Lymphatic Complaints in the Dermatology Clinic: an Osteopathic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Keratosis Follicularis Spinulosa Decalvans in a Female Child- a Rare Presentation Chowdhury J1, Ghoshal L2, Bannerjee S3
Bangladesh Journal of Medical Science Vol. 16 No. 04 October’17 Case report: Keratosis Follicularis Spinulosa Decalvans in a female child- a rare presentation Chowdhury J1, Ghoshal L2, Bannerjee S3 Abstract: Congenital alopecia universalis is a very rare presentation. A 6 year old girl came to us with total alopecia and multiple horny keratosis pilaris like skin lesions all over the body. The alopecia was mostly non-scarring with a few patches of scarring over the scalp. Histology from scalp revealed follicular plugging with perifollicular infiltrate of lymphocytes and plasma cells. The case was diagnosed as Keratosis follicularis spinulosa decalvans. This is very rare and even rarer in females. Keywords: keratosis pilaris; scarring alopecia; non-scarring alopecia Bangladesh Journal of Medical Science Vol. 16 No. 04 October’17. Page : 591-593 Introduction: Keratosis follicularis spinulosa Except a few brittle hairs on the crown area hair was decalvans is a rare genodermatosis that affects absent all over the scalp, eyelids and body. There predominantly males. It appears in infancy or were a few small patches of non-scarring alopecia childhood, and is characterized by diffuse follicular over the scalp [Figure 3]. keratotic papules associated with progressive Palms, soles, nail and mucosa were unaffected. cicatricial alopecia of the scalp, eyebrows and Family history was unremarkable with no history eyelashes. Family history is often positive. We report of consanguinity. Her twin sister was unaffected. a case of KFSD in a female child. There was no history of photophobia, no evidence Case-report: A 6 year old girl presented with of physical or mental retardation. -

Bilateral Lower Extremity Hyperkeratotic Plaques: a Case Report of Ichthyosis Vulgaris
Faculty & Staff Scholarship 2015 Bilateral lower extremity hyperkeratotic plaques: a case report of ichthyosis vulgaris Hayley Leight Zachary Zinn Omid Jalali Follow this and additional works at: https://researchrepository.wvu.edu/faculty_publications Clinical, Cosmetic and Investigational Dermatology Dovepress open access to scientific and medical research Open Access Full Text Article CASE REPORT Bilateral lower extremity hyperkeratotic plaques: a case report of ichthyosis vulgaris Hayley Leight Abstract: Here, we report a case of a middle-aged woman presenting with severe, long-standing, Zachary Zinn hyperkeratotic plaques of the lower extremities unrelieved by over-the-counter medications. Omid Jalali Initial history and clinical findings were suggestive of an inherited ichthyosis. Ichthyoses are genetic disorders characterized by dry scaly skin and altered skin-barrier function. A diagnosis Department of Dermatology, West Virginia University, of ichthyosis vulgaris was confirmed by histopathology. Etiology, prevalence, and treatment Morgantown, WV, USA options are discussed. Keywords: filaggrin gene, FLG, profilaggrin, keratohyalin granules, hyperkeratosis Introduction For personal use only. Inherited ichthyoses are a diverse group of genetic disorders characterized by dry, scaly skin; hyperkeratosis; and altered skin-barrier function. While these disorders of cutaneous keratinization are multifaceted and varying in etiology, disruption in the stratum corneum with generalized scaling is common to all.1–4 Although not entirely known -

Molecular Mechanisms of Neuroimmune Crosstalk in the Pathogenesis of Stroke
International Journal of Molecular Sciences Review Molecular Mechanisms of Neuroimmune Crosstalk in the Pathogenesis of Stroke Yun Hwa Choi 1, Collin Laaker 2, Martin Hsu 2, Peter Cismaru 3, Matyas Sandor 4 and Zsuzsanna Fabry 2,4,* 1 School of Pharmacy, University of Wisconsin-Madison, Madison, WI 53705, USA; [email protected] 2 Neuroscience Training Program, University of Wisconsin-Madison, Madison, WI 53705, USA; [email protected] (C.L.); [email protected] (M.H.) 3 Chemistry, University of Wisconsin-Madison, Madison, WI 53705, USA; [email protected] 4 Department of Pathology and Laboratory Medicine, University of Wisconsin-Madison, Madison, WI 53705, USA; [email protected] * Correspondence: [email protected] Abstract: Stroke disrupts the homeostatic balance within the brain and is associated with a significant accumulation of necrotic cellular debris, fluid, and peripheral immune cells in the central nervous system (CNS). Additionally, cells, antigens, and other factors exit the brain into the periphery via damaged blood–brain barrier cells, glymphatic transport mechanisms, and lymphatic vessels, which dramatically influence the systemic immune response and lead to complex neuroimmune communi- cation. As a result, the immunological response after stroke is a highly dynamic event that involves communication between multiple organ systems and cell types, with significant consequences on not only the initial stroke tissue injury but long-term recovery in the CNS. In this review, we discuss the complex immunological and physiological interactions that occur after stroke with a focus on how the peripheral immune system and CNS communicate to regulate post-stroke brain homeostasis. First, Citation: Choi, Y.H.; Laaker, C.; Hsu, we discuss the post-stroke immune cascade across different contexts as well as homeostatic regulation M.; Cismaru, P.; Sandor, M.; Fabry, Z. -

