Inflammatory Response Mechanisms of the Dentine–Pulp Complex And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
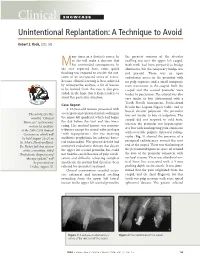
Clinical SHOWCASE Unintentional Replantation: a Technique to Avoid
Clinical SHOWCASE Unintentional Replantation: A Technique to Avoid Robert S. Roda, DDS, MS any times in a dentist’s career, he the greatest contour of the alveolar or she will make a decision that swelling was over the upper left cuspid. Mhas unintended consequences. In Both teeth had been prepared as bridge the case reported here, some quick abutments, but the temporary bridge was thinking was required to resolve the out- not present. There was an open come of an unexpected series of events. endodontic access in the premolar with Because clinical learning is best achieved no pulp exposure and a small composite by retrospective analysis, a list of lessons resin restoration in the cuspid. Both the to be learned from this case is also pro- cuspid and the second premolar were vided, in the hope that it helps readers to tender to percussion. The cuspid was also avoid this particular situation. very tender to bite (determined with a Tooth Slooth instrument, Professional Case Report Results Inc, Laguna Niguel, Calif.) and to A 63-year-old woman presented with buccal alveolar palpation. The premolar severe pain and extraoral facial swelling in The articles for this was not tender to bite or palpation. The the upper left quadrant, which had begun month’s “Clinical cuspid did not respond to cold tests, the day before the visit and was wors- Showcase” section were whereas the premolar was hyperrespon- ening. Her medical history was noncon- written by speakers sive but with nonlingering pain consistent at the 2006 CDA Annual tributory except for mitral valve prolapse with reversible pulpitis. -

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

Cracked Tooth Syndrome, an Update
International Journal of Applied Dental Sciences 2021; 7(2): 314-317 ISSN Print: 2394-7489 ISSN Online: 2394-7497 IJADS 2021; 7(2): 314-317 Cracked tooth syndrome, an update © 2021 IJADS www.oraljournal.com Received: 19-02-2021 Dariela Isabel Gonzalez-Guajardo, Guadalupe Magdalena Ramirez- Accepted: 21-03-2021 Herrera, Alejandro Mas-Enriquez, Guadalupe Rosalia Capetillo- Dariela Isabel Gonzalez-Guajardo Hernandez, Leticia Tiburcio-Morteo, Claudio Cabral-Romero, Rene Master in Sciences Student, Hernandez-Delgadillo and Juan Manuel Solis-Soto Universidad Autonoma de Nuevo Leon, Facultad de Odontologia, Monterrey, Nuevo Leon, CP 64460, DOI: https://doi.org/10.22271/oral.2021.v7.i2e.1226 Mexico Guadalupe Magdalena Ramirez- Abstract Herrera Introduction: Cracked tooth syndrome is defined as an incomplete fracture initiated from the crown and Professor, Universidad Autonoma de extending cervically, and sometimes gingivally, and is usually directed mesiodistally. Objective: To Nuevo Leon, Facultad de analyze the literature about cracked tooth syndrome, its etiology, prevalence, pulp involvement and Odontologia, Monterrey, Nuevo Leon, CP 64460, Mexico treatment. Methodology: Using the keywords “cracked tooth syndrome”, “etiology”, “prevalence”, “pulp Alejandro Mas-Enriquez involvement” and “treatment”, the MEDLINE/PubMed and ScienceDirect databases were searched, with Associate Professor, Universidad emphasis on the last 5 years. It was evaluated with the PRISMA and AMSTAR-2 guidelines. Autonoma de Nuevo Leon, Facultad de Odontologia, Monterrey, Nuevo Results: There are many causes for cracks, the main one being malocclusion. Another is due to Leon, CP 64460, Mexico restorations, pieces to which amalgam was placed due to the extension of the cavity for the retentions. The second lower molar presents more frequently fissures due to premature contact. -
Teeth What Do I Need to Know?
Teeth What do I Need to Know? Enamel Enamel is a semitranslucent, highly mineralized crystalline solid which covers the crowns of teeth and acts as a barrier to protect the teeth. Dentin Dentin is less mineralized than enamel, but more mineralized than bone; it acts as a cushion for the enamel and a further barrier to the pulp. Pulp Questions? The pulp is the area in the middle of the tooth containing the blood vessels and nerves for that tooth. If you would like more Pulp Horns information or have any The projections of the pulp underneath the taller parts of the tooth, or the “cusps.” specific questions, contact*: These are the areas of the pulp which are closest to the functional (or “occlusal”) part of the tooth which is used to chew food. Leslie Blackburn Cementum XLH [email protected] Protects the dentin and pulp of the roots the and way enamel protects it in the crown. or [email protected] My Teeth XLH Network contact: Raghbir Kaur, DMD; [email protected] Scientific Advisory Board *Please include XLH in the subject line of the email. Challenges Yale-New Haven Pediatric Dental Center 1 Long Wharf Dr, Suite 403, New Haven, CT 06510 Suggestions http://www.ynhh.org/medical-services/dental_pediatric.aspx What is the Most Important Thing to Know? It is not your fault. People with XLH have unique dental challenges. Sometimes even when you are doing everything right you may still have dental problems. While it is important to do everything you can to keep your mouth healthy, it is also important to remember that you some things about your oral health are out of your control. -

