Redalyc.Toxoplasmosis As a Cause of Subacute Thyroiditis in Dogs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Subacute Thyroiditis with Non-Toxic Hyperfunctioning Thyroid Nodules
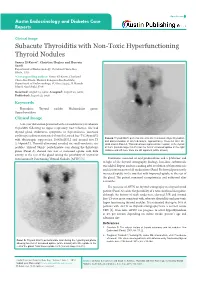
Open Access Austin Endocrinology and Diabetes Case Reports Clinical Image Subacute Thyroiditis with Non-Toxic Hyperfunctioning Thyroid Nodules Samer El-Kaissi*, Christine Hughes and Hussein Saadi Department of Endocrinology, Cleveland Clinic Abu Dhabi, UAE *Corresponding author: Samer El-Kaissi, Cleveland Clinic Abu Dhabi, Medical Subspecialties Institute, Department of Endocrinology, PO Box 112412, Al Maryah Island, Abu Dhabi, UAE Received: August 15, 2016; Accepted: August 22, 2016; Published: August 23, 2016 Keywords Thyroiditis; Thyroid nodule; Multinodular goitre; Hyperthyroidism Clinical Image A 46-year old woman presented with a 4-week history of subacute Thyroiditis following an upper respiratory tract infection. She had thyroid gland tenderness, symptoms of thyrotoxicosis, increased erythrocyte sedimentation rate [45mm/hr], raised free-T4 [29pmol/L] Panel B: Thyroid 99mTc pertechnetate scan after resolution of hyperthyroidism with thyrotropin suppression [0.005mIU/L] and normal free-T3 and discontinuation of all medications, approximately 10-weeks after the [5.64pmol/L]. Thyroid ultrasound revealed six small-moderate size initial scan in Panel A. This scan shows improved tracer uptake in the thyroid nodules. Thyroid 99mTc pertechnetate scan during the thyrotoxic at 0.6% (normal range 0.2-3%) but the foci of increased uptake in the right phase (Panel A) showed two foci of increased uptake with little midzone and left lower zone are still apparent (white arrows). activity in the rest of the gland raising the possibility of coexistent Autonomously Functioning Thyroid Nodules [AFTN] [1]. Treatment consisted of oral prednisolone and a β-blocker and in light of the thyroid scintigraphy findings, low-dose carbimazole was added. Repeat nuclear scanning after resolution of thyrotoxicosis and discontinuation of all medications (Panel B) showed persistently increased uptake in the two foci with improved uptake in the rest of the gland. -

Disease/Medical Condition
Disease/Medical Condition HYPOTHYROIDISM Date of Publication: January 27, 2017 (also known as “underactive thyroid disease”; includes congenital hypothyroidism [also known as “neonatal hypothyroidism”] and Hashimoto’s thyroiditis [also known as “autoimmune thyroiditis”]; may manifest as “cretinism” [if onsets during fetal or early life; also known as “congenital myxedema”] or “myxedema” [if onset occurs in older children and adults]) Is the initiation of non-invasive dental hygiene procedures* contra-indicated? No. ◼ Is medical consult advised? – Yes, if previously undiagnosed hypothyroidism or enlarged (or shrunken) thyroid gland is suspected1, in which case the patient/client should see his/her primary care physician. Detection early in childhood can prevent permanent intellectual impairment. – Yes, if previously diagnosed hypothyroidism is suspected to be undermedicated (with manifest signs/symptoms of hypothyroidism) or overmedicated (with manifest signs/symptoms of hyperthyroidism2), in which case the patient/client should see his/her primary care physician or endocrinologist. Major stress or illness sometimes necessitates an increase in prescribed thyroid hormone. Is the initiation of invasive dental hygiene procedures contra-indicated?** Possibly, depending on the certainty of diagnosis and level of control. ◼ Is medical consult advised? – See above. ◼ Is medical clearance required? – Yes, if undiagnosed or severe hypothyroidism is suspected. ◼ Is antibiotic prophylaxis required? – No. ◼ Is postponing treatment advised? – Yes, if undiagnosed hypothyroidism is suspected (necessitating medical assessment/management) or severe hypothyroidism is suspected (necessitating urgent medical assessment/management in order to avoid risk of myxedema coma). In general, the patient/client with mild symptoms of untreated hypothyroidism is not in danger when receiving dental hygiene therapy, and the well managed (euthyroid) patient/client requires no special regard. -

