Acupuncture Consent Form
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
TM/CAM Update First Quarter 2011
New Zealand Centre for Evidence‐based Research into Complementary and Alternative Medicine (ENZCAM) ENZCAM Newsletter TM/CAM Update First Quarter 2011 The purpose of this update on traditional medicine and complementary medicine (TM/CAM) is to inform healthcare professionals, researchers, funders and policy‐makers about developments. The update provides links to new material published or released as well as links to classic resources on traditional, complementary and integrative medicine as we gather them for the web‐site. 1. Policy and Legislation World Health Organization (WHO) The World Health Organization (WHO) has a site devoted to Traditional Medicine (TM), including Complementary and Alternative Medicine (CAM). See http://www.who.int/medicines/areas/traditional/en/index.html The first ENZCAM Brief for Professionals will deal in more detail with WHO policy with respect to TM/CAM. 2. Research Organisations National Center for Complementary and Alternative Medicine (NCCAM) The National Center for Complementary and Alternative Medicine (NCCAM), is part of the National Institutes of Health (NIH) in the USA. http://nccam.nih.gov/ NCCAM is the USA “Federal Government's lead agency for scientific research on the diverse medical and health care systems, practices, and products that are not generally considered part of conventional medicine.” NCCAM “is dedicated to exploring complementary and alternative healing practices in the context of rigorous science, training CAM researchers, and disseminating authoritative information to the public and professionals.” The Resources for Health Care Providers section at http://nccam.nih.gov/health/providers/ includes: Educational Resources: including lectures, material for continuing education and data on CAM use; Evidence‐based Medicine: Results of NCCAM‐sponsored research and literature reviews of CAM modalities; Clinical Practice Guidelines: Abstracts and full‐text guidelines from other organizations; and For Patients: printable fact sheets for patients. -

Price List Price List
Price List Price List Energy – Intuitive Services: Massage Minutes: 60 /75/90 Energy Healing: Swedish $85 $105 $120 75/90/120 minutes $95/$115/$145 Therapeutic $90 $115 $130 Reiki, IET 60/75/90 mins :$85/100/135 Reiki & Sound Healing: 75 minutes $100 Deep Tissue/Sports $100 $125 $140 Chakra Balancing: 60 mins. $85 30 Minute Massage (1 area) Therapeutic $60 30 minute Massage (1 area) Deep Tissue $65 Reiki & Angel Card Reading Combo: 90mins.$140/ 2Hrs. $165 Integrative Treatment 75 or 90 mins. Energy Angel or Tarot Card Reading: work integrated with Massage 75 or 90 Bringing Complementary and minutes $125/$140 OR $135/$150 (Deep Tis- 45/60 minutes $70/$85 sue) Alternative Care to our HWC recognizes that everyone has a right to wear or not Pre -Natal Massage $95 $120 $140 wear a masn depending on their belief system & comfort Community...and Holistic Gift level. Because most of our staff are immune compromised, Hot Stone Therapeutic Massage $115/135/ 150 we are not able to provide service to clients not willing to Emporium! wear a masn in our store or for treatment. We have found 18 North Meadows rd., Unit 12B Hot Stone Deep Tissue Massage $120/140/160 with even the most anxious clients, that we are able to mane clients wearing masns comfortable so they can enjoy (Rt.27) their therapy. We appreciate your understanding . CBD or Far Infared Light enhancedMassage Medfield, MA 02052 Add $10 to any Treatment Foot Massage 30 min. $50 508 -359 -7400 www.Holisticwellnesscenter.0rg Foot Reflexology 30 mins $50 /45 - $60 [email protected] Foot Reflexology/Massage with Bio -Mat $70 Copyright 2020 Holistic Wellness Center, LLC. -