Orofacial Pain
QUINTESSENCE INTERNATIONAL OROFACIAL PAIN Noboru Noma Cracked tooth syndrome mimicking trigeminal autonomic cephalalgia: A report of four cases Noboru Noma DDS, PhD1/Kohei Shimizu DDS, PhD2/Kosuke Watanabe DDS3/Andrew Young DDS, MSD4/ Yoshiki Imamura DDS, PhD5/Junad Khan BDS, MSD, MPH, PhD6 Background: This report describes four cases of cracked All cases mimicked trigeminal autonomic cephalalgias, a group tooth syndrome secondary to traumatic occlusion that mim- of primary headache disorders characterized by unilateral icked trigeminal autonomic cephalalgias. All patients were facial pain and ipsilateral cranial autonomic symptoms. referred by general practitioners to the Orofacial Pain Clinic at Trigeminal autonomic cephalalgias include cluster headache, Nihon University Dental School for assessment of atypical facial paroxysmal hemicrania, hemicrania continua, and short-lasting pain. Clinical Presentation: Case 1: A 51-year-old woman unilateral neuralgiform headache attacks with conjunctival presented with severe pain in the maxillary and mandibular injection and tearing/short-lasting neuralgiform headache left molars. Case 2: A 47-year-old woman presented with sharp, attacks with cranial autonomic features. Pulpal necrosis, when shooting pain in the maxillary left molars, which radiated to caused by cracked tooth syndrome, can manifest with pain the temple and periorbital region. Case 3: A 49-year-old man frequencies and durations that are unusual for pulpitis, as was presented with sharp, shooting, and stabbing pain in the max- seen in these cases. Conclusion: Although challenging, dif- illary left molars. Case 4: A 38-year-old man presented with ferentiation of cracked tooth syndrome from trigeminal intense facial pain in the left supraorbital and infraorbital areas, autonomic cephalalgias is a necessary skill for dentists. -

