Neuroinflammation New Insights Into Beneficial and Detrimental Functions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Huda Y. Zoghbi, MD, Howard Hughes Medical Institute, Jan and Dan Duncan Neurological Research Institute at Texas Children’S Hospital and Baylor College of Medicine
Investigator Spotlight: Huda Y. Zoghbi, MD, Howard Hughes Medical Institute, Jan and Dan Duncan Neurological Research Institute at Texas Children’s Hospital and Baylor College of Medicine It is hard to believe that the 7th World Rett Syndrome Congress has come and gone with great success! Now with summer upon us, IRSF continues to move the spotlight to the committed scientists who have made the World Congress an impressive, high quality meeting with outstanding presentations and discussions. This month we are honored to focus on Dr. Huda Zoghbi who had co-chaired the Basic Research Symposium at the World Congress along with Dr. Gail Mandel. Together, they had produced an exciting lineup of speakers who were encouraged to present new, unpublished data in an effort to foster new ideas that will help chart the course for Rett syndrome research. Dr. Zoghbi is a Howard Hughes Medical Institute (HHMI) Investigator, the Director of the Jan and Dan Duncan Neurological Research Institute at Texas Children’s Hospital, and Professor of the Baylor College of Medicine in Houston, TX. She received her medical degree from Meharry Medical College and completed residency training in pediatrics and neurology at Baylor College of Medicine where she encountered her first Rett syndrome patient in 1983. Dr. Zoghbi was inspired to receive additional research training in the area molecular genetics and upon completion she joined the faculty of Baylor College of Medicine. In 1999, Dr. Zoghbi and collaborators including research fellow Ruthie Amir made a major breakthrough for Rett syndrome. They had discovered that mutations in MECP2, the gene encoding methyl-CpG-binding protein 2, causes Rett syndrome. -

UC San Diego UC San Diego Electronic Theses and Dissertations
UC San Diego UC San Diego Electronic Theses and Dissertations Title Spinocerebellar Ataxia Type 7 is Characterized by Defects in Mitochondrial and Metabolic Function Permalink https://escholarship.org/uc/item/02b7m809 Author Ward, Jacqueline Marie Publication Date 2016 Supplemental Material https://escholarship.org/uc/item/02b7m809#supplemental Peer reviewed|Thesis/dissertation eScholarship.org Powered by the California Digital Library University of California UNIVERSITY OF CALIFORNIA, SAN DIEGO Spinocerebellar Ataxia Type 7 is Characterized by Defects in Mitochondrial and Metabolic Function A dissertation submitted in partial satisfaction of the requirements for the degree Doctor of Philosophy in Biomedical Sciences by Jacqueline Marie Ward Committee in charge: Professor Albert La Spada, Chair Professor Eric Bennett Professor Lawrence Goldstein Professor Alysson Muotri Professor Miles Wilkinson 2016 Copyright Jacqueline Marie Ward, 2016 All rights reserved The Dissertation of Jacqueline Marie Ward is approved, and it is acceptable in quality and form for publication on microfilm and electronically: Chair University of California, San Diego 2016 iii DEDICATION This work is dedicated to my grandfather, Dr. Wayne Ward, the kindest person I’ve ever known. His memory inspires me to be a better person daily. iv TABLE OF CONTENTS SIGNATURE PAGE .......................................................................................... iii DEDICATION .................................................................................................. -
Program Book
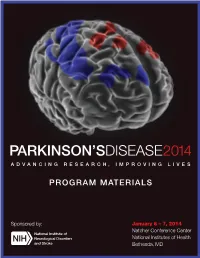
