International Consolidated Venous Ulcer Guideline (ICVUG) 2015 (Update of AAWC Venous Ulcer Guideline, 2005 and 2010)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Arterial Leg Ulcer Clinical Pathway
Waterloo Wellington Integrated Wound Care Program Evidence-Based Wound Care Arterial Leg Ulcer Clinical Pathway 0-7 Days Expected Outcomes Notes Most Responsible Physician(MRP)/Nurse Practitioner (NP) Refer patient to ‘Care Connects’ if no responsible practitioner currently involved with patient identified/informed Determine if MRP/NP is part of Family Health Team (FHT) or Community Health Centre (CHC) and consider additional supports available Medical/surgical history and co-morbidity management Risk factors include: Chronic renal disease considered within care plan Smoking Congestive heart failure Diabetes mellitus Impaired liver function Hyperlipidemia Use of systemic steroids, Hypertension immunosuppressive and chemotherapy Coronary artery disease >70 years of age History of cerebral vascular accident Age 50-69 years with history of diabetes (CVA) or smoking Low hemoglobin < 50 years with diabetes and one other Obesity atherosclerotic factor Poor nutrition History of vascular surgery or deep vein Decreased thyroid function thrombosis Psoriasis Bleeding disorders Autoimmune diseases Family history of arterial disease Medication reconciliation and their impact on wound healing Prescription, non-prescription, naturopathic and illicit drug use (including e-cigarettes, reviewed inhaled substances and nicotine replacement therapy) Medications that can affect healing include: chemotherapy, anticoagulants, antiplatelets, corticosteroids, vasoconstrictors, antihypertensives, diuretics and immunosepressive drugs Other -

Wound Bed Preparation: TIME in Practice
Clinical PRACTICE DEVELOPMENT Wound bed preparation: TIME in practice Wound bed preparation is now a well established concept and the TIME framework has been developed as a practical tool to assist practitioners when assessing and managing patients with wounds. It is important, however, to remember to assess the whole patient; the wound bed preparation ‘care cycle’ promotes the treatment of the ‘whole’ patient and not just the ‘hole’ in the patient. This paper discusses the implementation of the wound bed preparation care cycle and the TIME framework, with a detailed focus on Tissue, Infection, Moisture and wound Edge (TIME). Caroline Dowsett, Heather Newton dependent on one another. Acute et al, 2003). Wound bed preparation wounds usually follow a well-defined as a concept allows the clinician to KEY WORDS process described as: focus systematically on all of the critical Wound bed preparation 8Coagulation components of a non-healing wound to Tissue 8Inflammation identify the cause of the problem, and Infection 8Cell proliferation and repair of implement a care programme so as to Moisture the matrix achieve a stable wound that has healthy 8Epithelialisation and remodelling of granulation tissue and a well vascularised Edge scar tissue. wound bed. In the past this model of healing has The TIME framework been applied to chronic wounds, but To assist with implementing the he concept of wound bed it is now known that chronic wound concept of wound bed preparation, the preparation has gained healing is different from acute wound TIME acronym was developed in 2002 T international recognition healing. Chronic wounds become ‘stuck’ by a group of wound care experts, as a framework that can provide in the inflammatory and proliferative as a practical guide for use when a structured approach to wound stages of healing (Ennis and Menses, managing patients with wounds (Schultz management. -