Erythrokeratodermia Variabilis Et Progressiva Allelic to Oculo-Dento
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector COMMENTARY See related article on pg 1540 translocated into the plasma membrane. Once expressed on the cell surface, the hemichannel docks with a connexon of an adjacent cell to form a channel that Erythrokeratodermia Variabilis et is termed gap junction. Connexons can form either homotypic (docking of two Progressiva Allelic to Oculo-Dento- identical connexons), heterotypic (docking of two dissimilar homomeric Digital Dysplasia connexons), or heteromeric (docking of two heteromeric connexons) channels Sabine Duchatelet1,2 and Alain Hovnanian1,2,3 (Mese et al., 2007). These diverse Erythrokeratodermia variabilis et progressiva (EKVP) is a genodermatosis with combinations of connexins create clinical and genetic heterogeneity, most often transmitted in an autosomal different types of channels, each having dominant manner, caused by mutations in GJB3 and GJB4 genes encoding unique properties (ionic conductance, connexins (Cx)31 and 30.3, respectively. In this issue, Boyden et al. (2015) report permeability, sensitivity to voltage, or for the first time de novo dominant mutations in GJA1 encoding the ubiquitous pH). Of note, several connexins may also Cx43 in patients with EKVP. These results expand the genetic heterogeneity of form functional nonjunctional hemi- EKVP and the human disease phenotypes associated with GJA1 mutations. They channels, although their physiological disclose that EKVP is allelic to oculo-dento-digital dysplasia, a rare syndrome relevance remains uncertain (Pfenniger previously known to be caused by dominant GJA1 mutations. et al., 2010). Mutations in 11 connexin genes cause a variety of genetic dis- Journal of Investigative Dermatology (2015) 135, 1475–1478. -

Skin Brief Articles
SKIN BRIEF ARTICLES Nab-paclitaxel/gemcitabine Induced Acquired Ichthyosis Adriana Lopez BAa, Joel Shugar MDb, and Mark Lebwohl MDc aColumbia University Vagelos College of Physicians and Surgeons, New York, NY bIcahn School of Medicine at Mount Sinai, Department of Otolaryngology, New York, NY cIcahn School of Medicine at Mount Sinai, Department of Dermatology, New York, NY ABSTRACT The ichthyoses are a diverse group of cutaneous disorders characterized by abnormalities in cornification. The majority of ichthyoses are inherited with childhood presentation and new onset ichthyosis in adulthood warrants further medical evaluation. Though most well recognized for its association with Hodgkin’s disease, acquired ichthyosis (AI) has been linked to a number of inflammatory, autoimmune, and endocrine processes. However, drug- induced AI is exceedingly rare and remains a poorly understood entity. Here we report a case of a male patient who developed AI while receiving nab-paclitaxel plus gemcitabine for treatment of pancreatic adenocarcinoma. months prior, the patient was first seen for INTRODUCTION recurrent, self-healing, pruritic erythematous Acquired ichythyosis (AI) is an uncommon papules. Punch biopsy was performed which non-inherited cutaneous disorder of showed an atypical cellular infiltrate of abnormal keratinization that is most scattered large CD30+ cells with clonal T-cell frequently associated with underlying receptor-β gene rearrangement. Though the malignancy. Drug induced AI is uncommon clinicopathologic diagnosis was most and has been rarely linked to consistent with lymphomatoid papulosis chemotherapeutic agents. Herein, we report (LyP), imaging was pursued to exclude the case of a man with pancreatic extracutaneous lymphoproliferative disease. adenocarcinoma who developed an CT scan incidentally detected a mass in the ichthyosiform eruption upon starting body of the pancreas and biopsy was chemotherapy with nab-paclitaxel plus concordant with pancreatic adenocarcinoma. -