PARKINSON’SDISEASE2014 ADVANCING RESEARCH, IMPROVING LIVES PROGRAM MATERIALS Sponsored by: January 6 – 7, 2014 Natcher Conference Center National Institutes of Health Bethesda, MD About our cover: The program cover image is a stylized version of the Parkinson’s Disease Motor-Related Pattern (PDRP), an abnormal pattern of regional brain function observed in MRI studies which shows increased metabolism indicated by red in some brain regions (pallidothalamic, pontine, and motor cortical areas), and decreased metabolism indicated by blue in others (associated lateral premotor and posterior parietal areas). Original image used with permission of David Eidelberg, M.D. For further information see: Hirano et al., Journal of Neuroscience 28 (16): 4201-4209. Welcome Message from Dr. Story C. Landis Welcome to the National Institute of Neurological Disorders and Stroke (NINDS) conference, “Parkinson’s Disease 2014: Advancing Research, Improving Lives.” Remarkable new discoveries and technological advances are rapidly changing the way we study the biological mechanisms of Parkinson’s disease, identify paths to improved treatments, and design effective clinical trials. Elucidating mechanisms and developing and testing effective interventions require a diverse set of approaches and perspectives. The NINDS has organized this conference with the primary goal of seeking consensus on, and prioritizing, research recommendations spanning clinical, translational, and basic Parkinson’s disease research that we support. We have assembled a stellar and dedicated group of session chairs and panelists who have worked collaboratively to identify emerging research opportunities in Parkinson’s research. While we have divided our working groups into three main research areas, we expect each will inform the others over the course of the next two days, and we look forward to both complementary and unique perspectives. -

Huda Zoghbi: Taking Genetic Inquiry to the Next Level
Spectrum | Autism Research News https://www.spectrumnews.org NEWS, PROFILES Huda Zoghbi: Taking genetic inquiry to the next level BY RACHEL ZAMZOW 25 JUNE 2021 Listen to this story: Most mornings, Huda Zoghbi, 67, climbs a glass-encased, curling staircase to reach her lab on the top and 13th floor of the Jan and Dan Duncan Neurological Research Institute in Houston, Texas. The twisting glass tower, which she designed with a team of architects, echoes the double helix of DNA — a structure that has been central to her career-long quest to uncover genes underlying neurological conditions. As the institute’s director — and as a scientist— she is known for going beyond the standard job description. Genetics researchers often cast a wide net and sequence thousands of genes at a time. But in her prolific career, Zoghbi has focused on a handful of genes, methodically building up an understanding of their function one careful step at a time. Thanks to that approach, Zoghbi has made a number of landmark discoveries, including identifying the genetic roots of Rett syndrome, an autism-related condition that primarily affects girls, as well as the genetic mutations that spur spinocerebellar ataxia, a degenerative motor condition. She has authored more than 350 journal articles. Her accomplishments have earned her almost every major biology and neuroscience research award, including the prestigious Breakthrough Prize in 2017 and the Brain Prize in 2020. “She’s clearly the international leader in the field,” said the late Stephen Warren, professor of human genetics at Emory University in Atlanta, Georgia. Zoghbi never set out to lead a large research center, she says — her heart is in the lab. -
2016 Joint Meeting Program
April 15 – 17, 2016 Fairmont Chicago Millennium Park • Chicago, Illinois The AAP/ASCI/APSA conference is jointly provided by Boston University School of Medicine and AAP/ASCI/APSA. Meeting Program and Abstracts www.jointmeeting.org www.jointmeeting.org Special Events at the 2016 AAP/ASCI/APSA Joint Meeting Friday, April 15 Saturday, April 16 ASCI President’s Reception ASCI Food and Science Evening 6:15 – 7:15 p.m. 6:30 – 9:00 p.m. Gold Room The Mid-America Club, Aon Center ASCI Dinner & New Member AAP Member Banquet Induction Ceremony (Ticketed guests only) (Ticketed guests only) 7:00 – 10:00 p.m. 7:30 – 9:45 p.m. Imperial Ballroom, Level B2 Rouge, Lobby Level How to Solve a Scientific Puzzle: Speaker: Clara D. Bloomfield, MD Clues from Stockholm and Broadway The Ohio State University