Gua-Sha: Application and Therapeutic Results in Musculoskeletal Pain Situations
BrJP. São Paulo, 2019 jul-sep;2(3):284-8 REVIEW ARTICLE Gua-sha: application and therapeutic results in musculoskeletal pain situations. Systematic review Gha-sha: aplicação e seus resultados terapêuticos em condições dolorosas musculoesqueléticas. Revisão sistemática Dérrick Patrick Artioli1, Gladson Ricardo Flor Bertolini2 DOI 10.5935/2595-0118.20190050 ABSTRACT RESUMO BACKGROUND AND OBJECTIVES: Gua-sha is a Tradi- JUSTIFICATIVA E OBJETIVOS: Gua-sha é uma técnica da tional Chinese Medicine technique, which consists of scraping Medicina Tradicional Chinesa, que consiste em raspar a pele the skin with a smooth and rounded edges object until the ap- com objeto de bordas lisas e arredondadas até o surgimento de pearance of petechiae. Used domestically in Asia, it is described petéquias. De uso doméstico na Ásia, é descrita como capaz de as capable of promoting the improvement of several conditions promover a melhora de uma série de afecções (ex. respiratórias, (e. g. respiratory, digestive, fever, and insomnia), such as painful digestivas, febre e insônia), como a de quadros dolorosos. Contu- conditions. However, there is a shortage of systematic reviews in do, há escassez de revisões sistemáticas a esse respeito na literatu- this respect in Western literature, so this study aimed to analyze ra ocidental, assim o objetivo deste estudo foi analisar a aplicação the common use of Gua-sha and the methodological quality of usual de Gua-sha e a qualidade metodológica dos estudos. the studies. CONTEÚDO: Foram consultadas as bases de dados PEDro, CONTENTS: The PEDro, Pubmed, Scielo and LILACS Da- Pubmed, Scielo e LILACS, buscando por ensaios clínicos com as tabases were consulted, searching for clinical trials with the seguintes palavras chaves e índice booleano: Gua-sha AND pain; following keywords and Boolean index: Gua-sha AND pain; Scraping therapy AND pain (inglês, português e espanhol). -

Spa Packages
WELCOME The Spa at Naples Grande provides a Quiet Environment variety of services focused on overall health enrichment through our modern and We strive to provide a tranquil and private innovative offerings. Your mind will relax, escape. As a courtesy to you and the rest of body rejuvenate, and soul be transformed. our guests we ask that you turn off your cell A Grande spa experience awaits. phones, electronic devices and cameras upon entering the spa. Arrival SPA PACKAGES Gratuities We invite you to enjoy the spa amenities on the day of any confirmed spa treatment and For your convenience, a 22% service charge is added to all spa and salon treatments. ask that you arrive at least 30 minutes in Spa Essentials | 2 Hours | $295 advance to allow proper time for checking in, Additional gratuities are at your discretion showering and enjoying spa amenities. and may be added upon request. Escape and indulge in our unique treatments to reduce stress and tension, while These amenities include our labyrinth, sun restoring peace and tranquility. This package includes your choice of any two deck, whirlpool, sauna, steam room and Cancellation & Rescheduling 50-minute Spa Services. meditation lounge. Your treatment will As a courtesy to you, other guests and start at its scheduled time and arriving late | 3 Hours | $440 service providers, we strictly adhere to Golden Trio will limit the time that you can enjoy your the spa cancellation policy: If you must Remove, restore, and radiate. Begin your experience with a 50-minute service. Should you like to enjoy these reschedule or cancel an appointment, Signature Muscle Melt Massage to relax, followed by a 50-minute amenities without booking a treatment please advise us eight (8) hours in advance Fijian Coconut Scrub to gently exfoliate your skin, and conclude with there is a separate charge based on daily to avoid being charged 100% of the availability. -

Fall 2020 Textbooks
Fall 2020 Textbooks Course Req or Pub Course Title ISBN-13 Title Author Edition Publisher ID Rec Price AC 101 Acupuncture Channels 978- Chinese Acupuncture and Cheng 3rd, 2010 Foreign Required $165 Pelzer and Points I 7119059945 Moxibustion (CAM) Language Press AC 101 Acupuncture Channels 978- Acupuncture A Comprehensive Bensky 1981 Eastland Required $75 Pelzer and Points I 0939616008 Text (Shanghai College of Press Traditional Medicine) AC 101 Acupuncture Channels 978- Manual of Acupuncture, A Deadman 2nd 2007 Eastland Required $150 Pelzer and Points I 0951054659 Press AC 101 Acupuncture Channels 978- Foundations of Chinese Maciocia 3rd, 2015 Churchill Required $175 Pelzer and Points I 0702052163 Medicine, The Livingston e AC 102 Acupuncture Channels 978- Chinese Acupuncture and Cheng 3rd, 2010 Foreign Required $165 Pelzer and Points II 7119059945 Moxibustion (CAM) Language Press AC 102 Acupuncture Channels 978- Acupuncture A Comprehensive Bensky 1981 Eastland Required $75 Pelzer and Points II 0939616008 Text (Shanghai College of Press Traditional Medicine) AC 102 Acupuncture Channels 978- Manual of Acupuncture, A Deadman 2nd 2007 Eastland Required $150 Pelzer and Points II 0951054659 Press AC 102 Acupuncture Channels 978- Foundations of Chinese Maciocia 3rd, 2015 Churchill Required $175 Pelzer and Points II 0702052163 Medicine, The Livingston e 1 6/22/2020 Fall 2020 Textbooks AC 104 Acupuncture Channels 978- Chinese Acupuncture and Cheng 3rd, 2010 Foreign Required $165 Pelzer and Points IV 7119059945 Moxibustion (CAM) Language Press -