Cytoplasmic Plaque Formation in Hemidesmosome Development Is Dependent on Soxf Transcription Factor Function
Cytoplasmic Plaque Formation in Hemidesmosome Development Is Dependent on SoxF Transcription Factor Function Shelly Oommen1, Mathias Francois2, Maiko Kawasaki1, Melanie Murrell2, Katsushige Kawasaki1, Thantrira Porntaveetus1, Sarah Ghafoor1, Neville J. Young2, Yoshimasa Okamatsu3, John McGrath4, Peter Koopman2, Paul T. Sharpe1, Atsushi Ohazama1,3* 1 Craniofacial Development and Stem Cell Biology, and Biomedical Research Centre, Dental Institute, King’s College London, London, United Kingdom, 2 Institute for Molecular Bioscience, The University of Queensland, Brisbane, Australia, 3 Department of Periodontology, Showa University Dental School, Tokyo, Japan, 4 Genetic Skin Disease Group, St John’s Institute of Dermatology, Division of Skin Sciences, King’s College London, London, United Kingdom Abstract Hemidesmosomes are composed of intricate networks of proteins, that are an essential attachment apparatus for the integrity of epithelial tissue. Disruption leads to blistering diseases such as epidermolysis bullosa. Members of the Sox gene family show dynamic and diverse expression patterns during development and mutation analyses in humans and mice provide evidence that they play a remarkable variety of roles in development and human disease. Previous studies have established that the mouse mutant ragged-opossum (Raop) expresses a dominant-negative form of the SOX18 transcription factor that interferes with the function of wild type SOX18 and of the related SOXF-subgroup proteins SOX7 and 217. Here we show that skin and oral mucosa in homozygous Raop mice display extensive detachment of epithelium from the underlying mesenchymal tissue, caused by tearing of epithelial cells just above the plasma membrane due to hemidesmosome disruption. In addition, several hemidesmosome proteins expression were found to be dysregulated in the Raop mice. -

Epidermolytic Hyperkeratosis with Ichthyosis Hystrix Geromanta Baleviciené, MD, Vilnius, Lithuania Robert A
pediatric dermatology Series Editor: Camila K. Janniger, MD, Newark, New Jersey Epidermolytic Hyperkeratosis With Ichthyosis Hystrix Geromanta Baleviciené, MD, Vilnius, Lithuania Robert A. Schwartz, MD, MPH, Newark, New Jersey Epidermolytic hyperkeratosis (EH) is a congenital, autosomal-dominant genodermatosis characterized by blisters.1,2 Shortly after birth, the infant’s skin becomes red and may show bullae. The erythema regresses, but brown verrucous hyperkeratosis persists, particularly accentuated in the flexures. This condition is also known as bullous ichthyosiform erythroderma. The disorder of keratinization has varied clinical manifestations in the extent of cutaneous involve- ment, palmar and plantar hyperkeratosis, and evi- dence of erythroderma. We describe 5 patients, 4 with EH (one of whom had it in localized form and one of whom had an unusual type of ichthyosis hystrix described by Curth and Macklin3-7). Case Reports FIGURE 1. Seven-year-old girl with EH, demonstrating Patient 1—A 7-year-old girl with a cutaneous erup- erythema and verrucous hyperkeratosis (Patient 1). tion since birth characterized by flaccid bullae vary- ing in size. The palms and soles had intense diffuse keratosis from 1 year of age. Her nails, hair, teeth, and mental state were normal. The patient’s mother (Pa- tient 2) had a similar disorder. Skin biopsy specimens showed the changes of EH, with pronounced cellular vacuolation of the middle and upper portions of the malpighian stratum and large, clear, irregular spaces. Cellular boundaries were indistinct. A thickened granular layer was evident with large, irregularly shaped keratohyalin granules. Ultrastructural study showed tonofilament clumping of the malpighian layer and cytolysis. -

