Skeletal System -Axial System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Part 1 the Thorax ECA1 7/18/06 6:30 PM Page 2 ECA1 7/18/06 6:30 PM Page 3
ECA1 7/18/06 6:30 PM Page 1 Part 1 The Thorax ECA1 7/18/06 6:30 PM Page 2 ECA1 7/18/06 6:30 PM Page 3 Surface anatomy and surface markings The experienced clinician spends much of his working life relating the surface anatomy of his patients to their deep structures (Fig. 1; see also Figs. 11 and 22). The following bony prominences can usually be palpated in the living subject (corresponding vertebral levels are given in brackets): •◊◊superior angle of the scapula (T2); •◊◊upper border of the manubrium sterni, the suprasternal notch (T2/3); •◊◊spine of the scapula (T3); •◊◊sternal angle (of Louis) — the transverse ridge at the manubrio-sternal junction (T4/5); •◊◊inferior angle of scapula (T8); •◊◊xiphisternal joint (T9); •◊◊lowest part of costal margin—10th rib (the subcostal line passes through L3). Note from Fig. 1 that the manubrium corresponds to the 3rd and 4th thoracic vertebrae and overlies the aortic arch, and that the sternum corre- sponds to the 5th to 8th vertebrae and neatly overlies the heart. Since the 1st and 12th ribs are difficult to feel, the ribs should be enu- merated from the 2nd costal cartilage, which articulates with the sternum at the angle of Louis. The spinous processes of all the thoracic vertebrae can be palpated in the midline posteriorly, but it should be remembered that the first spinous process that can be felt is that of C7 (the vertebra prominens). The position of the nipple varies considerably in the female, but in the male it usually lies in the 4th intercostal space about 4in (10cm) from the midline. -

Anatomy of the Spine
12 Anatomy of the Spine Overview The spine is made of 33 individual bones stacked one on top of the other. Ligaments and muscles connect the bones together and keep them aligned. The spinal column provides the main support for your body, allowing you to stand upright, bend, and twist. Protected deep inside the bones, the spinal cord connects your body to the brain, allowing movement of your arms and legs. Strong muscles and bones, flexible tendons and ligaments, and sensitive nerves contribute to a healthy spine. Keeping your spine healthy is vital if you want to live an active life without back pain. Spinal curves When viewed from the side, an adult spine has a natural S-shaped curve. The neck (cervical) and low back (lumbar) regions have a slight concave curve, and the thoracic and sacral regions have a gentle convex curve (Fig. 1). The curves work like a coiled spring to absorb shock, maintain balance, and allow range of motion throughout the spinal column. The muscles and correct posture maintain the natural spinal curves. Good posture involves training your body to stand, walk, sit, and lie so that the least amount of strain is placed on the spine during movement or weight-bearing activities. Excess body weight, weak muscles, and other forces can pull at the spine’s alignment: • An abnormal curve of the lumbar spine is lordosis, also called sway back. • An abnormal curve of the thoracic spine is Figure 1. (left) The spine has three natural curves that form kyphosis, also called hunchback. an S-shape; strong muscles keep our spine in alignment. -

Thoracic Cage EDU - Module 2 > Thorax & Spine > Thorax & Spine
Thoracic Cage EDU - Module 2 > Thorax & Spine > Thorax & Spine Thoracic cage • Protects the chest organs (the heart and lungs). Main Structures: The sternum (aka, breastbone) lies anteriorly. 12 thoracic vertebrae lie posteriorly. 12 ribs articulate with the thoracic vertebrae. Sternum • Manubrium (superiorly) • Body (long and flat, middle portion) • Xiphoid process - Easily injured during chest compression (for CPR). • Sternal angle - Where manubrium and body meet - Easily palpated to find rib 2 • Sternal indentations: - Jugular notch (aka, suprasternal notch) is on the superior border of the manubrium. - Clavicular notches are to the sides of the jugular notch; these are where the clavicles (aka, collarbones), articulate with the sternum. - Costal notches articulate with the costal cartilages of the ribs ("costal" refers to the ribs). Rib Types • True ribs - Ribs 1-7; articulate with the sternum directly via their costal cartilages. • False ribs - Ribs 8-12; do not articulate directly with the sternum. - Ribs 11 and 12 are "floating ribs," do not articulate at all with the sternum. 