Empowering Communities to Collectively
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Report on Orchid Project's Knowledge Sharing Workshops in Hargeisa
Knowledge Sharing Workshops on FGM/C Policy and programme implementation December 2017 Hargeisa, Somaliland i Contents Summary 1 1 Introduction 2 Aim and intended learning outcomes 2 2 Workshop process 2 Stimulus material 3 FGM/C in Somaliland: knowledge, attitudes and perceptions 4 (SOFHA / ORCHID) Changes in FGM/C in Somaliland (Population Council) 4 UNICEF Six Elements of Abandonment 5 3 Open dialogue sessions 5 Medicalisation 5 Policy 6 Behavioural / social change 6 Child rights 7 Further research 7 Role of NGOs and CBOs 7 4 Action planning 8 5 Review 9 6 Looking forward 11 7 Conclusions 12 Appendices A Workshop participants 13 B Workshop timetable 14 C Briefing - SOFHA research 17 D Briefing – Population Council research 18 E Summary UNICEF Six Elements of Abandonment 19 F Action participants would like others to take 20 G Action plans from policy makers and programme implementers 21 H Abbreviations 30 i Summary In 2016/17, Population Council (PC) sponsored research into FGM/C in Somaliland, supported by the Norwegian Agency for Development Cooperation (Norad), through the project FGM/C Research Capacity Building which seeks to strengthen the capacity of Norad partners to generate and use evidence for decision making in relation to FGM/C. Knowledge sharing workshops took place in December 2017, involving over 40 policy makers and programme implementers working to end FGM/C in Somaliland. The aim of the workshops was to pilot a new approach to disseminating research findings to increase the impact of research findings on decision -

Somaliland Assistance Bulletin
Somaliland Assistance Bulletin 1 – 30 November 2005 HUMANITARIAN SITUATION Security & Access The overall security situation in Somaliland remained stable. A verdict was issued on the trail case of the 10 arrested suspects of the killings of four humanitarian workers occurring in 2003 and 2004. The case originally started in March 2005. According to the regional court in Hargeisa, 8 men were found guilty of "terrorism" and were sentenced to death. Following the killing of the 4 expatriate humanitarian workers, the UN in collaboration with the national authorities established a Special Protection Unit (SPU) initially to provide protection for humanitarian workers of UN & international NGOs, subsequently extended to the rest of the community. Since then no further incidents were reported. A deadly mine accident occurred in Burao on 16 November 2005 where a vehicle diverted from the main road towards a roadside short cut. Three out of a total of seven passengers were reported dead, including one UN staff member. Somaliland Mine Action Center (SMAC), supported by UNDP, coordinates mine action activities, since late 1999, an approximate area of around 115 million square meters has been cleared. Food Security/Livelihoods Aerial Photograph of Burao settlements, source UN Habitat. Deyr rain started on time, whereby most areas received Ministry of Health & Labour (MOH&L), the Somali Red normal to above normal rains except for parts of Crescent Society, Save the Children Fund, Candlelight southern Awdal region. Rainfall distribution and intensity and Havoyoco. Sources of income among Burao were good and allowed for further replenishment of water settlements were labeled more irregular and unreliable. -
2019 Programmatic Overview 1
IOM SOMALIA 2019 PROGRAMMATIC OVERVIEW 1 2019 PROGRAMMATIC OVERVIEW SOMALIA IOM SOMALIA 2019 PROGRAMMATIC OVERVIEW 2 In Memorium IOM stands in solidarity with the people of Somalia who have suffered numerous deadly attacks on civilians during the course of 2019. We are deeply saddened by the terrible loss of one of our colleagues, Abdifatah Mohamed Abdow, who dedicated his life and work to Somalia. IOM extends its deepest condolences to the families and loved ones of all those who lost their lives in Kismayo in July 2019. IOM SOMALIA 2019 PROGRAMMATIC OVERVIEW 3 Cover photo: A family benefited from IOM’s Baidoa relocation project © IOM Somalia 2019 IOM staff organizing the relocation of IDP families in Baidoa © IOM Somalia 2019 DISCLAIMER: The names and boundaries shown do not imply official endorsement nor