160 Lymphedema in Dengue Fever – an Unreported Case
Downloaded from www.medrech.com “Lymphedema in dengue fever – An unreported case” Medrech ISSN No. 2394-3971 Case Report LYMPHEDEMA IN DENGUE FEVER – AN UNREPORTED CASE Ching Soong Khoo 1* , Wan Yi Leong 1, Rosaida Md Said 1, Suguna Raman 2, Pushpagandy Ramanathan 2, Petrick Periyasamy 3 1. Department of Internal Medicine/ Ampang Hospital/ Jalan Mewah Utara, Taman Pandan Mewah, 68000 Ampang, Selangor, Malaysia 2. Department of Radiology/ Ampang Hospital/ Jalan Mewah Utara, Taman Pandan Mewah, 68000 Ampang, Selangor, Malaysia 3. University Kebangsaan Malaysia Medical Centre/ Jalan Yaacob Latif, Bandar Tun Razak, 56000 Cheras, Kuala Lumpur, Malaysia Submitted on: October 2015 Accepted on: October 2015 For Correspondence Email ID: Abstract Dengue fever is a neglected tropical disease, which is rearing its ugly head in increasing numbers of both morbidities and mortalities in Malaysia. As of August 18, 2015, a total of 76819 dengue cases and 212 dengue deaths have been reported for 2015 according to Malaysian health officials [1]. Atypical presentations of dengue fever are also on the rise, which are underreported or unrecognized due to lack of awareness [2,3,4]. Lymphedema complicating dengue fever has not been reported in any literature. We detail this case to highlight the varied manifestations of dengue fever. Keywords: Dengue fever, lymphedema Introduction Case Report According to the World Health Organization A 38-year-old Nepalese gentleman (WHO), dengue fever is most commonly an presented to the Emergency Department acute febrile illness defined by the presence with fever for three days, arthralgia, of fever and two or more of the following, myalgia, persistent vomiting, epigastric pain retro-orbital or ocular pain, headache, rash, and productive coughs. -

Hereditary Hearing Impairment with Cutaneous Abnormalities
G C A T T A C G G C A T genes Review Hereditary Hearing Impairment with Cutaneous Abnormalities Tung-Lin Lee 1 , Pei-Hsuan Lin 2,3, Pei-Lung Chen 3,4,5,6 , Jin-Bon Hong 4,7,* and Chen-Chi Wu 2,3,5,8,* 1 Department of Medical Education, National Taiwan University Hospital, Taipei City 100, Taiwan; [email protected] 2 Department of Otolaryngology, National Taiwan University Hospital, Taipei 11556, Taiwan; [email protected] 3 Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei City 100, Taiwan; [email protected] 4 Graduate Institute of Medical Genomics and Proteomics, National Taiwan University College of Medicine, Taipei City 100, Taiwan 5 Department of Medical Genetics, National Taiwan University Hospital, Taipei 10041, Taiwan 6 Department of Internal Medicine, National Taiwan University Hospital, Taipei 10041, Taiwan 7 Department of Dermatology, National Taiwan University Hospital, Taipei City 100, Taiwan 8 Department of Medical Research, National Taiwan University Biomedical Park Hospital, Hsinchu City 300, Taiwan * Correspondence: [email protected] (J.-B.H.); [email protected] (C.-C.W.) Abstract: Syndromic hereditary hearing impairment (HHI) is a clinically and etiologically diverse condition that has a profound influence on affected individuals and their families. As cutaneous findings are more apparent than hearing-related symptoms to clinicians and, more importantly, to caregivers of affected infants and young individuals, establishing a correlation map of skin manifestations and their underlying genetic causes is key to early identification and diagnosis of syndromic HHI. In this article, we performed a comprehensive PubMed database search on syndromic HHI with cutaneous abnormalities, and reviewed a total of 260 relevant publications. -

Mutation and Expression of Abca12in Keratosis Pilaris and Nevus
MOLECULAR MEDICINE REPORTS 18: 3153-3158, 2018 Mutation and expression of ABCA12 in keratosis pilaris and nevus comedonicus FEN LIU1,2*, YAO YANG1,3*, YAN ZHENG1,3, YAN-HUA LIANG1,3 and KANG ZENG1 1Department of Dermatology, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong 510515; 2Department of Histology and Embryology, Institute of Neuroscience, School of Basic Medical Sciences, Wenzhou Medical University, Wenzhou, Zhejiang 325035; 3Department of Dermatology, Shenzhen Hospital, Southern Medical University, Shenzhen, Guangdong 518100, P.R. China Received June 22, 2017; Accepted April 17, 2018 DOI: 10.3892/mmr.2018.9342 Abstract. Keratosis pilaris (KP) and nevus comedonicus Introduction (NC) are congenital keratinized dermatoses; however, the exact etiology of these two diseases is unclear. The objective Keratosis pilaris (KP; OMIM #604093), also known as of the present study was to identify the disease-causing genes lichen pilaris, is a benign genodermatosis that is estimated and their association with functional alterations in the devel- to effect ~40% of the population (1). KP is characterized by opment of KP and NC. Peripheral blood samples of one KP the presence of symmetric, asymptomatic and grouped kera- family, two NC families and 100 unrelated healthy controls totic follicular papules with varying degrees of perifollicular were collected. The genomic sequences of 147 genes associ- erythema. KP lesions often involve the proximal and extended ated with 143 genetic skin diseases were initially analyzed parts of extremities, the cheeks and the buttocks (2). Cases from the KP proband using a custom-designed GeneChip. A may be generalized or unilateral (2). Most patients develop KP novel heterozygous missense mutation in the ATP-binding in their childhood, with a peak in incidence during adoles- cassette sub-family A member 12 (ABCA12) gene, designated cence (3). -