Comprehensive Cancer Center Speaker: Joe Goldstein, MD APSA Welcome Reception & University of Texas Southwestern Medical Center at Dallas Presidential Address APSA Dinner (Ticketed guests only) 9:00 p.m. – Midnight Signature Room, 360 Chicago, 7:30 – 9:00 p.m. John Hancock Center (off-site) Rouge, Lobby Level Speaker: Daniel DelloStritto, APSA President Finding One’s Scientific Niche: Musings from a Clinical Neuroscientist Speaker: Helen Mayberg, MD, Emory University Dessert Reception (open to all attendees) 10:00 p.m. – Midnight Imperial Foyer, Level B2 Sunday, April 17 APSA Future of Medicine and www.jointmeeting.org Residency Luncheon Noon – 2:00 p.m. Rouge, Lobby Level 2 www.jointmeeting.org Program Contents General Program Information 4 Continuing Medical Education Information 5 Faculty and Speaker Disclosures 7 Scientific Program Schedule 9 Speaker Biographies 16 Call for Nominations: 2017 Harrington Prize for Innovation in Medicine 26 AAP/ASCI/APSA Joint Meeting Faculty 27 Award Recipients 29 Call for Nominations: 2017 Harrington Scholar-Innovator Award 31 Call for Nominations: George M. -
Noninvasive Evaluation of Myocardial Ischemia and Left Ventricular Function
Linköping University Medical Dissertations No. 1109 Noninvasive Evaluation of Myocardial Ischemia and Left Ventricular Function Eva Maret Division of Cardiovascular Medicine Department of Medical and Health Sciences Linköping University, Sweden Linköping 2009 Eva Maret, 2009 Cover picture/illustration: William Björklund Published articles have been reprinted with the permission of the copyright holder. Printed in Sweden by LiU-Tryck, Linköping, Sweden, 2009 ISBN 978-91-7393-675-0 ISSN 0345-0082 To Martin and John! Somewhere over the rainbow Way up high, There's a land that I heard of Once in a lullaby. Somewhere over the rainbow Skies are blue, And the dreams that you dare to dream Really do come true. From “The Wizard of OZ”, music by Harold Arlen and lyrics by E.Y. Harburg CONTENTS POPULÄRVETENSKAPLIG SAMMANFATTNING ................................................................ 7 LIST OF PUBLICATIONS .......................................................................................................... 9 INTRODUCTION ....................................................................................................................... 13 Coronary Artery Disease ........................................................................................................ 13 Coronary flow, resistance and flow reserve ........................................................................... 14 Coronary atherosclerosis and myocardial infarction .............................................................. 15 Left ventricular function -

Chapter 1: Stroke and Neuroprotection 1 – 21
DEVELOPMENT OF NOVEL THERAPEUTICS FOR STROKE: PRECLINICAL INVESTIGATIONS OF OSTEOPONTIN AND 3-IODOTHYRONAMINE By Kristian Paul Doyle A DISSERTATION Presented to the Department of Molecular Microbiology & Immunology at the Oregon Health & Science University in partial fulfillment of the requirements for the degree of Doctor of Philosophy 1 CONTENTS List of Figures v List of Tables ix Acknowledgements x Preface xi Abstract xii List of Abbreviations xv Chapter 1: Stroke and Neuroprotection 1 – 21 1.1 Introduction 2 1.2 Brief History of Stroke 2 1.3 Stroke Pathophysiology 4 1.4 Neuroprotection 17 1.5 Ischemic Preconditioning 19 1.6 Research Goal 21 Chapter 2: Osteopontin 22-86 2.1 An Introduction to OPN 23 2.2 The Structure of OPN 23 2.3 OPN, Integrins and Survival Signaling 25 2.4 OPN and Ischemic Injury 27 2.5 Preclinical Development of OPN 33 2.6 Optimizing Delivery 33 2 2.7 Improving the Potency of OPN 36 2.8 Identifying the Regions of OPN required for Neuroprotection 36 2.9 Hypothesis 37 2.10 Research Design 38 2.11 OPN has neuroprotective capability in vivo and in vitro 40 2.12 The mechanism of neuroprotection by OPN 51 2.13 OPN can be delivered to the brain by intranasal administration 56 2.14 Enhancing the neuroprotective capability of OPN 60 2.15 Peptides based on the N and C terminal fragment of thrombin cleaved OPN are neuroprotective 65 2.16 The C terminal peptide requires phosphorylation to be neuroprotective while the N terminal peptide does not require phosphorylation 70 2.17 Dose response and time window of NT 124-153 71 2.18 -
