyne, NE6 2PA, UK British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Copyright © 2021 by Kenan Demir and Selim Görgün and contributors All rights for this book reserved. No part of this book may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the copyright owner. ISBN (10): 1-5275-6910-1 ISBN (13): 978-1-5275-6910-2 TABLE OF CONTENTS Preface ...................................................................................................... viii Chapter One ................................................................................................. 1 Introduction to the Immune System Kemal Bilgin Chapter Two .............................................................................................. 10 Immune System Embryology Rümeysa Göç Chapter Three ............................................................................................. 18 Immune System Histology Filiz Yılmaz Chapter Four .............................................................................................. 36 Tolerance Mechanisms and Autoimmunity -

The Diagnosis and Treatment of Peripheral Lymphedema: 2016 Consensus Document of the International Society of Lymphology
170 Lymphology 49 (2016) 170-184 THE DIAGNOSIS AND TREATMENT OF PERIPHERAL LYMPHEDEMA: 2016 CONSENSUS DOCUMENT OF THE INTERNATIONAL SOCIETY OF LYMPHOLOGY This International Society of Lymphology “Consensus” of the international community (ISL) Consensus Document is the latest based on various levels of evidence. The revision of the 1995 Document for the document is not meant to override individual evaluation and management of peripheral clinical considerations for complex patients lymphedema (1). It is based upon modifica- nor to stifle progress. It is also not meant to tions: [A] suggested and published following be a legal formulation from which variations the 1997 XVI International Congress of define medical malpractice. The Society Lymphology (ICL) in Madrid, Spain (2), understands that in some clinics the method discussed at the 1999 XVII ICL in Chennai, of treatment derives from national standards India (3), and considered/ confirmed at the while in others access to medical equipment 2000 (ISL) Executive Committee meeting in and supplies is limited; therefore the suggested Hinterzarten, Germany (4); [B] derived from treatments might be impractical. Adaptability integration of discussions and written and inclusiveness does come at the price that comments obtained during and following the members can rightly be critical of what they 2001 XVIII ICL in Genoa, Italy as modified see as vagueness or imprecision in definitions, at the 2003 ISL Executive Committee meeting qualifiers in the choice of words (e.g., the use in Cordoba, Argentina (5); [C] suggested of “may... perhaps... unclear”, etc.) and from comments, criticisms, and rebuttals as mentions (albeit without endorsement) of published in the December 2004 issue of treatment options supported by limited hard Lymphology (6); [D] discussed in both the data. -

April 2011 Preventiongenetics Newsletter
News from PreventionGenetics IN THIS ISSUE Volume 3, Number 1 New Tests Welcome to the April 2011 PreventionGenetics Newsletter. In New Hires this issue, we present new DNA sequencing tests for 40 President's Corner disorders. In addition, we introduce two new geneticists to our staff. In the President's Corner, Dr. Jim Weber discusses recent progress at PreventionGenetics. QUICK LINKS Our Website Requisition Form New Tests at PreventionGenetics Please follow the gene links for the corresponding test description. · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · Achondrogenesis (SLC26A2) Achondrogenesis Type II-Hypochondrogenesis (COL2A1) Amyotrophic Lateral Sclerosis and Primary Open-Angle Glaucoma (OPTN) Atelosteogenesis (SLC26A2) Camurati-Engelmann Disease (TGFB1) Cartilage-hair Hypoplasia and Related Disorders (RMRP) Chediak-Higashi Syndrome (LYST) Chondrodysplasia Punctata, X-Linked Dominant (EBP) Cleidocranial Dysplasia (RUNX2) Cranioectodermal Dysplasia 1 (IFT122) Diastrophic Dysplasia (SLC26A2) Dilated Cardiomyopathy and Limb-Girdle Muscular Dystrophy Type 2F (SGCD) Dentinogenesis Imperfecta (DSPP) Ellis-van Creveld Syndrome (EVC, EVC2) Emery-Dreifuss Muscular Dystrophy-1 (EMD) Fanconi Anemia (FANCL) Hennekam Lymphangiectasia-Lymphedema (CCBE1) Hereditary Breast Cancer (CHEK2) Hermansky Pudlak Syndrome (HPS1, HPS2/AP3B1, HPS3, HPS4, HPS5, HPS6, HPS7/DTNBP1, HPS8/BLOC1S3) Hirschsprung Disease (RET) Holt-Oram Syndrome (TBX5) Kneist Dysplasia (COL2A1) Lynch Syndrome (PMS2) Menkes Disease and X-Hereditary -