April 2011 Preventiongenetics Newsletter
News from PreventionGenetics IN THIS ISSUE Volume 3, Number 1 New Tests Welcome to the April 2011 PreventionGenetics Newsletter. In New Hires this issue, we present new DNA sequencing tests for 40 President's Corner disorders. In addition, we introduce two new geneticists to our staff. In the President's Corner, Dr. Jim Weber discusses recent progress at PreventionGenetics. QUICK LINKS Our Website Requisition Form New Tests at PreventionGenetics Please follow the gene links for the corresponding test description. · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · Achondrogenesis (SLC26A2) Achondrogenesis Type II-Hypochondrogenesis (COL2A1) Amyotrophic Lateral Sclerosis and Primary Open-Angle Glaucoma (OPTN) Atelosteogenesis (SLC26A2) Camurati-Engelmann Disease (TGFB1) Cartilage-hair Hypoplasia and Related Disorders (RMRP) Chediak-Higashi Syndrome (LYST) Chondrodysplasia Punctata, X-Linked Dominant (EBP) Cleidocranial Dysplasia (RUNX2) Cranioectodermal Dysplasia 1 (IFT122) Diastrophic Dysplasia (SLC26A2) Dilated Cardiomyopathy and Limb-Girdle Muscular Dystrophy Type 2F (SGCD) Dentinogenesis Imperfecta (DSPP) Ellis-van Creveld Syndrome (EVC, EVC2) Emery-Dreifuss Muscular Dystrophy-1 (EMD) Fanconi Anemia (FANCL) Hennekam Lymphangiectasia-Lymphedema (CCBE1) Hereditary Breast Cancer (CHEK2) Hermansky Pudlak Syndrome (HPS1, HPS2/AP3B1, HPS3, HPS4, HPS5, HPS6, HPS7/DTNBP1, HPS8/BLOC1S3) Hirschsprung Disease (RET) Holt-Oram Syndrome (TBX5) Kneist Dysplasia (COL2A1) Lynch Syndrome (PMS2) Menkes Disease and X-Hereditary -
Hand and Arm Guidelines After Your Axillary Lymph Node Dissection
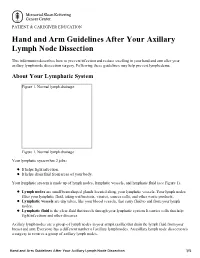
PATIENT & CAREGIVER EDUCATION Hand and Arm Guidelines After Your Axillary Lymph Node Dissection This information describes how to prevent infection and reduce swelling in your hand and arm after your axillary lymph node dissection surgery. Following these guidelines may help prevent lymphedema. About Your Lymphatic System Figure 1. Normal lymph drainage Figure 1. Normal lymph drainage Your lymphatic system has 2 jobs: It helps fight infection. It helps drain fluid from areas of your body. Your lymphatic system is made up of lymph nodes, lymphatic vessels, and lymphatic fluid (see Figure 1). Lymph nodes are small bean-shaped glands located along your lymphatic vessels. Your lymph nodes filter your lymphatic fluid, taking out bacteria, viruses, cancer cells, and other waste products. Lymphatic vessels are tiny tubes, like your blood vessels, that carry fluid to and from your lymph nodes. Lymphatic fluid is the clear fluid that travels through your lymphatic system. It carries cells that help fight infections and other diseases. Axillary lymph nodes are a group of lymph nodes in your armpit (axilla) that drain the lymph fluid from your breast and arm. Everyone has a different number of axillary lymph nodes. An axillary lymph node dissection is a surgery to remove a group of axillary lymph nodes. Hand and Arm Guidelines After Your Axillary Lymph Node Dissection 1/5 About Lymphedema Sometimes, removing lymph nodes can make it hard for your lymphatic system to drain properly. If this happens, lymphatic fluid can build up in the area where the lymph nodes were removed. This extra fluid causes swelling called lymphedema.