US Department of Veterans Affairs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

AAFP Letter to CMS on Prior Authorizations in Medicare
February 28, 2019 The Honorable Seema Verma Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services Hubert H. Humphrey Building, Room 445–G 200 Independence Avenue, SW Washington, DC 20201 Dear Administrator Verma: The undersigned organizations are writing to urge the Centers for Medicare & Medicaid Services (CMS) to provide guidance to Medicare Advantage (MA) plans on prior authorization (PA) processes through its 2020 Call Letter. CMS’ guidance should direct plans to target PA requirements where they are needed most. Specifically, CMS should require MA plans to selectively apply PA requirements and provide examples of criteria to be used for such programs, including, for example, ordering/prescribing patterns that align with evidence- based guidelines and historically high PA approval rates. At a time when CMS has prioritized regulatory burden reduction in the patient-provider relationship through its Patients Over Paperwork initiative, we believe such guidance will help promote safe, timely, and affordable access to care for patients; enhance efficiency; and reduce administrative burden on physician practices. A Consensus Statement on Improving the Prior Authorization Process, issued by the AMA, the American Hospital Association, America’s Health Insurance Plans, the American Pharmacists Association, Blue Cross Blue Shield Association, and the Medical Group Management Association in January 2018, identified opportunities to improve the prior authorization process, with the goals of promoting safe, timely, and affordable access to evidence-based care for patients; enhancing efficiency; and reducing administrative burdens.1 It notes that the PA process can be burdensome for all involved—health care providers, health plans, and patients—and that plans should target PA requirements where they are needed most. -

June 9, 2020 the Honorable Nancy Pelosi the Honorable Mitch
June 9, 2020 The Honorable Nancy Pelosi The Honorable Mitch McConnell Speaker of the House of Representatives Senate Majority Leader U.S. Capitol Building, H-222 U.S. Capitol Building, S-230 Washington, DC 20515 Washington, DC 20510 The Honorable Kevin McCarthy The Honorable Charles Schumer House Republican Leader Senate Democratic Leader U.S. Capitol Building, H-204 U.S. Capitol Building, S-221 Washington, DC 20515 Washington, DC 20510 Dear Speaker Pelosi, Leader McConnell, Leader McCarthy, and Leader Schumer: The undersigned state, specialty, and national medical associations represent hundreds of thousands of frontline medical and mental health physicians who are diagnosing, testing, treating, and counseling millions of our nation’s patients in response to the COVID-19 pandemic. During this unprecedented national health emergency, physicians and other health care professionals have been putting themselves at risk every day while facing shortages of medical supplies and safety equipment, and making critical medical decisions based on changing directives and guidance. These physicians and other health care professionals are now facing the threat of years of costly litigation due to the extraordinary circumstances. As the House and Senate continue to work on the next COVID-19 relief package, we strongly urge you to include the targeted and limited liability protections that are in the bipartisan bill, H.R. 7059, the “Coronavirus Provider Protection Act.” The public health emergency triggered by the COVID-19 pandemic has created unprecedented challenges to our nation’s health care system. In addition to facing inadequate supplies and safety equipment, physicians, hospitals, and other frontline health care professionals have been faced with rapidly changing guidance and directives from all levels of government. -
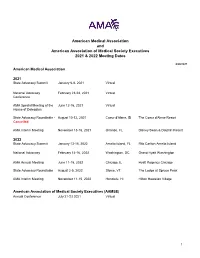
AMA and AAMSE 2021 & 2022 Meeting Dates
American Medical Association and American Association of Medical Society Executives 2021 & 2022 Meeting Dates 6/28/2021 American Medical Association 2021 State Advocacy Summit January 6-8, 2021 Virtual National Advocacy February 23-24, 2021 Virtual Conference AMA Special Meeting of the June 12-16, 2021 Virtual House of Delegates State Advocacy Roundtable - August 10-12, 2021 Coeur d'Alene, ID The Coeur d'Alene Resort Cancelled AMA Interim Meeting November 13-16, 2021 Orlando, FL Disney Swan & Dolphin Resort 2022 State Advocacy Summit January 13-15, 2022 Amelia Island, FL Ritz Carlton Amelia Island National Advocacy February 14-16, 2022 Washington, DC Grand Hyatt Washington AMA Annual Meeting June 11-15, 2022 Chicago, IL Hyatt Regency Chicago State Advocacy Roundtable August 2-5, 2022 Stowe, VT The Lodge at Spruce Peak AMA Interim Meeting November 11-15, 2022 Honolulu, HI Hilton Hawaiian Village American Association of Medical Society Executives (AAMSE) Annual Conference July 21-23 2021 Virtual 1 State Medical Society Meetings Alaska State Medical Association Annual Meeting May 8, 2021 Virtual Arizona Medical Association Annual Meeting April 16-17, 2021 Virtual Arkansas Medical Society Annual Meeting May 12, 2021 Virtual California Medical Association Annual Meeting October 23-24, 2021 Los Angeles, CA Marriott LA Live Colorado Medical Society Annual Meeting September 18, 2021 Virtual Connecticut State Medical Society Annual Meeting September, TBD, 2021 TBD TBD Florida Medical Association Annual Meeting July 31 - August 1, 2021 Orlando, -

