Morphometric Study of the Humerus Segments in Indian Population
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Considered a Bone of Both Shoulder Girdle and Shoulder Joint. the Shoulder Girdle Is Comprised of the Clavicle and the Scapula
Considered a bone of both shoulder girdle and shoulder joint. The shoulder girdle is comprised of the clavicle and the scapula. The shoulder joint consists of the scapula and the humerus. The primary function of the shoulder girdle is to position itself to accommodate movements of the shoulder joint. 1 Superior angle—top point Inferior angle—bottom point Vertebral border—side closest to vertebral column Axillary border—side closest to arm Subscapular fossa—anterior fossa Glenoid fossa, glenoid labrum, glenoid cavity --The glenoid fossa is the shallow cavity where the humeral head goes. The glenoid labrum is the cartilage that goes around the glenoid fossa. So the glenoid fossa and glenoid labrum together comprise the glenoid cavity. Supraspinous fossa—posterior, fossa above the spine Spine of the scapula—the back projection Infraspinous fossa—posterior depression/fossa below spine Coracoid process—anterior projection head Acromion process—posterior projection head above spine 2 Scapulothoracic “joint” = NOT a true joint; there are no ligaments or articular capsule. The scapula just rests on the muscle over top the rib cage, which allows for passive movements. Sternoclavicular joint=where the clavicle (collarbone) and the sternum (breastbone) articulate; movement is slight in all directions and of a gliding, rotational type Acromioclavicular joint = where the clavicle and scapula (acromion process) articulate; AKA: AC Joint; movement is a slight gliding when elevation and depression take place. Glenohumeral joint = the shoulder joint 3 4 All 3 true joints: Sternoclavicular, AC and glenohumeral (GH) all work together to move arm in all directions. The GH allows the arm to go out to the side and be abducted, then the AC and Sternoclavicular joints kick in to allow the arm to go above shoulder level by allowing the shoulderblade to move up to increase the range of motion (ROM). -

The Appendicular Skeleton Appendicular Skeleton
THE SKELETAL SYSTEM: THE APPENDICULAR SKELETON APPENDICULAR SKELETON The primary function is movement It includes bones of the upper and lower limbs Girdles attach the limbs to the axial skeleton SKELETON OF THE UPPER LIMB Each upper limb has 32 bones Two separate regions 1. The pectoral (shoulder) girdle (2 bones) 2. The free part (30 bones) THE PECTORAL (OR SHOULDER) GIRDLE UPPER LIMB The pectoral girdle consists of two bones, the scapula and the clavicle The free part has 30 bones 1 humerus (arm) 1 ulna (forearm) 1 radius (forearm) 8 carpals (wrist) 19 metacarpal and phalanges (hand) PECTORAL GIRDLE - CLAVICLE The clavicle is “S” shaped The medial end articulates with the manubrium of the sternum forming the sternoclavicular joint The lateral end articulates with the acromion forming the acromioclavicular joint THE CLAVICLE PECTORAL GIRDLE - CLAVICLE The clavicle is convex in shape anteriorly near the sternal junction The clavicle is concave anteriorly on its lateral edge near the acromion CLINICAL CONNECTION - FRACTURED CLAVICLE A fall on an outstretched arm (F.O.O.S.H.) injury can lead to a fractured clavicle The clavicle is weakest at the junction of the two curves Forces are generated through the upper limb to the trunk during a fall Therefore, most breaks occur approximately in the middle of the clavicle PECTORAL GIRDLE - SCAPULA Also called the shoulder blade Triangular in shape Most notable features include the spine, acromion, coracoid process and the glenoid cavity FEATURES ON THE SCAPULA Spine - -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Parts of the Body 1) Head – Caput, Capitus 2) Skull- Cranium Cephalic- Toward the Skull Caudal- Toward the Tail Rostral- Toward the Nose 3) Collum (Pl