1 / 2 Rib Features • Head - Articulates with the vertebral body; typically comprises two articular surfaces separated by a bony crest. • Neck - Extends from the head, and terminates at the tubercle. • Tubercle - Comprises an articular facet, which is where the rib articulates with the transverse process of the vertebra. • Shaft - Longest portion of the rib, extends from tubercle to rib end. • Angle - Bend in rib, just lateral to tubercle. Rib/vertebra articulation • Head and tubercle of rib articulate with body and thoracic process of vertebrae. Intercostal spaces • The spaces between the ribs • House muscles and neurovascular structures. -
Changes in L4/5 Intervertebral Foramen Bony Morphology With
www.nature.com/scientificreports OPEN Changes in L4/5 Intervertebral Foramen Bony Morphology with Age Received: 7 September 2017 Shuaifeng Yan, Kai Wang, Yunfan Zhang, Song Guo, Yan Zhang & Jun Tan Accepted: 1 May 2018 The purpose of this study was to explore the morphological changes in L4/5 intervertebral foramen Published: xx xx xxxx with age using a digital method. The closed boundaries of the intervertebral foramen (IGES) in diferent sagittal slices (inside, middle and outside) were obtained from Mimics, and then imported to a custom- written program, which provided quantitative distance between the nerve root and the closed curves. The quantitative information of each age group was used to produce radar chart and line chart for morphological and statistical analyses. Overall, the intervertebral foramen changes mainly occurred in the inner part from middle age to old age. The foraminal height decreased with age in the inside sagittal slice, while no signifcant diference was found in the middle sagittal slice or the outside sagittal slice. The foraminal width showed no decrease in each age group or each sagittal plane. The present study described foraminal geometry of asymptomatic males in diferent sagittal slices with age. This information enhances the knowledge of anatomical changes in intervertebral foramen with age, which provides better understanding of the pathology of intervertebral foramen diseases. Low back pain (LBP) is a global health problem, causing enormous fnancial burden1,2. Te lifetime prevalence of LBP is reported to be as high as 84%3. Radiculopathy is a common cause of low back and leg pain4. In general, radiculopathy caused by foramen stenosis consists of 8–11% nerve root compression5, and shows an increasing trend6. -

Chapter 02: Netter's Clinical Anatomy, 2Nd Edition
Hansen: Netter's Clinical Anatomy, 2nd Edition - with Online Access 2 BACK 1. INTRODUCTION 4. MUSCLES OF THE BACK REVIEW QUESTIONS 2. SURFACE ANATOMY 5. SPINAL CORD 3. VERTEBRAL COLUMN 6. EMBRYOLOGY FINAL 1. INTRODUCTION ELSEVIERl VertebraeNOT prominens: the spinous process of the C7- vertebra, usually the most prominent The back forms the axis (central line) of the human process in the midline at the posterior base of body and consists of the vertebral column, spinal cord, the neck supporting muscles, and associated tissues (skin, OFcon- l Scapula: part of the pectoral girdle that sup- nective tissues, vasculature, and nerves). A hallmark of ports the upper limb; note its spine, inferior human anatomy is the concept of “segmentation,” and angle, and medial border the back is a prime example. Segmentation and bilat l Iliac crests: felt best when you place your eral symmetry of the back will be obvious as you hands “on your hips”; an imaginary horizontal study the vertebral column, the distribution of the line connecting the crests passes through the spinal nerves, the muscles of th back, and its vascular spinous process of the L4 vertebra and the supply. intervertebral disc of L4-L5, a useful landmark Functionally, the back is involved in three primary for a lumbar puncture or epidural block tasks: l Posterior superior iliac spines: an imaginary CONTENThorizontal line connecting these two points l Support: the vertebral column forms the axis of passes through the spinous process of S2 (second the body and is critical for our upright posture sacral segment) (standing or si ting), as a support for our head, as an PROPERTYattachment point and brace for move- 3. -