AAFP Response to VHA Health Professionals Scope of Practice
January 7, 2021 Robert Wilkie Secretary Department of Veterans Affairs 810 Vermont Ave. NW, Room 1068 Washington, DC 20420 Re: RIN 2900–AQ94—Authority of VA Professionals to Practice Health Care Dear Secretary Wilkie, The undersigned physician organizations representing national specialty and state medical societies are writing in opposition to the Department of Veterans Affairs’ Interim Final Rule, entitled “Authority of VA Professionals to Practice Health Care,” which permits virtually all VHA-employed non-physician providers (NPPs) to practice without the clinical supervision of physicians and without regard to state scope of practice law. NPPs are an integral part of physician-led health care teams. However, NPPs cannot substitute for physicians especially when it comes to diagnosing complex medical conditions, developing comprehensive treatment plans, ensuring that procedures are properly performed, and managing highly involved and complicated patient cases. Nowhere is this more important than at the Department of Veterans Affairs (VA), which delivers multifaceted medical care to veterans, including those with traumatic brain injuries and other serious medical and mental health issues. As such, our nation’s veterans deserve high quality health care that is overseen by physicians. For the reasons below, the undersigned organizations strongly oppose the Interim Final Rule (IFR) and urge the VA to rescind the IFR and consider policy alternatives that prioritize physician led team-based care. The IFR violates the Administrative Procedure -

Public Health and Patient Protection
SUMMER 2011 PUBLIC HEALTH AND ALSo… PATIENT PROTECTION • Electronic Medical Records - The Path The Future of Integrated Delivery Systems: Forward for Maryland Primary Care and Public Health Partnerships in Physicians Care Coordination • MD-Tech: Use Your The Importance of Reporting Drug Adverse Events EMR Meaningfully: Streamline the Team! Early Breast Cancer and Modern Healthcare This Edition Approved for 2.5 CME Credits. Ovarian Cancer: Are Physicians Under-Screening Complete and Submit Journal CME Quiz at for a Silent Killer? www.mdafp.org. THE MARYLAND familydoctor / SUMMER 2011 • 1 Place your trust in Maryland’s leading medical professional liability insurer. You work in a challenging world where outsiders often use 20-20 hindsight to second-guess health care decisions you’ve made for your patients. As a result, litigation can strike at any time. Fortunately, since 1975, Medical Mutual has been here to protect your practice and professional reputation. Our unyielding and proactive claims defense gives you the confidence you need to practice good medicine. That’s why more Maryland Doctors depend on Medical Mutual than all other medical professional liability carriers combined. 225 International Circle | Hunt Valley, Maryland 21030 | 410-785-0050 | 800-492-0193 2 • THE MARYLAND familydoctor / SUMMER 2011 THE MARYLAND familydoctor Summer 2011 Volume 48, Number 1 contents FEATURES The Future of Integrated Delivery Systems: 12 Primary Care and Public Health Partnerships in Care Coordination by Andrea Mathias, M.D., MPH The Importance of Reporting Drug Adverse Events 15 by Jasmine Chen Gatti, M.D. Early Breast Cancer and Modern Healthcare 17 by Niharika Khanna, M.D. -

American Osler Society
49th Annual Meeting of the American Osler Society Sir William Osler, quoting Leigh Hunt, “Abou Ben Adhem” Sunday, May 12th – Wednesday May 15th, 2019 Hotel Omni Mont-Royal Montréal, Canada Hotel Omni Mont-Royal 49th Annual Meeting of the AMERICAN OSLER SOCIETY Sunday, May 12th – Wednesday, May 15th, 2019 Hotel Omni Mont-Royal Montréal, Canada Credit: Karen Koshof The Osler Niche contains the ashes of Sir William Osler and Lady Osler, as well as those of Osler’s dear cousin and first Librarian of the Osler Library, W.W. Francis. The Niche was designed with Osler’s wishes in mind. Its realization was not far off the vision imagined by Osler’s alter ego Egerton Yorrick Davis in “Burrowings of a Bookworm”: I like to think of my few books in an alcove of a fire-proof library in some institution that I love; at the end of the alcove an open fire-place and a few easy chairs, and on the mantelpiece an urn with my ashes and my bust or portrait through which my astral self, like the Bishop at St. Praxed’s, could peek at the books I have loved, and enjoy the delight with which kindred souls still in the flesh would handle them. Course Objectives Upon conclusion of this program, participants should be able to: Describe new research findings in the history of medicine. Outline the evolution of medicine in a particular disease. List professional contributions made by others in medicine. Intended Audience The target audience includes physicians and others interested in Osler, medical history and any of the medically oriented humanities who research and write on a range of issues. -