BIO 3330 Advanced Human Cadaver Anatomy Instructor: Dr. Jeff Simpson Department of Biology Metropolitan State College of Denver 1 PARTS OF THE BODY 1) HEAD – CAPUT, CAPITUS 2) SKULL- CRANIUM CEPHALIC- TOWARD THE SKULL CAUDAL- TOWARD THE TAIL ROSTRAL- TOWARD THE NOSE 3) COLLUM (PL. COLLI), CERVIX 4) TRUNK- THORAX, CHEST 5) ABDOMEN- AREA BETWEEN THE DIAPHRAGM AND THE HIP BONES 6) PELVIS- AREA BETWEEN OS COXAS EXTREMITIES -UPPER 1) SHOULDER GIRDLE - SCAPULA, CLAVICLE 2) BRACHIUM - ARM 3) ANTEBRACHIUM -FOREARM 4) CUBITAL FOSSA 6) METACARPALS 7) PHALANGES 2 Lower Extremities Pelvis Os Coxae (2) Inominant Bones Sacrum Coccyx Terms of Position and Direction Anatomical Position Body Erect, head, eyes and toes facing forward. Limbs at side, palms facing forward Anterior-ventral Posterior-dorsal Superficial Deep Internal/external Vertical & horizontal- refer to the body in the standing position Lateral/ medial Superior/inferior Ipsilateral Contralateral Planes of the Body Median-cuts the body into left and right halves Sagittal- parallel to median Frontal (Coronal)- divides the body into front and back halves 3 Horizontal(transverse)- cuts the body into upper and lower portions Positions of the Body Proximal Distal Limbs Radial Ulnar Tibial Fibular Foot Dorsum Plantar Hallicus HAND Dorsum- back of hand Palmar (volar)- palm side Pollicus Index finger Middle finger Ring finger Pinky finger TERMS OF MOVEMENT 1) FLEXION: DECREASE ANGLE BETWEEN TWO BONES OF A JOINT 2) EXTENSION: INCREASE ANGLE BETWEEN TWO BONES OF A JOINT 3) ADDUCTION: TOWARDS MIDLINE -

Shoulder Shoulder
SHOULDER SHOULDER ⦿ Connects arm to thorax ⦿ 3 joints ◼ Glenohumeral joint ◼ Acromioclavicular joint ◼ Sternoclavicular joint ⦿ https://www.youtube.com/watch?v=rRIz6oO A0Vs ⦿ Functional Areas ◼ scapulothoracic ◼ scapulohumeral SHOULDER MOVEMENTS ⦿ Global Shoulder ⦿ Arm (Shoulder Movement Joint) ◼ Elevation ◼ Flexion ◼ Depression ◼ Extension ◼ Abduction ◼ Abduction ◼ Adduction ◼ Adduction ◼ Medial Rotation ◼ Medial Rotation ◼ Lateral Rotation ◼ Lateral Rotation SHOULDER MOVEMENTS ⦿ Movement of shoulder can affect spine and rib cage ◼ Flexion of arm Extension of spine ◼ Extension of arm Flexion of spine ◼ Adduction of arm Ipsilateral sidebending of spine ◼ Abduction of arm Contralateral sidebending of spine ◼ Medial rotation of arm Rotation of spine ◼ Lateral rotation of arm Rotation of spine SHOULDER GIRDLE ⦿ Scapulae ⦿ Clavicles ⦿ Sternum ⦿ Provides mobile base for movement of arms CLAVICLE ⦿ Collarbone ⦿ Elongated S shaped bone ⦿ Articulates with Sternum through Manubrium ⦿ Articulates with Scapula through Acromion STERNOCLAVICULAR JOINT STERNOCLAVICULAR JOINT ⦿ Saddle Joint ◼ Between Manubrium and Clavicle ⦿ Movement ◼ Flexion - move forward ◼ Extension - move backward ◼ Elevation - move upward ◼ Depression - move downward ◼ Rotation ⦿ Usually movement happens with scapula Scapula Scapula ● Flat triangular bone ● 3 borders ○ Superior, Medial, Lateral ● 3 angles ○ Superior, Inferior, Lateral ● Processes and Spine ○ Acromion Process, Coracoid Process, Spine of Scapula ● Fossa ○ Supraspinous, Infraspinous, Subscapularis, Glenoid SCAPULA -

Skeletal System -Appendicular System
Skeletal System -Appendicular System Chapter 8 Part B Skeleton - Divisions Total number of bones: 206 Divided into two major subdivisions: Axial system….blue Appendicular system….tan Axial system: Composed of bones that form the axis of the body. 80 bones. Appendicular system: Composed of bones that form The limbs. The bones that attach the limbs to the axial. 