1 the Thoracic Wall I
AAA_C01 12/13/05 10:29 Page 8 1 The thoracic wall I Thoracic outlet (inlet) First rib Clavicle Suprasternal notch Manubrium 5 Third rib 1 2 Body of sternum Intercostal 4 space Xiphisternum Scalenus anterior Brachial Cervical Costal cartilage plexus rib Costal margin 3 Subclavian 1 Costochondral joint Floating ribs artery 2 Sternocostal joint Fig.1.3 3 Interchondral joint Bilateral cervical ribs. 4 Xiphisternal joint 5 Manubriosternal joint On the right side the brachial plexus (angle of Louis) is shown arching over the rib and stretching its lowest trunk Fig.1.1 The thoracic cage. The outlet (inlet) of the thorax is outlined Transverse process with facet for rib tubercle Demifacet for head of rib Head Neck Costovertebral T5 joint T6 Facet for Tubercle vertebral body Costotransverse joint Sternocostal joint Shaft 6th Angle rib Costochondral Subcostal groove joint Fig.1.2 Fig.1.4 A typical rib Joints of the thoracic cage 8 The thorax The thoracic wall I AAA_C01 12/13/05 10:29 Page 9 The thoracic cage Costal cartilages The thoracic cage is formed by the sternum and costal cartilages These are bars of hyaline cartilage which connect the upper in front, the vertebral column behind and the ribs and intercostal seven ribs directly to the sternum and the 8th, 9th and 10th ribs spaces laterally. to the cartilage immediately above. It is separated from the abdominal cavity by the diaphragm and communicates superiorly with the root of the neck through Joints of the thoracic cage (Figs 1.1 and 1.4) the thoracic inlet (Fig. -
The Axial Skeleton Visual Worksheet
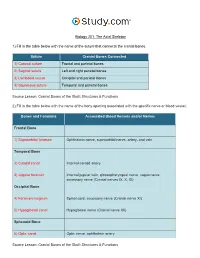
Biology 201: The Axial Skeleton 1) Fill in the table below with the name of the suture that connects the cranial bones. Suture Cranial Bones Connected 1) Coronal suture Frontal and parietal bones 2) Sagittal suture Left and right parietal bones 3) Lambdoid suture Occipital and parietal bones 4) Squamous suture Temporal and parietal bones Source Lesson: Cranial Bones of the Skull: Structures & Functions 2) Fill in the table below with the name of the bony opening associated with the specific nerve or blood vessel. Bones and Foramina Associated Blood Vessels and/or Nerves Frontal Bone 1) Supraorbital foramen Ophthalmic nerve, supraorbital nerve, artery, and vein Temporal Bone 2) Carotid canal Internal carotid artery 3) Jugular foramen Internal jugular vein, glossopharyngeal nerve, vagus nerve, accessory nerve (Cranial nerves IX, X, XI) Occipital Bone 4) Foramen magnum Spinal cord, accessory nerve (Cranial nerve XI) 5) Hypoglossal canal Hypoglossal nerve (Cranial nerve XII) Sphenoid Bone 6) Optic canal Optic nerve, ophthalmic artery Source Lesson: Cranial Bones of the Skull: Structures & Functions 3) Label the anterior view of the skull below with its correct feature. Frontal bone Palatine bone Ethmoid bone Nasal septum: Perpendicular plate of ethmoid bone Sphenoid bone Inferior orbital fissure Inferior nasal concha Maxilla Orbit Vomer bone Supraorbital margin Alveolar process of maxilla Middle nasal concha Inferior nasal concha Coronal suture Mandible Glabella Mental foramen Nasal bone Parietal bone Supraorbital foramen Orbital canal Temporal bone Lacrimal bone Orbit Alveolar process of mandible Superior orbital fissure Zygomatic bone Infraorbital foramen Source Lesson: Facial Bones of the Skull: Structures & Functions 4) Label the right lateral view of the skull below with its correct feature. -
Bones of the Trunk