Hashimoto Thyroiditis
Hashimoto thyroiditis Description Hashimoto thyroiditis is a condition that affects the function of the thyroid, which is a butterfly-shaped gland in the lower neck. The thyroid makes hormones that help regulate a wide variety of critical body functions. For example, thyroid hormones influence growth and development, body temperature, heart rate, menstrual cycles, and weight. Hashimoto thyroiditis is a form of chronic inflammation that can damage the thyroid, reducing its ability to produce hormones. One of the first signs of Hashimoto thyroiditis is an enlargement of the thyroid called a goiter. Depending on its size, the enlarged thyroid can cause the neck to look swollen and may interfere with breathing and swallowing. As damage to the thyroid continues, the gland can shrink over a period of years and the goiter may eventually disappear. Other signs and symptoms resulting from an underactive thyroid can include excessive tiredness (fatigue), weight gain or difficulty losing weight, hair that is thin and dry, a slow heart rate, joint or muscle pain, and constipation. People with this condition may also have a pale, puffy face and feel cold even when others around them are warm. Affected women can have heavy or irregular menstrual periods and difficulty conceiving a child ( impaired fertility). Difficulty concentrating and depression can also be signs of a shortage of thyroid hormones. Hashimoto thyroiditis usually appears in mid-adulthood, although it can occur earlier or later in life. Its signs and symptoms tend to develop gradually over months or years. Frequency Hashimoto thyroiditis affects 1 to 2 percent of people in the United States. -

SUBACUTE THYROIDITIS by SELWYN TAYLOR, M.CH., F.R.C.S
Postgrad Med J: first published as 10.1136/pgmj.33.381.327 on 1 July 1957. Downloaded from 327 SUBACUTE THYROIDITIS By SELWYN TAYLOR, M.CH., F.R.C.S. Surgeon, King's College Hospital, Belgrave Hospitalfor Children, and Hammersmith Hospital; Lecturer in Surgery, Postgraduate Medical School of London The term ' thyroiditis ' implies inflammation of to become much more common in that particular the thyroid gland, but by long usage it has come clinic. I had never seen an example before I950, to be used for a number of conditions in which but saw six in the next three years and pro- infection or trauma play apparently no part. Sub- gressively more each year since then. The con- acute thyroiditis is the title given to a condition dition is much commoner in women than men in which was first clearly described by de Quervain the ratio of about six to one. It has not yet been in I904 and which has been rediscovered, or re- reported in a child and is commonest in the fourth described, on a number of occasions since then, and fifth decades, although I have seen it in a with the result that it now has a multiplicity of student teacher of twenty-one. In our own series different names: granulomatous thyroiditis, giant- there was a history of a pre-existing goitre in 50 cell thyroiditis, pseudotuberculous thyroiditis, per cent. of the patients. The incidence, compared creeping thyroiditis, struma granulomatosa, acute with that of Hashimoto's thyroiditis and Riedel's non-infectious thyroiditis, acute non-suppurative thyroiditis, varies widely in different clinics, but thyroiditis and de Quervain's thyroiditis. -

Iodine Intake and Prevalence of Thyroid Autoimmunity And
European Journal of Endocrinology (2012) 167 387–392 ISSN 0804-4643 CLINICAL STUDY Iodine intake and prevalence of thyroid autoimmunity and autoimmune thyroiditis in children and adolescents aged between 1 and 16 years Emilio Garcı´a-Garcı´a, Marı´a A´ ngeles Va´zquez-Lo´pez, Eduardo Garcı´a-Fuentes1, Firma Isabel Rodrı´guez-Sa´nchez2, Francisco Javier Mun˜oz2, Antonio Bonillo-Perales and Federico Soriguer1 Hospital Torreca´rdenas, Unidad de Pediatrı´a, Paraje Torreca´rdenas, s/n, E-04009 Almerı´a, Spain, 1Hospital Carlos Haya, Unidad de Endocrinologı´a y Nutricio´n, Ma´laga, Spain and 2Hospital Torreca´rdenas, Unidad de Biotecnologı´a, Almerı´a, Spain (Correspondence should be addressed to E Garcı´a-Garcı´a; Email: [email protected]) Abstract Objectives: To determine the status of iodine nutrition in children and adolescents in Almerı´a, Spain. To calculate prevalence of thyroid autoimmunity (TA) and autoimmune thyroiditis (AT) in pediatric ages and to research into associated factors. Methods: Cross-sectional epidemiological study. By a multistage probability sampling 1387 children and adolescents aged between 1 and 16 were selected. Physical examination was carried out including neck palpation. Parents were asked about eating habits as well as about social and demographic aspects. Urinary iodine, free thyroxine, TSH, antiperoxidase and antithyroglobulin antibodies were measured. TA was diagnosed when any antibody was positive and AT when autoimmunity was associated with impaired thyroid function or goitre. Results are shown using percentages (and its 95% confidence interval). To study associated factors we used multiple logistic regression, quantifying the relation with odds ratio (OR), and multiple lineal regression. -