Pulpotomy Treatment for Primary Teeth
2010 National Primary Oral Health Conference October 24-27 Gaylord Palm, Orlando, Florida Pulpotomy treatment for primary teeth Enrique Bimstein Professor of Pediatric Dentistry University of Florida College of Dentistry. Pulpotomy treatment for primary teeth Goal The participants will become familiar with the basic knowledge and procedures required for the performance of the pulpotomy treatment in primary teeth. Pulpotomy treatment for primary teeth Topics Introduction Definition and rationale. Indications and contraindications. Materials and techniques. Pulpotomy technique (clinical procedures). Pulpotomy follow up. Summary and conclusions. Pulpotomy treatment for primary teeth Topics Introduction Definition and rationale. Indications and contraindications. Materials and techniques. Pulpotomy technique (clinical procedures). Pulpotomy follow up. Summary and conclusions. Preservation of the primary teeth until their time of exfoliation is required to: a. Maintain arch length, masticatory function and esthetics. Preservation of the primary teeth until their time of exfoliation is required to: a. Maintain arch length, masticatory function and esthetics. Preservation of the primary teeth until their time of exfoliation is required to: a. Maintain arch length, masticatory function and esthetics. b. Eliminate pain, inflammation and infection. Preservation of the primary teeth until their time of exfoliation is required to: a. Maintain arch length, masticatory function and esthetics. b. Eliminate pain, inflammation and infection. c. Prevent any additional pain or damage to the oral tissues. Despite all the prevention strategies, childhood caries is still a fact that we confront every day in the clinic. The retention of pulpally involved primary teeth until the time of normal exfoliation remains to be a challenge. Primary teeth with cariously exposed vital pulps should be treated with pulp therapies that allow for the normal exfoliation process. -

Pulp Canal Obliteration After Traumatic Injuries in Permanent Teeth – Scientific Fact Or Fiction?
CRITICAL REVIEW Endodontic Therapy Pulp canal obliteration after traumatic injuries in permanent teeth – scientific fact or fiction? Juliana Vilela BASTOS(a) Abstract: Pulp canal obliteration (PCO) is a frequent finding associated (b) Maria Ilma de Souza CÔRTES with pulpal revascularization after luxation injuries of young permanent teeth. The underlying mechanisms of PCO are still unclear, (a) Universidade Federal de Minas Gerais - and no experimental scientific evidence is available, except the results UFMG, School of Dentistry, Department of Restorative Dentistry, Belo Horizonte, MG, of a single histopathological study. The lack of sound knowledge Brazil. concerning this process gives rise to controversies, including the (b) Pontifícia Universidade Católica de Minas most suitable denomination. More than a mere semantic question, Gerais – PUC-MG, Department of Dentistry, the denomination is an important issue, because it reflects the nature Belo Horizonte, MG, Brazil. of this process, and directly impacts the treatment plan decision. The hypothesis that accelerated dentin deposition is related to the loss of neural control over odontoblastic secretory activity is well accepted, but demands further supportive studies. PCO is seen radiographically as a rapid narrowing of pulp canal space, whereas common clinical features are yellow crown discoloration and a lower or non-response to sensibility tests. Late development of pulp necrosis and periapical disease are rare complications after PCO, rendering prophylactic endodontic intervention -

Cell Delamination in the Mesencephalic Neural Fold and Its
© 2013. Published by The Company of Biologists Ltd | Development (2013) 140, 4890-4902 doi:10.1242/dev.094680 RESEARCH ARTICLE Cell delamination in the mesencephalic neural fold and its implication for the origin of ectomesenchyme Raymond Teck Ho Lee1, Hiroki Nagai2, Yukiko Nakaya2, Guojun Sheng2, Paul A. Trainor3,4, James A. Weston5 and Jean Paul Thiery1,6,7,* ABSTRACT dorsal neural fold epithelia (Hörstadius, 1950) suggested that the The neural crest is a transient structure unique to vertebrate embryos neural crest is the source of multipotent stem cells that give rise to that gives rise to multiple lineages along the rostrocaudal axis. In a remarkable diversity of cell types, including pigment cells, neurons cranial regions, neural crest cells are thought to differentiate into and glia of the peripheral and enteric nervous systems. In addition, chondrocytes, osteocytes, pericytes and stromal cells, which are the neural crest was widely considered to be the source of collectively termed ectomesenchyme derivatives, as well as pigment mesenchymal connective tissues that entered the branchial arches to and neuronal derivatives. There is still no consensus as to whether form components of the craniofacial skeleton and connective tissue the neural crest can be classified as a homogenous multipotent of the dorsal fin at the trunk axial levels of fishes and amphibia population of cells. This unresolved controversy has important (Hörstadius, 1950; Le Douarin and Kalcheim, 1999; Raven, 1936). implications for the formation of ectomesenchyme and for Grafting studies in avian embryos (Le Douarin and Teillet, 1974; confirmation of whether the neural fold is compartmentalized into Nakamura and Ayer-le Lievre, 1982) suggested that developmental distinct domains, each with a different repertoire of derivatives. -