BONES OF THE TRUNK Andrea Heinzlmann Veterinary University Department of Anatomy and Histology 16th September 2019 VERTEBRAL COLUMN (COLUMNA VERTEBRALIS) • the vertebral column composed of the vertebrae • the vertebrae form a horizontal chain https://hu.pinterest.com/pin/159877855502035893/ VERTEBRAL COLUMN (COLUMNA VERTEBRALIS) along the vertebral column three major curvatures are recognized: 1. the DORSAL CONVEX CURVATURE – between the head and the neck 2. the DORSAL CONCAVE CURVATURE – between the neck and the chest 3. the DORSAL CONVEX CURVATURE – between the thorax and the lumbar region - in carnivores (Ca) there is an additional DORSAL CONVEXITY in the sacral region https://hu.pinterest.com/pin/159877855502035893/ VERTEBRAL COLUMN (COLUMNA VERTEBRALIS) - corresponding to the regions of the body, we distinguish: 1. CERVICAL VERTEBRAE 2. THORACIC VERTEBRAE 3. LUMBAR VERTEBRAE 4. SACRAL VERTEBRAE 5. CAUDAL (COCCYGEAL) VERTEBRAE https://www.ufaw.org.uk/dogs/french-bulldog-hemivertebrae https://rogueshock.com/know-your-horse-in-9-ways/5/ BUILD OF THE VERTEBRAE each vertebrae presents: 1. BODY (CORPUS VERTEBRAE) 2. ARCH (ARCUS VERTEBRAE) 3. PROCESSES corpus Vertebra thoracica (Th13) , Ca. THE VERTEBRAL BODY (CORPUS VERTEBRAE) - the ventral portion of the vertebra ITS PARTS: 1. EXTREMITAS CRANIALIS (seu CAPUT VERTEBRAE) – convex 2. EXTREMITAS CAUDALIS (seu FOSSA VERTEBRAE) - concave Th13, Ca. THE VERTEBRAL BODY (CORPUS VERTEBRAE) 3. VENTRAL SURFACE of the body has a: - ventral crest (CRISTA VENTRALIS) 4. DORSAL SURFACE of the body carries : - the vertebral arch (ARCUS VERTEBRAE) Th13, Ca., lateral aspect Arcus vertebrae corpus Vertebra thoracica (Th13) , Ca., caudal aspect THE VERTEBRAL BODY (CORPUS VERTEBRAE) 6. VERTEBRAL ARCH (ARCUS VERTEBRAE) compraisis: a) a ventral PEDICULUS ARCUS VERTEBRAE b) a dorsal LAMINA ARCUS VERTEBRAE C7, Ca. -
Axial Skeleton 214 7.7 Development of the Axial Skeleton 214
SKELETAL SYSTEM OUTLINE 7.1 Skull 175 7.1a Views of the Skull and Landmark Features 176 7.1b Sutures 183 7.1c Bones of the Cranium 185 7 7.1d Bones of the Face 194 7.1e Nasal Complex 198 7.1f Paranasal Sinuses 199 7.1g Orbital Complex 200 Axial 7.1h Bones Associated with the Skull 201 7.2 Sex Differences in the Skull 201 7.3 Aging of the Skull 201 Skeleton 7.4 Vertebral Column 204 7.4a Divisions of the Vertebral Column 204 7.4b Spinal Curvatures 205 7.4c Vertebral Anatomy 206 7.5 Thoracic Cage 212 7.5a Sternum 213 7.5b Ribs 213 7.6 Aging of the Axial Skeleton 214 7.7 Development of the Axial Skeleton 214 MODULE 5: SKELETAL SYSTEM mck78097_ch07_173-219.indd 173 2/14/11 4:58 PM 174 Chapter Seven Axial Skeleton he bones of the skeleton form an internal framework to support The skeletal system is divided into two parts: the axial skele- T soft tissues, protect vital organs, bear the body’s weight, and ton and the appendicular skeleton. The axial skeleton is composed help us move. Without a bony skeleton, we would collapse into a of the bones along the central axis of the body, which we com- formless mass. Typically, there are 206 bones in an adult skeleton, monly divide into three regions—the skull, the vertebral column, although this number varies in some individuals. A larger number of and the thoracic cage (figure 7.1). The appendicular skeleton bones appear to be present at birth, but the total number decreases consists of the bones of the appendages (upper and lower limbs), with growth and maturity as some separate bones fuse. -

Radiographic Anatomy of the Intervertebral Cervical and Lumbar Foramina 691
Diagnostic and Interventional Imaging (2012) 93, 690—697 View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector CONTINUING EDUCATION PROGRAM: FOCUS. Radiographic anatomy of the intervertebral cervical and lumbar foramina (vessels and variants) ∗ X. Demondion , G. Lefebvre, O. Fisch, L. Vandenbussche, J. Cepparo, V. Balbi Service de radiologie musculosquelettique, CCIAL, laboratoire d’anatomie, faculté de médecine de Lille, hôpital Roger-Salengro, CHRU de Lille, rue Émile-Laine, 59037 Lille, France KEYWORDS Abstract The intervertebral foramen is an orifice located between any two adjacent verte- Spine; brae that allows communication between the spinal (or vertebral) canal and the extraspinal Spinal cord; region. Although the intervertebral foramina serve as the path traveled by spinal nerve roots, Vessels vascular structures, including some that play a role in vascularization of the spinal cord, take the same path. Knowledge of this vascularization and of the origin of the arteries feeding it is essential to all radiologists performing interventional procedures. The objective of this review is to survey the anatomy of the intervertebral foramina in the cervical