6Th Biennial International Symposium on the BI-DIGITAL O-RING TEST
6th Biennial International Symposium ON THE BI-DIGITAL O-RING TEST FRIDAY August 6 – SUNDAY August 8, 2004 IBUKA AUDITORIUM INTERNATIONAL CONFERENCE HALL, WASEDA UNIVERSITY 1-20-14, NISHIWASEDA, SHINJYUKU-KU, TOKYO, JAPAN ORGANIZED BY: THE JAPAN BI-DIGITAL O-RING TEST MEDICAL SOCIETY JOINTLY SPONSORED BY: INTERNATIONAL COLLEGE OF ACUPUNCTURE & ELECTRO-THERAPEUTICS O-RING TEST LIFE SCIENCE RESEARCH INSTITUTE Inhibitory effect of Chinese parsley (Coriandrum sativum, Cilantro) on Drug-metabolizing Enzyme Induced by Endocrine Disrupters (Environmental Hormone) SHIGEHARU Fukuda Ph.D.1), YOSHINARI Honda2), TATSUYA Ishihara2), SHINPEI Ushio Ph.D. 2 ) ,KANSO Iwaki2 ) , MASAO Ikeda2 ) , MASASHI Kurimoto Ph.D. 2) , YASUHIRO Shimotsuura MD.,F.I.C.A.E., Cert. ORT-MD(5DAN) 3 ) , and YOSHIAKI Omura MD., Sc.D., F.I.C.A.E., FACA,FAAIM, FRSM 4) 1)Amase Institute and 2)Fujisaki Institute, Hayashibara Biochemical Laboratories Inc., Okayama City 3) Shimotsuura Clinic, Kurume City 4) Heart Disease Research Foundation, New York [Purpose] Omura discovered that the accumulation of mercury in tissues, particularly in cell nucleus, may be one of the main causes of cancer and he found that these metal deposits can be removed by using Chinese parsley and Omura’s Selective Drug Uptake Enhancement Method (1-4). In this report, the inhibitory effect of Chinese parsley on drug-metabolizing enzyme induced by endocrine disruptors (environmental hormone) and the identification of active components in Chinese parsley are described. [Materials and Methods] It is known that Dioxins taken in body bind to aryl hydrocarbon receptor (AhR) and cause the toxicity, carcinogenicity and teratogenicity by inducing the cytochrome P450 1A1 (CYP1A1), a kind of drug-metabolizing enzyme. -