32Nd Annual Report to the Community
32nd Annual Report to the Community JULY 2017–JUNE 2018 DEAR FRIENDS, The ancient Greek philosopher Heraclitus of Ephesus (c. 500 BC) is credited with saying “change is the only constant in life.” With these words, Heraclitus has successfully influenced the way that we look at, consider, embrace, reject, and celebrate change. The Community Foundation has been influencing change since 1986 by way of every donor’s vision and desire to transform and improve the community. In 2011, the board of trustees made an intentional decision to increase influence through strategic grantsmaking based on its Frederick County Human Needs Assessment. Now, in 2018, the Needs Assessment has been updated, and the influence for change continues as the outcomes are studied and strategic grantsmaking evolves as a result. “Influence for change” is only possible because of “U” and the way “U” see the future of Frederick County and its residents. “U” is the most important letter in the word “Influence” because “U” are the most important driver in the Community Foundation’s efforts to address the pressing needs in the community. The community’s efforts to influence change in FY2018 was evident by the 1,740 donors who made more than 3,400 gifts to one or more of 700 funds. Most gifts were added to our existing endowment that spends 5 percent of the annual market value in grants and scholarships. Grants benefitted more than 250 nonprofits, and nearly 300 students received scholarships for post-secondary education or trade and technical training. In addition to education, areas that were supported by grants included youth programs, elder care, historic preservation, health care, health and human services, those who were homeless or precariously housed, animal welfare, the environment, the arts, civic causes, and more. -

American Medical Association Resident and Fellow Section
MEDICAL SOCIETY OF DELAWARE COUNCIL Resolution: 01 (A-19) Introduced by: Psychiatric Society of Delaware Neil S. Kaye, MD, DLFAPA Subject: Commitment to Ethics Whereas, The medical profession has adhered to a Code of Ethics since the 5th Century BCE; and Whereas, Such Codes have included the Oath of Hippocrates and the Oath of Maimonides; and Whereas, In 1803 Thomas Percival introduced our country’s first medical ethics standards; and Whereas, These codes were adopted by the AMA in 1847; and Whereas, The Code of Medical Ethics has been revised continuously, most recently in 2016; and Whereas, Forces from both within the house of medicine and outside of the house of medicine continually try to influence the practice of medicine; and Whereas, What has never changed in any of these ethical codes is the requirement that physicians focus 100% of their efforts on healing; therefore be it RESOLVED, That the Medical Society of Delaware will continue to recognize the AMA Code of Medical Ethics as binding on all decisions made by the organization and its members; and be it further RESOLVED, That the Medical Society of Delaware will actively resist all attempts to lessen its ethical standards as enumerated in the AMA Code of Medical Ethics. Fiscal Note: Undetermined 1American Medical Association. Code of Medical Ethics of the American Medical Association. Chicago, IL: American Medical Association; 2017 MEDICAL SOCIETY OF DELAWARE COUNCIL Resolution: 02 (A-19) Introduced by: Robert J. Varipapa, MD Subject: MSD Support of Medical Aid in Dying (MAID) -

Secretary of Veterans' Affairs
June 24, 2020 The Honorable Robert Wilkie Secretary U.S. Department of Veterans Affairs 810 Vermont Avenue NW, Room 1063B Washington, DC 20420 Dear Secretary Wilkie: The undersigned medical associations and medical specialty societies are writing to register serious concerns with the Health Care Professional Practice in VA Memorandum (Memorandum) issued by the Office of the Under Secretary of Health on April 21, 2020, and underlying Directive 1899 (Directive). The undersigned organizations urge the Secretary to amend Directive 1899 as it relates to allowing non-physician healthcare professionals in 32 specialties to operate “within the full scope of their license, registration, or certification” and rescind the Memorandum as it relates to encouraging all VA medical facilities to allow CRNAs to practice without physician oversight during the national health emergency. The undersigned organizations are very concerned Directive 1899 preempts state scope of practice laws. Directive 1899 memorializes U.S. Department of Veterans Affairs (VA) policy allowing VA health care professionals to practice across state lines and establishes new policy allowing VA health care professionals to operate within the full scope of their license, registration, or certification. This combination in effect circumvents state scope of practice laws for the 32 health care professionals defined in the directive. Such a far-reaching expansion is overly broad, unnecessary and threatens the health and safety of patients within the VA system. As state scope of practice laws vary across these professions and across states, we urge the Secretary to amend the directive to defer to state scope of practice laws, similar to the language related to psychologists in Appendix B of the Directive. -