126 bones. Practice…Practice…Practice…Practice…Practice!! Appendicular Skeleton Appendicular system: Pectoral girdle 4 bones Upper extremity 60 bones Pelvic girdle 2 bones Lower extremity 60 bones 126 bones Appendicular Skeleton Appendicular system: Pectoral girdle 4 bones Upper extremity 60 bones Pelvic girdle 2 bones Lower extremity 60 bones 126 bones Upper Extremity/Limb Upper limbs/extremities are composed of 60 bones…30 bones in each limb: Upperarm – Humerus Forearm – Radius and Ulna Wrist – Carpals Hand – Metacarpals in palm – Phalanges in fingers and thumb Upper Extremity/Limb - Humerus Body/Shaft Humerus: long bone. Has 3 regions: Proximal end articulates with glenoid cavity of scapula. Distal end articulates with radius and ulna. Body/Shaft: diaphysis between proximal and distal ends. Has rough surface – deltoid tuberosity…for deltoid muscle attachment. Upper Extremity/Limb - Humerus Body/Shaft Humerus - Proximal end: Head: rounded projection fits into glenoid cavity of scapula. Greater and lesser tubercles: projections next to the head for muscle attachment. Intertubercular sulcus: groove between the tubercles accommodates tendon of an arm muscle. Upper Extremity/Limb - Humerus Body/Shaft Humerus - Distal end: Anterior surface: Capitulum: small, rounded knob articulates with proximal end of radius of forearm. Trochlea: spool-shaped structure articulates with proximal end of ulna of forearm. -

Arm and Cubital Fossa
Two Minute History M1 - Anatomy Dissection: • 300 B.C Arm and Cubital Alexandrian Egypt: King Ptolemy I, its ok Fossa to dissect cadavers of executed, mummies etc… •Herophilus “Father of Anatomy” accused by a rival of DG Simpson, Ph.D. dissecting 600 criminals…..live criminals VCU Department of Anatomy •1300 AD Europe Pope Boniface VIII edict to stop dissection to reduce the flow of bodies “parted out and boiled” from the crusades. Unclear if this is broad ban or very narrow. 1 2 Dissection: Dissection: •1540 parliament passes “The United Company of Barbers and •1700’s with the expansion of medical Surgeons, dissect 4-6 executed schools cadavers are used as tuition criminals/yr (not enough even then) •Competition is very high and medical •1600’s Britain. The executed are schools actively advertise that training includes dissections etc.. dissected in public as punishment • 1628 William Harvey •1828 London had 10 full time (cardiovascular fame). Autopsy & 200 part time body snatchers (“seasonal work” at 312 bodies/yr) of live and dead…. Medicine expands and shortages develop •Inventions to foil grave robbers Harvey dissects father and sister •1828 Robert Knox….and the rest • 1740’s Lots of private medical is amazing history. schools competing for students, William Hogarth The Reward of Cruelty 3 4 market forces develop 1750-1751 Dissection: •Burke was hanged: 25,000 watched. Hare was granted immunity as crowd called “Burke Hare” •1828, knock on the •Burke dissected: 30,000 came to see the open lab door, Knox’s assistant purchases a cadaver -
Bones of Upper Limb
BONES OF THE UPPER LIMB Dr. Jamila El-Medany OBJECTIVES At the end of the lecture, students should be able to: List the different bones of the UL. List the characteristic features of each bone. Differentiate between the bones of the right and left sides. List the articulations between the different bones. The Bones of UL are: Pectoral Girdle. Arm : Humerus. Forearm : Radius & Ulna. Wrist : Carpal bones Hand: Metacarpals & Phalanges Pectoral Girdle Formed of Two Bones: Clavicle (anteriorly) and Scapula (posteriorly). It is very light and allows the upper limb to have exceptionally free movement. Clavicle It is a doubly curved long bone lying horizontally across the root of the neck It is subcutaneous throughout its length. Functions: 1. It serves as a rigid support from which the scapula and free upper limb are suspended & keep them away from the trunk so that the arm has maximum freedom of movement. 2. Transmits forces from the upper limb to the axial skeleton. 3. Provides attachment for muscles. 4. It forms a boundary of the Cervicoaxillary canal for protection of the neurovascular bundle of the UL. Clavicle It is a long bone with no medullary cavity. It has the appearance of an elongated letter Capital (S) lying on one side. It has Two Ends: Medial (Sternal) : enlarged & triangular. Lateral (Acromial) : flattened. Body (shaft): Its medial 2/3 is convex forward. Its lateral 1/3 is concave forward. Surfaces: Superior : smooth as it lies just deep to the skin. Inferior : rough because strong ligaments bind it to the 1st rib. Articulations of Clavicle Medially with the manubrium at the Sternoclavicular joint . -