Six Cases Report of Differential Diagnosis of Periapical Diseases
Int J Oral Sci (2011) 3: 153-159. www.ijos.org.cn CLINICAL ARTICLE Six cases report of differential diagnosis of periapical diseases Wen-wei Xia, Ya-qin Zhu, Xiao-yi Wang* Department of Endodontics and Operative Dentistry, Shanghai Ninth People’s Hospital Affiliated Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China The distinction of some particular forms of periapical area, involving diseases from regular periapical disease, is a matter of considerable importance when choosing a correct treatment. The aim of this study is to describe the differential diagnosis of periapical diseases from six rare cases in clinical practice. The six rare cases are examples of situations where it is difficult to make a differential diagnosis in clinical practice. By retrospective surveys on the clinical examination, radiographs and pathological results, six patients referred to endodontic treatment in our department were analyzed for the accuracy of diagnosis and therapy. The pathoses of the six cases included two atypical radical cysts, periapical cemental dysplasia, cemento-ossifying fibroma, thymus cancer metastasis in the periapical site and tuberculosis. This report indicates that endodontists should be cognizant of a few particular circumstances when clinically treating periapical diseases. Keywords: periapical diseases; differential diagnosis; endodontic International Journal of Oral Science (2011) 3: 153-159. doi: 10.4248/IJOS11055 Introduction appear initially as periapical signs. Thus, early correct diagnosis of such patients was crucial for treatment and The periapical disease is one of the most prevalent subsequent prevention of advanced pathological process. diseases in general dental practice. However, because the The aim of this study is to describe the differential clinical diagnosis and treatment of periapical diseases is diagnosis on periapical diseases based on six rare cases. -

The Investigation of Major Salivary Gland Agenesis: a Case Report
Oral Pathology The investigation of major salivary gland agenesis: A case report T.A. Hodgson FDS, RCS, MRCP(UK) R. Shah FDS, RCS S.R. Porter MD, PhD, FDS, RCS, FDS, RCSE Dr. Hodgson is a specialist registrar and professor, and Dr. Porter is a consultant and head of department, Department of Oral Medicine; Dr. Shah is senior house officer, Department of Pediatric Dentistry , Eastman Dental Institute for Oral Health Care Sciences, University College London. Correspond with Dr. Hodgson at [email protected] Abstract Salivary gland agenesis is an extremely uncommon congenital The present report details a child with rampant dental car- anomaly, which may cause a profound xerostomia in children. The ies secondary to xerostomia. Despite having oral disease for oral sequelae includes dental caries, candidosis, and ascending many years, the congenital absence of all the salivary glands sialadenitits. failed to be established until late adolescence, and, therefore, The present report details a child with rampant dental caries appropriate replacement therapy was not instituted, until this secondary to xerostomia. Despite having oral disease for many years, time, to prevent further oral disease. the congenital absence of all the salivary glands failed to be estab- lished until early adulthood. Case report The appropriate investigation and management of the In 1988, a 41/2-year-old Caucasian female was referred to the xerostomic child allows a definitive diagnosis to be made and at- Department of Pediatric Dentistry of the Eastman Dental In- tention focused on the prevention and treatment of resultant oral stitute for Oral Health Care Sciences for the extraction of disease. -