Facial Gua Sha?
Contents 1. What Is Facial Gua Sha? ................................................................................................................................ 4 What are the benefits of facial gua sha? ......................................................................................................... 4 Why is the gua sha tool better than my fingers?.............................................................................................. 4 Is facial gua sha painful? ................................................................................................................................. 5 Does facial gua sha cause bruises? ................................................................................................................ 5 Why this tool? .................................................................................................................................................. 5 Is facial gua sha for me and my skin type? ..................................................................................................... 5 2. Know the Basics .............................................................................................................................................. 6 Acupressure Points ......................................................................................................................................... 6 Reflexology Zones.......................................................................................................................................... -
Natural Therapists Modalities Listing
Natural Therapists Modalities List: Modalities Listing 5 Rhythms Dancing Meditation Audiometrist Booty Barre 5 Tibetan Rites Aura‐Kinetic Training Bowen Therapy Acceptance and Commitment Therapy Aura‐Soma Brain Gym Access Consciousness Australian Bush Flowers Therapy Brandon Raynor Access the Bars Aviva Method Breast Feeding Consulting Accunect Ayurveda Healing Breath Enhancement Training Acupoint Therapy Ayurvedic Acupuncture Breath Work Active Release Technique Ayurvedic Lifestyle Consultation Brennan Healing Science Actively Ageing Consulting Bach Flower Remedies Building Biology Acu‐energetics Backpain Relief Reflexology Building Geobiology Acupoint Therapy Bai Shi Buteyko Breathing Method Acupressure Balance Awareness Training Calmbirth Acupuncture Barre Certified Transactional Analyst Acupuncture Point Injection Barre Attack Chakra Balancing African Drumming BarreCode Chakra Healing Af‐x Therapy Beamer Light Pen Chakradance Ageless Grace Behavioural Coach Chi Ball Ai Chi Belly Dancing Fitness Ajna Pineal Activation Light Therapy Chi Gong Bio Acoustical Utilisation Device (BAUD) Alcohol Screening Chi Nei Tsang Bio Impedance Analysis Alcohol Testing Chi Running Technique Biochemic Cell Salts Alexander Technique Chi Walking Biodynamic Craniosacral Therapy Allergy Consulting Chinese Herbal Medicine Bio‐Energetic Healing Allergy Testing Chinese Medicine Bio‐Energy Therapy Angel Intuitive Choice Theory Biofeedback Angelic Reiki Cholesterol Testing Biofrequency Animal Assisted Therapy Chonjo Bio‐Frequency Spectrum Animal Communication -

Wellness Spa Menu Buccaneer
The Buccaneer Spa Seaview Wellness Menu Buccaneer Seaview Spa Menu Focused Massage Therapy session 50 minutes - $120 Choose your Focus - Relax - Slow flow full body relaxation - Refresh - Neck, Back & feet focused - Rebuild - endurance with a sports focused massage - cross friction - focused on your fitness goals & target areas Immunity Massage 50 Minutes $135 Stimulate your lymphatic system - we apply immune boosting essential oils to help clean and clear your immune system. A light pressure lymphatic massage will be applied. Gua Sha Stone Massage 50 minutes $135 Deeper tissue massage without the pressure -Gua Sha stones help to loosen tight and restricted areas gently- this technique also flushes lymph to boost immunity. Facial Uplift Therapy - 20 minutes $120 Massage therapy techniques are implemented to uplift facial muscles, lesson tension, stimulate collagen - Gua sha - rose Quartz and a Jade roller help to reduce puffiness and tension. Express Back Massage - 20 minutes: $55 Express session. Neck & shoulders are massaged with Gua Sha stones to release tension and muscular restrictions. Mommy & Me Pregnancy Massage - 50 minutes $135 Massage for the mom to be! A gentle massage which will require extra support and side lying positions for safe practices. Relax as a light massage helps to relieve back and joint pain. Some contraindications may apply. Massage can be provided between 12 - 36 weeks. Honey can you rub my back! 50 minutes $140 Be ready for that big question - learn how to give your partner a back and neck massage! Learn how to find knots and & tension to help each other relax with a 1 to 1 massage lesson. -

The Effects of the Gua Sha Technique (Western View) on the Recuperation of Flexibility of the Posterior Chain in Parkinson: Case Study
European Journal of Research in Medical Sciences Vol. 4 No. 1, 2016 ISSN 2056-600X THE EFFECTS OF THE GUA SHA TECHNIQUE (WESTERN VIEW) ON THE RECUPERATION OF FLEXIBILITY OF THE POSTERIOR CHAIN IN PARKINSON: CASE STUDY Matheus de Siqueira Paulo Henrique Moraes Paulo Henrique Lima Mendes Barbalho Specialization in Kinesiology, State Rodrigues Physiotherapy and Physical University of Pará; Specialization in Physiotherapy, University Education, University of Acupuncture, Brazilian College of of Amazônia Amazônia, Pará. Systemic Studies; Physiotherapist, Estácio BRAZIL BRAZIL de Sá University, Rio de Janeiro; Physical Education, State University of Pará. BRAZIL ABSTRACT Introduction: The technique of Gua Sha is a method of traditional Chinese medicine (TCM), which has its origins in prehistory. In China, this technique was and is widely used by farmers. The beneficial effects of Gua Sha are due to simultaneous action on the skin, connective tissues, the lymphatic system, muscles, blood vessels and, lastly, the internal organs. Objectives: To present another new tool in the vast number of manual techniques that exist in the literature, always seeking the best care and patient satisfaction. Methodology: This study was subject to an elderly individual, carrier of Parkinson's disease. The study was conducted primarily by the patient's history. Later the individual was classified within the Hoehn and Yahr scale, being prerequisite to be between stages 1-3 of the disease. Results: After one treatment session using the Gua Sha, was notorious the patient improves. The data demonstrate that a gain flexibility by using a goniometer and test fingertip-to-Floor. In the test fingers to the ground, the patient was classified with reduced flexibility after the use of the technique the patient was classified with normal flexibility. -