State Medical Society Membership Requirements
State Medical Society Membership Requirements State Medical Society Representation‐ Updated June 2013 Recently, ASAM staff contacted each state medical society requesting required procedures for ASAM chapters to obtain official membership in the medical society’s governing body. Below are the responses received – Alaska: ASMA’s current bylaws call for House of Delegate members to be elected by the local medical society. There is no representation of specialty societies within the House of Delegates. Arizona: A state specialty or subspecialty society with 250 or fewer members shall be entitled to representation in the House of Delegates by one delegate and a specialty or subspecialty society with more than 250 members shall be entitled to 2 delegates if (1) the specialty or subspecialty is recognized by the American Board of Medical Specialties; (2) the specialty or subspecialty society has a minimum of twenty members practicing in Arizona; (3) the specialty or subspecialty society maintains an existing organization or structure with a slate of periodically elected officers, a constitution and bylaws and a frequency of meeting at least once a year; (4) by a vote of the House it shall be deemed to be in the best interests of the Association. Specialty or subspecialty society delegates shall be the society president or designee(s) who shall be members of the Association (http://www.azmed.org/arma‐governance). California: Each statewide specialty organization recognized by the House of Delegates shall be entitled to one (1) delegate and one (1) alternate. Specialty organizations having five hundred (500) or more members who are regular active members of CMA shall have one (1) additional delegate and alternate, plus one additional delegate and alternate for each full five hundred (500) members thereafter who are regular active members of CMA. -

Joint Letter to CMS to Sunset Waivers When PHE Concludes
July 22, 2020 The Honorable Seema Verma Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services Hubert H. Humphrey Building, Room 445-G 200 Independence Avenue, SW Washington, DC 20201 Dear Administrator Verma: The undersigned organizations represent the hundreds of thousands of physicians who provide care for our nation’s Medicare patients every day. We are writing to strongly support the Centers for Medicare & Medicaid Services (CMS) decision to temporarily waive certain regulatory requirements during the COVID-19 pandemic. These temporary waivers, in extraordinary circumstances, have empowered physicians and non-physician health care professionals to focus on their patients and prevented a collapse of the health care system in the hardest hit areas of the country. However, we urge CMS to sunset the waivers involving scope of practice and licensure when the public health emergency (PHE) concludes. To our dismay, it is our understanding that some organizations have already been advocating to make the temporary waivers permanent—permanently diminishing physician oversight and supervision of patient care. While we are greatly appreciative of CMS’ rapid and substantial removal of regulatory barriers to allow physicians to continue providing care during the PHE, we also strive to continue to work with CMS to support patient access to physician-led care teams during and after the PHE. Throughout the coronavirus pandemic, physicians, nurses, and the entire health care community have been working side-by-side caring for patients and saving lives. Now more than ever, we need health care professionals working together as part of physician-led health care teams. -

Winter 2020 Roland Park News
Quarterly from the Roland Park Community Foundation • Volume Seventy-Nine • Winter 2020 Feeding Students, Finding Solutions Keeping Watch on the Tower 2 Volume 79 • Winter 2020 Dan McIntyre (1956-2020): Table of Contents i Dan McIntyre (1956-2020): A Personal Recollection A Personal Recollection 1 Feeding Students, Finding Solutions: Dan McIntyre was a 30-year Roland Park tell that he didn’t remember me. But after One Principal’s COVID-19 Response resident and community leader, active in that nanosecond, he forced a smile and 3 Sidney Brower (1930-2020): A Good both the Civic League and the Community welcomed me in. He asked about my Neighbor Foundation. Many people remember Dan family and the old Alex. Brown gang in the 4 A COVID-19 Update rolling up Roland Avenue in his wheelchair, States. He was lying there, broken and in 6 Keeping Watch on the Tower: talking to friends and neighbors. Dan passed pain, but solely focused on making me feel Terry Ross away recently and one of those friends, Hap comfortable. I still get misty when I recall 7 Greater Roland Park Home Sales Cooper, remembers him fondly. that visit and what a gentleman he was. 8 The Park School’s StoryWalk I met Dan McIntyre when we had both just The McIntyres returned to Roland Park 10 Community Foundation Update: joined the Legal and Marketing departments shortly thereafter and, by coincidence, The Baltimore Country Club Land at Alex. Brown. He was tall, soft-spoken and we lived five houses apart. Our families 11 Notes from the Garden: To Stack Stones appropriate—with a wry sense of humor.