Thyrotoxicosis
THYROTOXICOSIS: A RETROSPECTIVE STUDY OF CASES SEEN AT NUCLEAR MEDICINE UNIT (NEMROCK) Thesis Submitted for the fulfillment of master degree In nuclear medicine By Amira Hodhod Elsayed M.B.B.CH Under Supervision of Professor Dr. Shawky Ibrahim El.Haddad Professor of Radiotherapy and Nuclear Medicine Faculty of medicine –Cairo University Dr. Gehan Ahmed Yuonis Lecturer of Nuclear Medicine Faculty of medicine –Cairo University Faculty of medicine Cairo University 2013 Acknowledgments First, I would like to thank all my professors who allowed me to quote their work. I particularly grateful to professor Dr/ Shawky El.hadad for his encouragement and generosity in dealing with science and Dr/ Gehan Younis, this study would be much poorer without her help. I am grateful to everyone in Nuclear Medicine department, Cairo University. A special thanks to Dr/ Ahmed Sabrey who helped me in the statistical part of the study. I am deeply indebted to my dear husband Dr/ Hisham Aboelnasr, who was encouraging and supportive throughout. This list would not be completed without mentioning the role of my great mother in supporting me. And last but not least, to my family and my friends for patiently persevering with me. Index List of figures……………………………………………….…….…………………I List of tables………………………………………………………………………….III List of abbreviations………………………………………..………………..….V Introduction and aim of the study………………………..…………….…1 Review of literature……………………………………….………..……………5 Material, methods and data collection…………………………….….49 Results………………………………………………………………………………..52 -

Thyroid Dysfunction and the Eye March 19, 2021 Greg a Caldwell
Thyroid Dysfunction and the Eye March 19, 2021 Disclosures- Greg Caldwell, OD, FAAO $ The content of this activity was prepared independently by me - Dr. Caldwell $ Lectured for: Alcon, Allergan, Aerie, BioTissue, Kala, Maculogix, Optovue Thyroid Dysfunction $ Advisory Board: Allergan, Sun, Alcon, Maculogix, Dompe $ Envolve: PA Medical Director, Credential Committee and the Eye $ Healthcare Registries – Chairman of Advisory Council $ I have no direct financial or proprietary interest in any companies, products or services mentioned in this presentation Greg Caldwell OD, FAAO $ The content and format of this course is presented without commercial bias and does not claim Utah Optometric Association superiority of any commercial product or service $ Optometric Education Consultants - Scottsdale, Minneapolis, Florida (Ponte Verda Beach), March 19, 2021 Mackinac Island, MI, Nashville, and Quebec City - Owner 1 2 Thyroid $Thyroid is an endocrine gland $Two types of glands Thyroid Disease ¬ Endocrine and ¬ Exocrine $Endocrine system is a control system of ductless endocrine glands that Thyroid Eye Disease secrete hormones (chemical messenger) that circulate within the body via the bloodstream or lymph system to affect distant organs ¬ Hypothalamus ¬ Pancreas ¬ Pituitary gland ¬ Adrenal glands ¬ Thyroid ¬ Gonads (testes and ovaries) ¬ Parathyroid glands ¬ Pineal gland 3 4 Thyroid Thyroid $Exocrine glands contain ducts. Ducts are tubes leading from a gland to its target organ $Largest endocrine gland in the body ¬ Digestive glands have ducts for releasing the digestive enzymes $Butterfly shaped ¬ Salivary glands, sweat glands and glands within the gastrointestinal tract $Two lobes located on either side of the trachea in the lower portion of $Pancreas is both endocrine and exocrine the neck ¬ Exocrine (ducted gland) secreting digestive enzymes into the small intestine. -