acceptance by IOM. They are meant for illustrative purposes. EDITOR: Erin Bowser, Jan Van’t Land, Yuko Tomita LAYOUT DESIGN: Claudia Barrios Rosel IOM SOMALIA 2019 PROGRAMMATIC OVERVIEW 4 IOM SOMALIA 2019 OVERVIEW CONTENTS IOM OVERVIEW 2019 HIGHLIGHTS HUMANITARIAN RESPONSE Camp Coordination and Camp Management (CCCM) Displacement Tracking Matrix (DTM) Water, Sanitation and Hygiene (WASH) Health Shelter and Non-Food Items (S-NFI) STABILIZATION, RECOVERY AND DURABLE SOLUTIONS Recovery and Durable Solutions (RDS) Somalia Stabilization Initiative (SSI) Disengagement, Disassociation, Reintegration and Reconciliation (DDRR) MIGRATION GOVERNANCE & DEVELOPMENT Immigration and Border Management (IBM) Labour Mobility and Human Development (LHD) Migrant Protection and Assistance (MPA) IOM SOMALIA 2019 PROGRAMMATIC OVERVIEW 5 1/ IOM OVERVIEW Established in 2006, IOM Somalia has set a strong record on the delivery of frontline services to crisis-affected populations, while steadily developing models and partnerships for longer term recovery and migration governance. -

2010 by Bram Piot
Birding in and around Hargeisa, Somaliland, December 2010 by Bram Piot From December 10 to 17 I stayed in Hargeisa for my work with PSI, a public health NGO that recently established an office in Somaliland. For Saturday 11th I had organised a day out birding with Abdi Jama from NatureSomaliland, who had also guided three groups earlier this year – the first commercial birding tours to visit Somaliland. Our day trip took us east of Hargeisa through thorn bush, acacia woodland, rocky plains and wadis all the way to the vast Tuuyo plain (see map 1). Several very productive stops were made along the first 20 kilometers of the trip; Tuuyo plain was explored in the early afternoon so the birds there was not very active – e.g. none of the larks were singing, but this may also be because it is non-breeding season for most species. Our late lunch stop to the north of Shaarub village proved to be a good spot, but a long drive back to Hargeisa prevented us from fully exploring this area or the plains that we crossed further to the north (Qoryale for example looked pretty good). On hindsight, it probably would have been more efficient (less driving, more birding!) to drive back the way we came, rather than doing the long loop towards the Hargeisa-Berbera tarmac road. Total trip distance was about 280 km. Nearly 100 species were recorded during this day trip, with personal highlights including 3 species of Bustard (Little Brown, Heuglin’s, Buff-crested), several confiding Somali and Double- banded Coursers, a Greyish Eagle-Owl, 6 lark species including the endemic Lesser Hoopoe and Sharpe’s Larks, an Arabian Warbler, several Golden-breasted Starlings, a Three-streaked Tchagra, Rosy-patched Bush-shrikes, Somali Wheatears, Somali Bee-eaters, a group of Scaly Chatterers, etc. -

UNFPA Final 23.06.2016
EVALUATION REPORT SOMALIA INDEPENDENT COUNTRY PROGRAMME EVALUATION 2011-2015 This report was prepared by Vision Quest Consultants. Disclaimer: This evaluation report was prepared for United Nations Population Fund Somalia Country Office by Vision Quest Consultants. The analysis and recommendations of this report do not necessarily reflect the views of UNFPA, its Executive Board or the United Nations Member States. ACKNOWLEDGEMENTS Vision Quest Consultants (VQC) extends its sincere field teams, led by Heads of Sub-Offices for gratitude to the UNFPA Somalia country office for Somaliland, Puntland and Mogadishu for their the opportunity to undertake this evaluation valuable support and guidance during planning and exercise. VQC is grateful for the support that the execution of the evaluation. We also extend special country office staff gave to the evaluation team at thanks to Simon-Pierre Tegang the Regional M&E every stage of the process. In particular, we Adviser- Arab States Regional Office and Yukari appreciate the support of Grace Kyeyune, the Horii, Programme Analyst (Monitoring and Deputy Representative, the entire management Evaluation) for the UNFPA Arab States Region, for team, and Ezekiel Kutto, the M&E Analyst for the their professional guidance during the Country country office for his technical support and Programme Evaluation (CPE) design and for their guidance during the evaluation period. We also valuable comments on the evaluation findings. recognise the efforts of Stella Kimani, UNFPA’s M&E intern who helped coordinate -