A Review of Prolonged Post-COVID-19 Symptoms and Their Implications on Dental Management
International Journal of Environmental Research and Public Health Review A Review of Prolonged Post-COVID-19 Symptoms and Their Implications on Dental Management Trishnika Chakraborty 1,2 , Rizwana Fathima Jamal 3 , Gopi Battineni 4 , Kavalipurapu Venkata Teja 5 , Carlos Miguel Marto 6,7,8,9 and Gianrico Spagnuolo 10,11,* 1 Department of Conservative Dentistry and Endodontics, Chaudhary Charan Singh University, Meerut, Uttar Pradesh 250001, India; [email protected] 2 Department of Health System Management, Ben-Gurion University of Negev, Beer-Sheva 8410501, Israel 3 Department of Oral and Maxillofacial Surgery, Chettinad Dental College and Research Institute, Kancheepuram, Tamil Nadu 603103, India; [email protected] 4 Telemedicine and Tele Pharmacy Center, School Medicinal and Health Products Sciences, University of Camerino, 62032 Camerino, Italy; [email protected] 5 Department of Conservative Dentistry & Endodontics, Saveetha Dental College & Hospitals, Saveetha Institute of Medical & Technical Sciences, Saveetha University, Chennai, Tamil Nadu 600077, India; [email protected] 6 Faculty of Medicine, Institute of Experimental Pathology, University of Coimbra, 3004-531 Coimbra, Portugal; [email protected] 7 Faculty of Medicine, Coimbra Institute for Clinical and Biomedical Research (iCBR), University of Coimbra, Area of Environment Genetics and Oncobiology (CIMAGO), 3000-548 Coimbra, Portugal 8 Centre for Innovative Biomedicine and Biotechnology (CIBB), University of Coimbra, 3004-504 Coimbra, Portugal 9 Clinical Academic Center of Coimbra (CACC), 3004-531 Coimbra, Portugal 10 Department of Neurosciences, Reproductive and Odontostomatological Sciences, University of Naples “Federico II”, 80131 Napoli, Italy Citation: Chakraborty, T.; Jamal, R.F.; 11 Institute of Dentistry, I. M. Sechenov First Moscow State Medical University, 119435 Moscow, Russia Battineni, G.; Teja, K.V.; Marto, C.M.; * Correspondence: [email protected] Spagnuolo, G. -

Clinical Diagnosis of Herpes Zoster Presenting As Odontogenic Pain
대한치과보존학회지: Vol. 33, No. 5, 2008 Clinical Diagnosis of Herpes Zoster Presenting as Odontogenic Pain Seong-Hak Yang, Dong-Ho Jung, Hae-Doo Lee, Yoon Lee, Hoon-Sang Chang, Kyung-San Min* Department of Conservative Dentistry, College of Dentistry, Wonkwang University ABSTRACT Herpes zoster, an acute viral infection produced by the varicella zoster virus, may affect any of the trigeminal branches. This case report presents a patient with symptoms mimicking odontogenic pain. No obvious cause of the symptoms could be found based on clinical and radiographic examinations. After a dermatologist made a diagnosis of herpes zoster involving the third trigeminal branch, the patient was given antiviral therapy. Two months later, the facial lesions and pain had almost disap- peared, and residual pigmented scars were present. During the diagnostic process, clinicians should keep in mind the possibility that orofacial pain might be related to herpes zoster. [J Kor Acad Cons Dent 33(5):452-456, 2008] Key words : Herpes zoster, Trigeminal nerve, Odontogenic pain - Received 2008.7.2., revised 2008.8.4., accepted 2008.8.25- Ⅰ. INTRODUCTION affected by the reactivation of the latent herpes zoster virus the most. The first division of the Diagnostic assessment in patients with orofacial trigeminal nerve is commonly affected, whereas pain may be challenging due to the close proximi- the second and third divisions are rarely ty between the teeth and other orofacial tissues, involved4). If the third division of the trigeminal and symptoms associated with neurological disor- nerve is affected, it may be characterized by pul- ders. Herpes zoster (shingles) is caused by the pitis in the mandibular molars and vesicular skin reactivation of the latent varicella-zoster virus eruptions in the affected sensory nerve area.