Subacute Thyroiditis Christa M
ENDOCRINECONSULT Subacute Thyroiditis Christa M. Blose, MPAS, PA-C, Holly Jodon, MPAS, PA-C erry, a 48-year-old white man, is referred to endocri- TABLE Jnology for abnormal results Lab Results for Case Patient of thyroid tests performed four Time after symptom onset weeks ago (see table for values). Two months ago, Jerry developed 1 mo 2 mo 4 mo 6 mo an upper respiratory infection TSH (0.40-4.50 mlU/mL) 0.03 0.14 8.23 3.54 (URI) with fever, odynophagia, and anterior neck discomfort. Free T4 (0.8-1.8 ng/dL) 2.58 1.74 0.72 1.66 His symptoms resolved after two weeks; however, he has since de- Free T3 (2.3-4.2 pg/mL) 4.12 1.7 3.0 veloped fatigue and nervousness. The remaining review of sys- TPO antibody (< 20) 11 tems is unremarkable. Medical ESR (0-22 mm/h) 55 history is negative. Jerry denies any factors that can affect thyroid Abbreviations: ESR, erythrocyte sedimentation rate; T3, triiodothyronine; T4, thyroxine; function: He does not take thyroid TPO, thyroid peroxidase antibody. medication, OTC thyroid supple- ments, amiodarone, lithium, or TSH, with normal free thyroxine except for a small, firm thyroid interferon-α, does not have high (T4) and free triiodothyronine gland without the tenderness iodine intake, and has not un- (T3) levels. His thyroid peroxidase elicited previously. Labwork re- dergone head/neck irradiation. antibody (Anti-TPO) is negative. veals an elevated TSH with low There is no personal or family Radioactive iodine uptake (RAIU) free T4 and free T3. -

Subacute Thyroiditis: Diagnostic Difficulties and Simple Treatment
SUBACUTE THYROIDITIS: DIAGNOSTIC DIFFICULTIES AND SIMPLE TREATMENT Joel I. Hamburger Northland Thyroid Laboratory, Southfield, Michigan Subacute thyroiditis (SAT) constitutes 0.8% produce the systemic manifestations of hyperthyroid of referrals to Northland Thyroid Laboratory ism, usually mild. and is one tenth as common as hyperthyroidism. The laboratory abnormalities are readily under The peak age is 30—SOyears, and women pre standable in terms of the underlying pathophysiology. dominated by a factor of 4.5. Two thirds of the As a consequence of the diffuse inflammation, the patients presented in typical fashion with a thyroidal uptake of radioactive iodine (RAI) is im painful tender goiter, but for one third the paired (1—9). The discharge of thyroid hormone presentation was atypical in that there was no elevates serum thyroxine values (ST4) (1—9). The pain, the principal complaint in most cases erythrocyte sedimentation rate (ESR) is elevated being painless goiter, thyroid nodule, or fea as a nonspecific response to inflammation (1—9), and tures of hyperthyroidism. Elevated erythrocyte occasionally there is an increase in the white blood sedimentation rates were found in all typical cell count (WBC) as well (3,6—9). patients and in 11 of 14 atypical patients. As the disease progresses the local and systemic Serum thyroxine iodide values were elevated in features decline until full recovery is realized, usually two thirds of the patients, typical and atypi within 2—4months. In some instances there is a cal. The radioactive iodine uptake was sub temporary hypothyroid phase (2,3) which rarely nornwl for all and responded subnormally to may prove permanent (10) . -
A Rare Case of Subacute Thyroiditis Simultaneously Complicated by Graves’ Disease: a Case Report and Review of the Literature
Journal of Endocrinology and Thyroid Research ISSN: 2573-2188 Case Report J Endocrinol Thyroid Res Volume 2 Issue 4 August 2017 DOI: 10.19080/JETR.2017.02.555595 Copyright © All rights are reserved by Toshihiko Yanase A Rare Case of Subacute Thyroiditis Simultaneously Complicated by Graves’ Disease: A Case Report and Review of the Literature Ayako Fukushima, Makito Tanabe, Yuichi Terawaki, Takashi Fukuda, Takashi Nomiyama, and Toshihiko Yanase* Department of Endocrinology and Diabetes Mellitus, Fukuoka University, Japan Submission: July 27, 2017; Published: August 28, 2017 *Corresponding author: Toshihiko Yanase, MD, Department of Endocrinology and Diabetes Mellitus, School of Medicine, Fukuoka University, 7-45-1 Nanakuma, Jonan-ku, Fukuoka 814-0180, Japan, Tel: +81-92-801-1011; Fax: +81-92-865-5163; Email: Abstract A 46-year-old female presented with neck pain and thyrotoxicosis. Further examination revealed that she had both subacute thyroiditis (SAT) and Graves’ disease (GD). These diagnoses were made based on increased thyroid hormone levels, high TSH-R antibody titers, echographic normalized by oral administration of prednisolone. Interestingly, she possessed characteristic HLA typing associated with susceptibility to both SATfindings and ofGD. the A thyroidreview andof four concomitant other cases inflammatory showing simultaneous findings. Her onset thyrotoxicosis, of SAT and inflammatory GD in the literature findings revealed and TSH-R a similar antibodies clinical were course gradually and comparable changes in TRAb in all cases. -