Provision of Surgical Care for Children Across Somaliland: Challenges and Policy Guidance
World J Surg https://doi.org/10.1007/s00268-019-05079-8 ORIGINAL SCIENTIFIC REPORT Provision of Surgical Care for Children Across Somaliland: Challenges and Policy Guidance 1 1,2 3 3 Tessa L. Concepcion • Emily R. Smith • Mubarak Mohamed • Shugri Dahir • 3 4 5 1 Edna Adan Ismail • Andrew J. M. Leather • Dan Poenaru • Henry E. Rice on behalf of the Global Initiative for Children’s Surgery Ó Socie´te´ Internationale de Chirurgie 2019 Abstract Background Existing data suggest a large burden of surgical conditions in low- and middle-income countries (LMICs). However, surgical care for children in LMICs remains poorly understood. Our goal was to define the hospital infrastructure, workforce, and delivery of surgical care for children across Somaliland and provide policy guidance to improve care. Methods We used two established hospital assessment tools to assess infrastructure, workforce, and capacity at all hospitals providing surgical care for children across Somaliland. We collected data on all surgical procedures performed in children in Somaliland between August 2016 and July 2017 using operative logbooks. Results Data were collected from 15 hospitals, including eight government, five for-profit, and two not-for-profit hospitals. Children represented 15.9% of all admitted patients, and pediatric surgical interventions comprised 8.8% of total operations. There were 0.6 surgical providers and 1.2 anesthesia providers per 100,000 population. A total of 1255 surgical procedures were performed in children in all hospitals in Somaliland over 1 year, at a rate of 62.4 surgical procedures annually per 100,000 children. Care was concentrated at private hospitals within urban areas, with a limited number of procedures for many high-burden pediatric surgical conditions. -
Email: [email protected]
Web: www.somalilandcsd.org Email: [email protected] This document is prepared in accordance with the standard procedures stated in the Code of Practice for Somaliland Official Statistics 2013. © November, 2020 All rights reserved Citation: Somaliland Central Statistics Department, 2020. Somaliland in Figures data 2019, Hargeisa – Somaliland. All correspondence should be directed to: Somaliland Central Statistics Department Minister of Planning and National Development Hargeisa, Somaliland Email: [email protected] Website: Somalilandcsd.org Map of Somaliland I Preface Complete, accurate and reliable statistics are an absolute requirement for efficient public action. Statistics inform decision makers and the broader community with critical information on the needs of the population and specific challenges they face. Quality data can reveal where resources are most needed, and provide the means to track progress and assess the impact of different plans and policies. Somaliland, as it is the case in many other developing countries, still lacks the capacity to regularly produce the full range and quality of statistics which are typically requires to effectively design, implement and monitor the relevant policies and plans needed for the country’s development. The need to fill that capacity gap becomes more pressing as Somaliland progresses. Indeed, raising complexity of the productive base and integration of the country in the global economy are two processes which can offer tremendous dividends to the population of Somaliland, but require sufficient, accurate and timely information to fully take effect. To face this challenge, the Government of Somaliland has undertaken various efforts to improve the overall capacity and functionality of its National Statistics System (NSS) coordinated by the Central Statistics Department (CSD) of the Ministry of Planning and National Development (MoPND), and in particular to reinforce the role of public institutions in the production of quality data. -
Private Health Care Services in a Fragile Country Context Somaliland Physicians’ Perspective