Ayurvedic Inspired Wellness Menu
THEAYURVEDIC INSPIRED WELLNESS MENU sanarahotels.com Our Vision We believe in harnessing the power of nature, coupled with our own innate healing capabilities to support your vitality. Our world-class Wellness Center forms an integral part of the Sanará experience, both within our core Nourish & Heal immersive programs, and for our hotel guests and visitors. Our Independent therapists, as well as visiting alternative and complementary practitioners provide our guests with a wide range of treatment options, whether you are simply in need of deep relaxation or an energy boost, a complete rethink in your lifestyle, or are dealing with a health issue. Sanará also offers a range of spa treatments to soothe, relax and rejuvenate including: our signature Sanara Holistic Facial, pedicure, manicure, waxing, and other rejuvenation treatments. We source pure and natural ingredients for all our treatments and therapies and within our Daniella Hunter range of products which are available for purchase within the Wellness Center Boutique. Treatments and therapies are offered in one of our 4 treatment rooms, and many therapies may be taken in the privacy and comfort of your room, including massages, detox baths, and one-to-one counseling/consultations. “I believe that we are all walking a path towards true vitality and peace, and we have boundless, untapped energy and healing abilities if we give ourselves the blessing to explore the true essence of our Being.” DANIELLA HUNTER The mantra which flows through all aspects of our Sanara space, and team, is to care deeply for ourselves, and each other, while nurturing our world. All of our ingredients, products, practices, and therapies follow this philosophy, and we aim to minimize our environmental impact in all of our choices. -
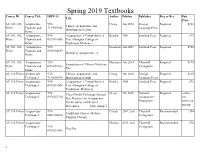
Spring 2019 Textbooks Course ID Course Title ISBN-13 Author Edition Publisher Req Or Rec Pub
Spring 2019 Textbooks Course ID Course Title ISBN-13 Author Edition Publisher Req or Rec Pub. Title Price AC 101, 103, Acupuncture 978- Cheng 3rd, 2010 Foreign Required $165 Chinese Acupuncture and Pelzer Channels and 7119059945 Language Press Moxibustion (CAM) Points AC 101, 103, Acupuncture 978- Acupuncture A Comprehensive Bensky 1981 Eastland Press Required $75 Pelzer Channels and 0939616008 Text (Shanghai College of Points Traditional Medicine) AC 101, 103, Acupuncture 978- Deadman 2nd 2007 Eastland Press Required $150 Pelzer Channels and 0951054659 Manual of Acupuncture, A Points AC 101, 103, Acupuncture 978- Maciocia 3rd, 2015 Churchill Required $175 Foundations of Chinese Medicine, Pelzer Channels and 0702052163 Livingstone The Points AC 110 Pelzer Acupuncture 978- Chinese Acupuncture and Cheng 3rd, 2010 Foreign Required $165 Technique I 7119059945 Moxibustion (CAM) Language Press AC 110 Pelzer Acupuncture 978- Acupuncture A Comprehensive Bensky 1981 Eastland Press Required $75 Technique I 0939616008 Text (Shanghai College of Traditional .Medicine) AC 110 Pelzer Acupuncture 978- Clean Needle Technique Manual: Given 7th, 2016 National Required online Technique I 0976253730 Best Practices for Acupuncture Acupuncture free Needle Safety and Related Foundation www.cca Procedures [title change] om.org AC 110 Pelzer Acupuncture 978- Chirali 2007, 2nd Churchill Recommended $94 Traditional Chinese Medince Technique I 0443102660 Livingstone Cupping Therapy AC 110 Pelzer Acupuncture Nielson 2013, 2nd Churchill Recommended $78 Technique I