An Eye to the Future Advances in Imaging Are Accelerating the Pace of Biological Discovery
fall 2007 An Eye to the Future Advances in imaging are accelerating the pace of biological discovery. A new cellular imaging initiative at the University has researchers seeing small and thinking big. story on page 8 p r o f i l e s college News c l a s s N o t e s from the dean Where curiosity- and solution- driven science meet ome scientists are driven by a curiosity to under- As a curiosity-driven college, it’s CBS’ job to keep S stand how life works—from molecules to eco- adding to the foundation of knowledge that supports systems—and to add to the world’s collective body of translational and solution-driven science in other col- knowledge. Others are searching for a puzzle piece leges. As such, we are the stewards of the foundational that may yield a better way to treat cancer, produce disciplines in the biological sciences: biochemistry, food or create renewable forms of energy. molecular biology, genetics, cell biology and develop- ment, ecology, plant biology, etc. Both are essential, and there is plenty of overlap Robert Elde, Dean between the two. Curiosity-driven research often turns In order to keep fueling translational and solution- up a bit of information that has immediate applications driven research, we need to infuse foundational disci- in medicine, agriculture or engineering. By the same plines with new technologies and other opportunities token, solution-driven research can add to knowledge. as science evolves. And some scientists travel between these two worlds. Fall 07 Vol. 5 No. 3 Cellular imaging, the subject of our cover story, is one As a whole, College of Biological Sciences faculty of those opportunities. -
View Final Program
142nd ANNUAL MEETING OF THE AMERICAN ANA2017 NEUROLOGICAL ASSOCIATION SAN DIEGO, CA • OCTOBER 15-17, 2017 SHERATON SAN DIEGO HOTEL & MARINA EXPLORE • EXAMINE • INVESTIGATE FINAL PROGRAM OCTOBER 14, 2017 | Pre-Meeting Symposium: Big Science and the BRAIN Initiative 2017.MYANA.org 142nd ANNUAL MEETING OF THE AMERICAN ANA2017 NEUROLOGICAL ASSOCIATION SAN DIEGO, CA • OCTOBER 15 -17, 2017 SHERATON SAN DIEGO HOTEL & MARINA ND Please note some session titles may have changed since this program was printed. Please refer THE 142 ANA to your Mobile app for the most current session updates. ANNUAL MEETING LETTER FROM THE CHAIR 3 Enjoy outstanding scientific SCHEDULE AT A GLANCE 4 symposia covering the latest HOTEL FLOOR PLANS 6 research in the fields of neurology and neuroscience GENERAL INFORMATION 7 while taking the opportunity WIRELESS CONNECTION 8 to network with leaders in the world of academic neurology CONTINUING MEDICAL EDUCATION 8 at the 142nd ANA Annual ANNUAL MEETING MOBILE APP 8 Meeting in San Diego, CA, October 15-17, 2017. PROGRAMS BY DAY 9 SATURDAY OCT 14 9 MEETING LOCATION SUNDAY OCT 15 9 Sheraton San Diego MONDAY OCT 16 17 Hotel & Marina 1380 Harbor Island Drive TUESDAY OCT 17 25 San Diego, California 92101 IN MEMORIAM 28 ONSITE MEETING CONTACTS SPEAKER ABSTRACTS 29 Registration and meeting questions: THANK YOU TO OUR SUPPORTERS & EXHIBITORS 42 [email protected] FUTURE MEETING DATES 42 OR visit the registration desk Bay View Foyer 2017 AWARDEES 43 (located in Marina Tower Lobby Level) ACADEMIC NEUROLOGY REPRESENTATIVES FROM JAPAN 47 Saturday, October 14 2017 ABSTRACT REVIEWERS 48 3:00 PM–7:00 PM BOARD OF DIRECTORS 49 Sunday, October 15 6:00 AM–5:45 PM ANA 2017 COMMITTEES, SUBCOMMITTEES & TASK FORCES 50 Monday, October 16 6:30 AM–5:45 PM Tuesday, October 17 6:30 AM–2:15 PM #ANAMTG2017 ANA 2017 FROM THE CHAIR Dear Colleagues, It is a pleasure to welcome you to the 142nd Annual Meeting of the American Neurological Association (ANA). -

Immune Senescence and Brain Aging: Can Rejuvenation of Immunity Reverse Memory Loss?