BO6 106 Rzepkowki
106: Shoulder & Elbow Joint Replacements – New Advancements in Rehab Terry Rzepkowski, DPT, MS, BS To comply with professional boards/associations standards: • I declare that I (or my family) do not have a financial relationship in any amount, occurring in the last 12 months with a commercial interest whose products or services are discussed in my presentation. Additionally, all planners involved do not have any financial relationship. •Requirements for successful completion are attendance for the full session along with a completed session evaluation. •PESI and all current accreditation statuses does not imply endorsement of any commercial products displayed in conjunction with this activity. 106: Shoulder & Elbow Joint Replacements – New Advancements in Rehab Terry Rzepkowski, DPT, MS, BS Financial: Terry Rzepkowski is an Assistant Professor for Nova Southeastern University Tampa; and an Assistant Professor for South University Tampa. He receives a speaking honorarium from PESI, Inc. Non‐financial: Terry Rzepkowski is a member of the American Physical Therapy Association (APTA). UE joint replacements and post‐op management Dr. Terry Rzepkowski, DPT Associate Professor [email protected] 1 About the instructor Dr. Terry L Rzepkowski, DPT, MS, BS Dr. Terry L Rzepkowski, DPT, MS, BS, is a Doctor of Physical Therapy with specialization in Orthopedic Physical Therapy. Throughout his 38‐year career, he has specialized in Orthopedics, specifically: Musculoskeletal out‐patient rehab as an independent private practitioner, Total Joint Replacement Surgery, Sports Medicine, and Orthopedic Homecare. This extensive background allows him to relate his knowledge of the complex rehab patient from prevention strategies including rehabilitative exercises, lifestyle and activity modifications through all phases of post‐op rehabilitation. -

Variability of Elbow Radiography in the Injured Child: a Potential Diagnostic Dilemma
The Journal of Emergency Medicine, Vol. 57, No. 5, pp. 653–661, 2019 Ó 2019 Published by Elsevier Inc. 0736-4679/$ - see front matter https://doi.org/10.1016/j.jemermed.2019.08.036 Selected Topics: Emergency Radiology VARIABILITY OF ELBOW RADIOGRAPHY IN THE INJURED CHILD: A POTENTIAL DIAGNOSTIC DILEMMA Daniel S. Brereton, DO,*† Kevin Kwam, MS,‡ and John A. Schlechter, DO*† *Department of Orthopedics, Children’s Hospital Orange County, Adult and Pediatric Orthopedic Specialists, Orange, California, †Department of Orthopedics, Riverside University Health Systems, Moreno Valley, California, and ‡College of Osteopathic Medicine of the Pacific, Western University of Health Sciences, Pomona, California Reprint Address: Daniel S. Brereton, DO, Department of Orthopedics, Riverside University Health Systems, 26520 Cactus Avenue, Moreno Valley, CA 92555 , Abstract—Background: Radiographic imaging is essen- when assessing the injured child’s elbow and determining tial in assessing the severity and treatment of injuries. How- management. Ó 2019 Published by Elsevier Inc. ever, when a radiographic series is of poor quality, its diagnostic utility is limited, especially in cases involving pe- , Keywords—pediatric; orthopedic; elbow; fracture; diatric elbow injuries. Objectives: This study aims to inves- x-ray tigate the variability of elbow radiographs in the injured child, review parameters used to assess diagnostic quality, and introduce the lateral distal humeral metaphyseal- INTRODUCTION diaphyseal (LDHMD) ratio as a potential measurement of the quality of a lateral elbow radiograph. Methods: A retro- The quality of images such as electrocardiographic trac- spective review was performed of elbow radiographs of chil- ings, radiographs, magnetic resonance imaging, and the dren who presented to our hospital. -