MASTER OF DISASTER MANAGEMENT [MDMa] Master’s Thesis 2013 Dirk Grothuesmann Gynaecologist Private Health Care Services in a Fragile Country Context Somaliland Physicians’ Perspective Supervisor: Tania Dræbel, PhD Department of International Health, Immunology & Microbiology Faculty of Health and Medical Sciences University of Copenhagen Denmark Abstract Fragile states and their complex problems are of international concern. About 15% of the world population live in a fragile country context. Fragile states are characterized by the inability of a government to provide basic functions such as security, legitimacy, governance, public health care. Frequently a vibrant, unregulated private health care sector is thriving. Information about the private health care sector is sparse. Hereby the private providers’ own perceptions about their services are nearly never heard. This study focuses on nationally accredited physicians and their private services in a fragile state (Somaliland). The objective of this study is to understand Somali physicians’ perspectives about their role and to identify opportunities for improved contribution. The methodology is based on in-depth interviews and personal observations of private facilities. Key- informant interviews provide required baseline information. The data analysis is based on a thematic analysis, compatible with a theoretical framework that is inspired by phenomenology. Three major themes evolved: Physicians’ own perceived significance of their services Access to services Health sector regulations The findings highlight the perceived importance of this sector, related to high quality care and utilization. Motivation to serve is based on both extrinsic (mainly financial) and intrinsic (recognition, appreciation, caring) factors. Intrinsic factors have perceived priority. Income is derived from customers with varying wealth, coming from all Somali speaking regions i.e. -

Hinari Participating Academic Institutions
Hinari Participating Academic Institutions Filter Summary Country City Institution Name Afghanistan Bamyan Bamyan University Chakcharan Ghor province regional hospital Charikar Parwan University Cheghcharan Ghor Institute of Higher Education Faizabad, Afghanistan Faizabad Provincial Hospital Ferozkoh Ghor university Gardez Paktia University Ghazni Ghazni University Ghor province Hazarajat community health project Herat Rizeuldin Research Institute And Medical Hospital HERAT UNIVERSITY 19-Dec-2017 3:13 PM Prepared by Payment, HINARI Page 1 of 367 Country City Institution Name Afghanistan Herat Herat Institute of Health Sciences Herat Regional Military Hospital Herat Regional Hospital Health Clinic of Herat University Ghalib University Jalalabad Nangarhar University Alfalah University Kabul Kabul asia hospital Ministry of Higher Education Afghanistan Research and Evaluation Unit (AREU) Afghanistan Public Health Institute, Ministry of Public Health Ministry of Public Health, Presidency of medical Jurisprudence Afghanistan National AIDS Control Program (A-NACP) Afghan Medical College Kabul JUNIPER MEDICAL AND DENTAL COLLEGE Government Medical College Kabul University. Faculty of Veterinary Science National Medical Library of Afghanistan Institute of Health Sciences Aga Khan University Programs in Afghanistan (AKU-PA) Health Services Support Project HMIS Health Management Information system 19-Dec-2017 3:13 PM Prepared by Payment, HINARI Page 2 of 367 Country City Institution Name Afghanistan Kabul National Tuberculosis Program, Darulaman Salamati Health Messenger al-yusuf research institute Health Protection and Research Organisation (HPRO) Social and Health Development Program (SHDP) Afghan Society Against Cancer (ASAC) Kabul Dental College, Kabul Rabia Balkhi Hospital Cure International Hospital Mental Health Institute Emergency NGO - Afghanistan Al haj Prof. Mussa Wardak's hospital Afghan-COMET (Centre Of Multi-professional Education And Training) Wazir Akbar Khan Hospital French Medical Institute for children, FMIC Afghanistan Mercy Hospital. -
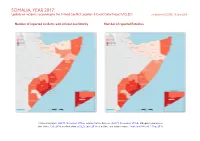
SOMALIA, YEAR 2017: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 18 June 2018