Kraft Washington 0250E 18634.Pdf (12.39Mb)
© Copyright 2018 John Cavin Kraft II Elucidating Mechanisms for Drug Combination Nanoparticles to Enhance and Prolong Lymphatic Exposure: Experimental and Modeling Approaches John Cavin Kraft II A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy University of Washington 2018 Reading Committee: Rodney J. Y. Ho, Chair Kenneth E. Thummel Shiu-Lok Hu Program Authorized to Offer Degree: Pharmaceutics University of Washington Abstract Elucidating Mechanisms for Drug Combination Nanoparticles to Enhance and Prolong Lymphatic Exposure: Experimental and Modeling Approaches John Cavin Kraft II Chair of the Supervisory Committee: Rodney J. Y. Ho Department of Pharmaceutics Human immunodeficiency virus (HIV) infection and metastatic cancers impact over 50 million people worldwide. Because HIV and metastatic cancers exploit the lymphatics to persist and spread, enhanced and prolonged lymphatic exposure to drug combinations is essential for treating these diseases. Unfortunately, many oral and intravenous small molecule drug therapies exhibit limited lymphatic exposure, which can lead to subtherapeutic drug levels and drug resistance. Moreover, most therapeutic strategies and decisions for these diseases are not made with lymphatic drug exposure in mind, largely because accounting for and understanding lymphatic drug levels is complex, and limited tools exist for this. Thus, there is a need for tools to better understand lymphatic drug exposure and for strategies to selectively deliver drug combinations to the lymphatics. We previously developed lymphatic-targeted drug combination nanoparticles (DcNPs), however, the mechanisms that enable DcNPs to target drug combinations to the lymphatics remained to be elucidated. Understanding these mechanisms could open up new therapeutic strategies for treating lymphatic diseases. -
Hand and Arm Guidelines After Your Axillary Lymph Node Dissection
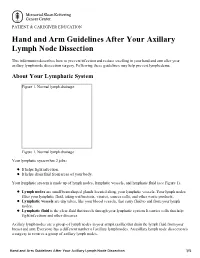
PATIENT & CAREGIVER EDUCATION Hand and Arm Guidelines After Your Axillary Lymph Node Dissection This information describes how to prevent infection and reduce swelling in your hand and arm after your axillary lymph node dissection surgery. Following these guidelines may help prevent lymphedema. About Your Lymphatic System Figure 1. Normal lymph drainage Figure 1. Normal lymph drainage Your lymphatic system has 2 jobs: It helps fight infection. It helps drain fluid from areas of your body. Your lymphatic system is made up of lymph nodes, lymphatic vessels, and lymphatic fluid (see Figure 1). Lymph nodes are small bean-shaped glands located along your lymphatic vessels. Your lymph nodes filter your lymphatic fluid, taking out bacteria, viruses, cancer cells, and other waste products. Lymphatic vessels are tiny tubes, like your blood vessels, that carry fluid to and from your lymph nodes. Lymphatic fluid is the clear fluid that travels through your lymphatic system. It carries cells that help fight infections and other diseases. Axillary lymph nodes are a group of lymph nodes in your armpit (axilla) that drain the lymph fluid from your breast and arm. Everyone has a different number of axillary lymph nodes. An axillary lymph node dissection is a surgery to remove a group of axillary lymph nodes. Hand and Arm Guidelines After Your Axillary Lymph Node Dissection 1/5 About Lymphedema Sometimes, removing lymph nodes can make it hard for your lymphatic system to drain properly. If this happens, lymphatic fluid can build up in the area where the lymph nodes were removed. This extra fluid causes swelling called lymphedema. -

Lymphedema Fact Sheet
Lymphedema Fact Sheet What is lymphedema? Lymphedema is the accumulation of lymphatic fluid that can cause swelling in the arm and/or hand. Lymphatic fluid is normally filtered through the lymph nodes. Removal of lymph nodes requires lymph fluids from the arm to be rerouted and filtered through remaining axillary lymph nodes. Lymphedema occurs in a small number of patients, and symptoms can range from hand swelling alone to total arm swelling. Should you notice any swelling, please contact your surgeon’s office who will instruct you in appropriate follow up care. Intervention includes physical or occupational therapy, manual lymphatic drainage, compression bandaging and garments. New research suggests gradual, progressive strengthening, when cleared by your physician, can actually minimize the risk of lymphedema by dilating, or widening, remaining lymphatic channels around the shoulder and arm. Who is at risk for lymphedema? With a sentinel node biopsy, the lifetime risk of lymphedema is very small and may occur in up to 5% of patients. With an axillary dissection or radiation to the axilla, the lifetime risk is up to 20%. The vast majority of cases of lymphedema related to breast surgery or radiation occur in the first year after treatment. Being overweight can increase your risk. What are the early signs of lymphedema? The early sign of lymphedema is swelling of the arm or hand. Sometimes the arm will feel heavy. Sometimes the first sign is that your sleeve, watch or jewelry feels tighter than usual. Can I prevent lymphedema? While there is no medical evidence that lymphedema can be prevented, below are some recommendations for possible risk reduction: • Maintaining a healthy weight has been shown to reduce risk of lymphedema.