and lumbar spines and of spinal cord vascularization. © 2012 Éditions françaises de radiologie. Published by Elsevier Masson SAS. All rights reserved. The intervertebral foramen is an orifice located between any two adjacent vertebrae that allows communication between the spinal (or vertebral) canal and the extraspinal region. Although the intervertebral foramina serve as the path traveled by spinal nerve roots, vascular structures, including some that play a role in vascularization of the spinal cord, take the same path. Knowledge of this vascularization and of the source of the arteries feeding the spinal cord is therefore essential to all radiologists performing interventional procedures in view of the iatrogenic risks they present. -

Protrusion of the Lung Apex Through Sibson's Fascia in Infancy
Thorax: first published as 10.1136/thx.33.3.290 on 1 June 1978. Downloaded from Thorax, 1978, 33, 290-294 Protrusion of the lung apex through Sibson's fascia in infancy MICHAEL GRUNEBAUM1 AND N. THORNE GRISCOM From the Department of Radiology, The Children's Hospital Medical Center and Harvard Medical School, Boston, Massachusetts 02115, USA Grunebaum, M., and Griscom, N. T. (1978). Thorax, 33, 290-294. Protrusion of the lung apex through Sibson's fascia in infancy. Apical 'herniation' of the lung is an unusual protrusion of the lung and its pleural coverings through the superior aperture of the thorax. It is supposedly caused by weakness of Sibson's fascia. The phenomenon is an anatomical variation and not a disease entity; however, it must be recognised in order to avoid inappropriate surgery. The condition apparently disappears spontaneously with growth. Protrusion of the lung parenchyma into the neck After recovering from his respiratory distress, is uncommon (Reinhart and Hermel, 1951; which was thought to be due to croup, the infant Munnell, 1968), especially in children (Bronsther was sent for radiological investigation with the et al., 1968; Thompson, 1976). Descriptions of this referring diagnosis of laryngocoele. Plain films phenomenon during the first year of life are rare showed a gas-containing structure in front of and (Palazzo and Garrett, 1951; Cunningham and to the right of the trachea just above the supra- Peters, 1969). Of the eight patients with protru- sternal notch. The trachea seemed to be displaced http://thorax.bmj.com/ sion of the apex of the lung through Sibson's backwards and slightly narrowed (Fig. -

Spinal Nerve Position and Morphometric Analysis with Silicon Molds in the Cadaveric Lumbar Intervertebral Foramen
대한체질인류학회지 제 31 권 제 4 호 Korean J Phys Anthropol Vol. 31, No. 4 (2018) pp. 151~158 https://doi.org/10.11637/kjpa.2018.31.4.151 Original Article Spinal Nerve Position and Morphometric Analysis with Silicon Molds in the Cadaveric Lumbar Intervertebral Foramen Soonwook Kwon Department of Anatomy, School of Medicine, Catholic University of Daegu (Received 4 December 2018, revised 14 December 2018, accepted 17 December 2018) Abstract : The intervertebral foramen is formed by two adjacent vertebrae and an intervertebral disc. Previous studies examining the foramen have been performed using various methods. The author obtained characteristics of the intervertebral foramen based on silicon mold. The author used 18 cadavers and dissected the lumbar intervertebral foramen. First, positional levels of the spinal nerve in the intervertebral foramen were measured. Second, after being removed all tissues covering the intervertebral, bony foramen was filled with melted silicon to mold the cross section. Subsequently, the solidified silicon mold was removed and stamped on a paper. The paper was scanned and analyzed area, perimeter, height and width of the intervertebral foramen on a computer. Area (average, 9.43 mm2) and perimeter (average, 48.02 mm) did not show any statistical significant pattern for any lumbar vertebral levels. However, the height and width significantly differed at the fifth lumbar vertebra, which had the shortest height (the fifth, 13.00 mm; average, 15.78 mm) and longest width (the fifth, 8.61 mm; average, 7.87 mm), although there were similar patterns in case of area and perimeter of the first to fourth lumbar vertebra.