Understand Your Chronic Wound
Patient Information Leaflet Understanding your Chronic Wound Dressings, management and wound infection In this leaflet Health Care Professional (HCP) refers to any member of the team involved in your wound care. This can include treatment room or practice nurse, community, ward or clinic nurse, GP or hospital doctor, podiatrist etc. Chronic Wounds and Dressings What is a Chronic wound? A wound with slow progress towards healing or shows delayed healing. This may be due to underlying issues such as: • Poor blood flow and less oxygen getting to the wound • Other health conditions • Poor diet, smoking, pressure on the wound e.g. footwear/seating. Can my wound be left open to the air? No, the evidence shows that wounds heal better when the surface is kept moist (not too wet or dry). The moisture provides the correct environment to aid your wound to heal. Does my dressing need changed daily? Not usually, your HCP will explain how often it needs changed. This will depend on the level of fluid leaking from your wound. Some dressings can be left in place up to a week. Most wounds have a slight odour, but if a wound smells bad it could be a sign that something is wrong. See section on wound infection. Your dressing may indicate that it needs changed when the dark area in the centre gets close to the edge of the dressing pad. The dark area is fluid from your wound, this is normal. It will be dry to touch. Let your HCP know if your dressing needs changed before your next visit or appointment is due. -
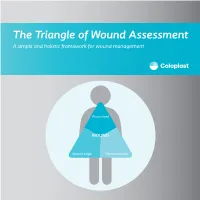
The Triangle of Wound Assessment a Simple and Holistic Framework for Wound Management
The Triangle of Wound Assessment A simple and holistic framework for wound management Wound bed WOUND Wound edge Periwound skin We asked healthcare professionals around the world about their priorities ? for wound care We found that most people Respondents said that treating wounds are not protecting the periwound specialists in a hospital1 skin is very important1 Approximately Up to 79% of wounds are 70% of being treated in wounds are the community2 surrounded by unhealthy skin3 2 ...none However, in a recent met all of the study of 14 wound criteria for assessment tools ... optimal wound assessment4 The Triangle of Wound Assessment is a holistic framework that allows practitioners üto assess and manage all areas of the wound, including the periwound skin. It is a simple and systematic approach that guides the user Wound bed from complete wound WOUND assessment to setting management goals, and Wound edge Periwound skin selecting the optimal treatment. 3 The Triangle of Wound Assessment offers a systematic approach to wound management Optimal wound management starts with a holistic wound assessment. This will help to more efficiently set management goals, which will increase the potential for better treatment outcomes. Assessment Management Goals Treatment 4 This is achieved through a holistic framework The Triangle of Wound Assessment provides a framework to assess all three areas of the wound while remembering the patient behind the wound within their social context. Patient Wound bed Social context WOUND Wound Wound edge Periwound skin 5 It’s not just about the wound but also the patient behind the wound Optimal management of the wound starts with assessing the patient behind the wound, and the social context in which the patient lives. -

Guideline: Wound Bed Preparation for Healable and Non Healable Wounds
British Columbia Provincial Nursing Skin and Wound Committee Guideline: Wound Bed Preparation for Healable and Non Healable Wounds Developed by the BC Provincial Nursing Skin and Wound Committee in collaboration with Wound Clinicians from: / TITLE Guideline: Wound Bed Preparation for Healable and Non-Healable Wounds in Adults & Children1 Practice Level Nurses in accordance with health authority and agency policy. Conservative sharp wound debridement (CSWD) is a restricted activity according to the Nurse’s (Registered) and Nurse Practitioner Regulation. 2 CRNBC states that registered nurses must successfully complete additional education and follow an established guideline when carrying out CSWD. Biological debridement therapy is a restricted activity according to the Nurse’s (Registered) and Nurse Practitioner Regulation. 3 CRNBC states that registered nurses must follow an established guideline when carrying out biological debridement. Clients 4 with wounds needing wound bed preparation require an interprofessional approach to provide comprehensive, evidence-based assessment and treatment. This clinical practice guideline focuses solely on the role of the nurse, as one member of the interprofessional team providing care to these clients. Background Factors affecting wound healability include the presence of adequate circulation in the area of the wound, wound related factors such as the size and duration of the wound, the ability to treat the cause of the wound and the presence of risk factors impacting wound healing. While many wounds heal, others are determined to be non-healing or slow-to-heal based on the presence or absence of these factors. Wound healability must be determined prior to debridement and moist wound healing. Although wound healing normally occurs in a predictable fashion, wound healing trajectories can be heterogeneous and non- uniform resulting is delayed wound healing for some clients. -