Painless Thyroiditis Associated to Thyroid Carcinoma
case report Painless thyroiditis associated to thyroid carcinoma: role of initial ultrasonography evaluation Raisa Bressan Valentini1, Bruno Mussoi de Macedo1, Rogério Friedrich Izquierdo2, Erika Laurini Souza Meyer1 1 Unidade de Tireoide, Serviço de ABSTRACT Endocrinologia, Irmandade da Santa Casa de Misericórdia de Porto Even though it is a rare event, most associations of thyroid carcinoma with subacute thyroiditis de- Alegre, Universidade Federal de scribed in the literature are related to its granulomatous form (Quervain’s thyroiditis). We present a Ciências da Saúde de Porto Alegre patient with subacute lymphocytic thyroiditis (painless thyroiditis) and papillary thyroid cancer that (UFCSPA), Porto Alegre, RS, Brasil was first suspected in an initial ultrasound evaluation. A 30-year old female patient who was referred 2 Serviço de Radiologia, Irmandade to the emergency room due to hyperthyroidism symptoms was diagnosed with painless thyroiditis da Santa Casa de Misericórdia established by physical examination and laboratory findings. With the presence of a palpable painless de Porto Alegre, UFCSPA, Porto Alegre, RS, Brasil. thyroid nodule an ultrasound was prescribed and the images revealed a suspicious thyroid nodule, microcalcification focus in the heterogeneous thyroid parenquima and cervical lymphadenopathy. Correspondence to: Fine needle aspiration biopsy was taken from this nodule; cytology was assessed for compatibility Erika Laurini Souza Meyer Serviço de Endocrinologia with papillary thyroid carcinoma. Postsurgical pathology evaluation showed a multicentric papillary Irmandade da Santa Casa de carcinoma and lymphocytic infiltration. Subacute thyroiditis, regardless of type, may produce tran- Misericórdia de Porto alegre sitory ultrasound changes that obscure the coexistence of papillary carcinoma. Due to this, initial Professor Annes Dias, 295 90020-090 – Porto Alegre, RS, Brasil thyroid ultrasound evaluation should be delayed until clinical recovery. -

ATA/AACE Guidelines
ATA/AACE Guidelines CLINICAL PRACTICE GUIDELINES FOR HYPOTHYROIDISM IN ADULTS: COSPONSORED BY THE AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AND THE AMERICAN THYROID ASSOCIATION Jeffrey R. Garber, MD, FACP, FACE1,2*; Rhoda H. Cobin, MD, FACP, MACE3; Hossein Gharib, MD, MACP, MACE4; James V. Hennessey, MD, FACP2; Irwin Klein, MD, FACP5; Jeffrey I. Mechanick, MD, FACP, FACE, FACN6; Rachel Pessah-Pollack, MD6,7; Peter A. Singer, MD, FACE8; Kenneth A. Woeber, MD, FRCPE9 for the American Association of Clinical Endocrinologists and American Thyroid Association Taskforce on Hypothyroidism in Adults American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice are systematically developed statements to assist health-care professionals in medical decision making for specific clinical conditions. Most of the content herein is based on literature reviews. In areas of uncertainty, professional judgment was applied. These guidelines are a working document that reflects the state of the field at the time of publication. Because rapid changes in this area are expected, periodic revisions are inevitable. We encourage medical professionals to use this information in conjunction with their best clinical judgment. The presented recommendations may not be appropriate in all situations. Any decision by practitioners to apply these guidelines must be made in light of local resources and individual patient circumstances. 988 989 CLINICAL PRACTICE GUIDELINES FOR HYPOTHYROIDISM IN ADULTS: COSPONSORED BY THE AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AND THE AMERICAN THYROID ASSOCIATION Jeffrey R. Garber, MD, FACP, FACE1,2*; Rhoda H. Cobin, MD, FACP, MACE3; Hossein Gharib, MD, MACP, MACE4; James V. Hennessey, MD, FACP2; Irwin Klein, MD, FACP5; Jeffrey I. Mechanick, MD, FACP, FACE, FACN6; Rachel Pessah-Pollack, MD6,7; Peter A.