Opinion Immune senescence and brain aging: can rejuvenation of immunity reverse memory loss? Noga Ron-Harel and Michal Schwartz Department of Neurobiology, The Weizmann Institute of Science, 76100, Rehovot, Israel The factors that determine brain aging remain a mystery. assisting in its restoration [2–8]. In this article, we suggest Do brain aging and memory loss reflect processes occur- a model that attributes to age-related immune compromise ring only within the brain? Here, we present a novel a role in age-related brain dysfunction and, specifically, in view, linking aging of adaptive immunity to brain senes- hippocampus-dependent memory deterioration. According cence and specifically to spatial memory deterioration. to this view, during old age, when the need for maintenance Inborn immune deficiency, in addition to sudden impo- increases, the senescent immune system fails to provide sition of immune malfunction in young animals, results the support required. The individual onset and rate of age- in cognitive impairment. As a corollary, immune restor- related memory impairments are determined both by the ation at adulthood or in the elderly results in a reversal of baseline of cognitive ability (i.e. intelligence) and the rate memory loss. These results, together with the known of cognitive aging [9]. We suggest that the latter is deter- deterioration of adaptive immunity in the elderly, mined by the subject’s immune potential at old age, in suggest that memory loss does not solely reflect chrono- addition to other known factors including early education logical age; rather, it is an outcome of the gap between and lifelong dietary habits [10–12]. -

College Catalog 2011–2012
1 College Catalog 2011–2012 - BOSTON | WORCESTER | MANCHESTER, NH This catalog is intended to provide working guidelines and descriptions of the general and academic policies of the College applicable to students. It is not intended and cannot be Massachusetts College of Pharmacy and Health Sciences construed as a contract or guaranty of any kind, express or implied, and the College may 179 Longwood Avenue, Boston, Massachusetts 02115 change, delete or add to these guidelines unilaterally in its sole discretion and without notice. The College also reserves the right to determine the applicability of any policy to a particular Telephone 617.732.2800; students outside Massachusetts and within the continental United situation or set of circumstances and to depart from the guidelines contained herein in States may call toll free 1.800.225.5506. Non-Discrimination Policy a given case. This catalog supersedes any previous catalog, policies or practices relating It is the policy and commitment of Massachusetts College of Pharmacy and Health Sciences 2 to students. It is the responsibility of the students to know and understand the College’s 3 not to discriminate on the basis of race, religion, color, age, sexual orientation, sex, sexual policies. The College may from time to time acquire or develop new programs, or expand its identity, disability, veteran status, marital status or national origin in its educational pro- offerings in other locations, including distance learning programs, and the guidelines in this grams, activities, admissions or employment policies and to actively comply with the require- ments of Federal Executive Orders 11246 and 11375 as amended; the Civil Rights Act of catalog shall apply to all such programs and locations. -
Ischemia and Reperfusion Injury: When Cells Almost Die
Peer Reviewed CE Article #1 Ischemia and Reperfusion Injury: When Cells Almost Die Amy N. Breton, CVT, VTS (ECC) Veterinary Emergency and Specialty Center of New England Waltham, Massachusetts schemia is defined as inadequate blood supply to a part ing energy for metabolism within cells.3 One of the fastest of the body, usually caused by partial or total block- ways that ATP is produced is by oxidative phosphorylation, age of an artery. Reperfusion injury occurs when tissue which, as the name implies, requires oxygen.3 Despite the I 3 perfusion and oxygenation are restored to an area that has importance of ATP, cells do not stockpile ATP. They only been affected by an ischemic event. make what they need for a particular time. When ischemia Ischemia/reperfusion (I/R) injury is a complex cascade occurs, oxygenation of cells ceases, resulting in anaerobic of events resulting in devastating effects on the body, ATP production, which is less efficient.3 sometimes including death. Despite more than 70 years of When oxygen becomes unavailable, cells begin anaero- research, I/R injury is not fully understood. Events such as bic glycolysis. This process can be a lifesaving way for cells gastric dilatation–volvulus (GDV), mesenteric torsion, or to obtain energy; however, it is extremely wasteful. During strangulation of a limb can lead to I/R injury. It is important anaerobic glycolysis, pyruvic acid and hydrogen atoms for all veterinary personnel to understand I/R injury so that combine with nicotinamide adenine dinucleotide (NAD) treatment and prevention can begin as early as possible. to form NADH and H+.3 If the buildup of NADH and H+ within cells becomes too great, the anaerobic process stops, The Ischemic Cascade terminating energy production.3 However, NADH and H+ The chain of events involved in I/R injury can be broken combine to form lactic acid, which diffuses from cells rap- down into the ischemic cascade (BOX 1) and reperfusion idly so that the process can continue.3 Although this is not injury (BOX 2).