SOMALIA, YEAR 2017: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 18 June 2018 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; Ethiopia/Somalia bor- der status: CIA, 2014; incident data: ACLED, June 2018; coastlines and inland waters: Smith and Wessel, 1 May 2015 SOMALIA, YEAR 2017: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 18 JUNE 2018 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Battles 1200 644 2866 Conflict incidents by category 2 Violence against civilians 774 566 1040 Development of conflict incidents from 2008 to 2017 2 Remote violence 619 244 1964 Riots/protests 199 10 24 Methodology 3 Strategic developments 187 8 40 Conflict incidents per province 4 Non-violent activities 53 0 0 Localization of conflict incidents 4 Headquarters established 2 0 0 Total 3034 1472 5934 Disclaimer 7 This table is based on data from ACLED (datasets used: ACLED, June 2018). Development of conflict incidents from 2008 to 2017 This graph is based on data from ACLED (datasets used: ACLED, June 2018). 2 SOMALIA, YEAR 2017: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 18 JUNE 2018 Methodology an incident occured, or the provincial capital may be used if only the province is known. -

Rapid Assessment Report on the Current Drought Emergency in the Sanaag Region
Rapid Assessment Report on the Current Drought Emergency in the Sanaag Region July 2009 Figure 1 - Malnourished migrating camels near Dhahar (Sanaag region) 1 1. EXECUTIVE SUMMARY Following to the near total failure of the main Gu rainy season, in the month of June 2009, Horn Relief (HR) conducted two successive rapid emergency assessment in all livelihoods zones of Sanaag region (including the important pastoral hub of Sool Plateau as well as the renowned Sarar and Ban-Adde plains of El-Afweyn district), Eastern parts of Sool region including important pastoral areas in Hudun and Ainabo districts up to the Eastern part of the Togdheer region in Somaliland. The assessment team has focused primarily on the impact of the failure of the rains on the livelihoods of the affected population and the coping mechanisms they are using to adapt to the current crisis. Furthermore, for the hard-hit pastoralist communities in the Sool Plateau, the mission sought to possibly identify potential out- migration opportunities for the weakened livestock, i.e. availability of adequate and accessible water and pasture resources in as far as Western Sanaag, North-Eastern Sool region and Eastern Togdheer. The assessment teams found that the failure of the Gu rains in Sanaag region and the surrounding pastoral areas in Sool and Eastern Togdheer regions has already caused a substantial damage while it is still posing even more serious (and by the day worsening) threat to the livelihoods of both the urban poor and all wealth groups of the pastoral communities particularly in terms of food security and depletion of assets. -

TRIP FORM Prepared for Practice King's Somaliland Partnership
TRIP FORM Prepared for Practice King’s Somaliland Partnership Thank you for volunteering with the King’s Somaliland Partnership. Our work is only possible because of the hundreds of experts, like you, who volunteer their time to support the Somaliland health system. This Trip Form is the key document for capacity building activities in Somaliland, used by UK volunteers, Somaliland partners and UK programme staff. It serves three purposes: First, the Trip Form outlines key information, specifying the trip’s aims, outputs, contacts and context. Second it is a monitoring tool, helping us know the progress of our work. At its simplest this process is about numbers, from number of people trained to the male-to-female ratio. It is also about tracking: did the trip achieve what it set out to do? To what extent did Somaliland partners co- deliver activities? We report all this information to our donors as part of our commitment to accountability. Third, the Trip Form supports wider learning. Answering questions about outcomes, unanticipated success and challenges help us understand our immediate impacts, what’s working, what isn't, and why. We can then adapt our approach based on these findings, improving future trips and shaping our overall programme strategy. The Trip Form is filled out in stages by different people, divided into the following sections: A. Context B. Terms of Reference – to be completed before the trip by the volunteer leads C. Trip Report – to be completed during trip by the trip volunteers. We strongly encourage trip volunteers to seek and incorporate the views of Somaliland colleagues.