Elbow Instability the Elbow Is Both a Hinge Joint and a Ball and Socket Joint Between the Humerus in the Upper Arm and the Radius and Ulna in the Forearm
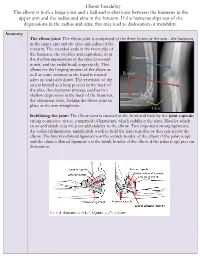
Elbow Instability The elbow is both a hinge joint and a ball and socket joint between the humerus in the upper arm and the radius and ulna in the forearm. If the humerus slips out of the depressions in the radius and ulna, this may lead to dislocation or instability. Anatomy The elbow joint: The elbow joint is comprised of the three bones of the arm - the humerus in the upper arm and the ulna and radius of the forearm. The rounded ends in the front side of the humerus, the trochlea and capitulum, sit in the shallow depressions in the ulna (coronoid Humerus notch) and the radial head, respectively. This allows for the hinging motion of the elbow as well as some rotation as the hand is rotated Radius palm up and palm down. The extension of the arm is limited as a long process in the back of the ulna, the olecranon process, catches in a shallow depression in the back of the humerus, the olecranon fossa, locking the elbow joint in place as the arm straightens. Ulna Stabilizing the joint: The elbow joint is encased in the front and back by the joint capsule, strong connective tissue, comprised of ligaments, which stabilizes the joint. Muscles which cross and attach near the joint add stability to the elbow. Two important strong ligaments, the collateral ligaments, significantly work to hold the joint together as they run across the elbow. The lateral collateral ligament (on the outside border of the elbow if the palm is up) and the ulnar collateral ligament (on the inside border of the elbow if the palm is up) prevent dislocation. -

Anatomical Features of Some Bones of the Forelimbs of Lions (Panthera Leo)
Int. J. Morphol., 39(2):378-385, 2021. Anatomical Features of Some Bones of the Forelimbs of Lions (Panthera leo) Características Anatómicas de Algunos Huesos de los Miembros Torácicos de Leones (Panthera leo) Md. Shahriar Hasan Sohel1; Kh. Nurul Islam2 & Mohammad Lutfur Rahman2 SOHEL, M. S. H.; ISLAM, K. N. & RAHMAN, M. L. Anatomical features of some bones of the forelimbs of lions (Panthera leo). Int. J. Morphol., 39(2):378-385, 2021. SUMMARY: We studied the bones of forelimb of four adult lions (Panthera leo) of both sexes to record the gross anatomical and morphometrical features of the scapula, humerus, radius and ulna. We observed some unique anatomical features that will be helpful for radiographic interpretation and forensic investigations. The lateral surface of scapula was unequally divided into supraspinous (fossa supraspinata) and infraspinous fossa (fossa infraspinata) by a well developed spine (spina scapulae). The acromion process was subdivided into suprahamate process (processus suprahamatus)and hamate process (processus hamatus); the later one was over hanged the glenoid cavity (cavitas glenoidalis), but the supraglenoid tubercle (tuberculum supraglenoidalis) was absent. The shaft (diaphysis) of humerus was compressed craniocaudally in proximal part, rounded to oval in middle part and compressed mediolaterally in distal part. A long, narrow supracondyloid foramen was found at distal limb just above the medial epicondyle (epicondylus medialis) which didn’t connect the radial fossa (fossa radialis) with the olecranon fossa (fossa olecrani). The radius and ulna were twin bones where radius was articulated craniolateral to the ulna proximally and craniomedial to the ulna distally. However, the ulna was the longest bone in the forelimb of lion.