Reactive Oxygen Species (ROS)
EuropeanN Bryan etCells al. and Materials Vol. 24 2012 (pages 249-265) Reactive DOI: 10.22203/eCM.v024a18oxygen species in inflammation and ISSN wound 1473-2262 healing REACTIVE OXYGEN SPECIES (ROS) – A FAMILY OF FATE DECIDING MOLECULES PIVOTAL IN CONSTRUCTIVE INFLAMMATION AND WOUND HEALING Nicholas Bryan1*, Helen Ahswin2, Neil Smart3, Yves Bayon2, Stephen Wohlert2 and John A. Hunt1 1Clinical Engineering, UKCTE, UKBioTEC, The Institute of Ageing and Chronic Disease, University of Liverpool, Duncan Building, Daulby Street, Liverpool, L69 3GA, UK 2Covidien – Sofradim Production, 116 Avenue du Formans – BP132, F-01600 Trevoux, France 3Royal Devon & Exeter Hospital, Barrack Road, Exeter, Devon, EX2 5DW, UK Abstract Introduction Wound healing requires a fine balance between the positive The survival and longevity of any animal requires an active and deleterious effects of reactive oxygen species (ROS); vigilant set of defence mechanisms to combat infection, a group of extremely potent molecules, rate limiting in efficiently repair damaged tissue and remove debris successful tissue regeneration. A balanced ROS response associated with apoptotic/necrotic cells. Compromised will debride and disinfect a tissue and stimulate healthy tissue rapidly results in decreased mobility, organ failures, tissue turnover; suppressed ROS will result in infection hypovolaemia, hypermetabolism, and ultimately infection and an elevation in ROS will destroy otherwise healthy and sepsis. Therefore, mammals have evolved an array stromal tissue. Understanding and anticipating the ROS of physiological pathways and mechanisms that enable niche within a tissue will greatly enhance the potential to damaged tissue to return to a basal homeostatic state. In exogenously augment and manipulate healing. an ideal scenario this occurs without compromise of tissue Tissue engineering solutions to augment successful mechanics, scarring or incorporation of microbial material. -

The Role of Antioxidants on Wound Healing: a Review of the Current Evidence
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 15 July 2021 doi:10.20944/preprints202107.0361.v1 Review THE ROLE OF ANTIOXIDANTS ON WOUND HEALING: A REVIEW OF THE CURRENT EVIDENCE. Inés María Comino-Sanz 1*, María Dolores López-Franco1, Begoña Castro2, Pedro Luis Pancorbo-Hidalgo1 1 Department of Nursing, Faculty of Health Sciences, University of Jaén, 23071 Jaén (Spain); [email protected] (IMCS); MDLP ([email protected]); PLPH ([email protected]). 2 Histocell S.L., Bizkaia Science and Technology Park, Derio, Bizkaia (Spain); [email protected] * Correspondence: [email protected]; Tel.: +34-953213627 Abstract: (1) Background: Reactive oxygen species (ROS) play a crucial role in the preparation of the normal wound healing response. Therefore, a correct balance between low or high levels of ROS is essential. Antioxidant dressings that regulate this balance is a target for new therapies. The pur- pose of this review is to identify the compounds with antioxidant properties that have been tested for wound healing and to summarize the available evidence on their effects. (2) Methods: A litera- ture search was conducted and included any study that evaluated the effects or mechanisms of an- tioxidants in the healing process (in vitro, animal models, or human studies). (3) Results: Seven compounds with antioxidant activity were identified (Curcumin, N-acetyl cysteine, Chitosan, Gallic Acid, Edaravone, Crocin, Safranal, and Quercetin) and 46 studies reporting the effects on the healing process of these antioxidants compounds were included. (4) Conclusions: These results highlight that numerous novel investigations are being conducted to develop more efficient systems for wound healing activity. The application of antioxidants is useful against oxidative damage and ac- celerates wound healing. -

A Focus on the Triangle of Wound Assessment — Addressing the Gap Challenge and Identifying Suspected Biofilm in Clinical Practice
Clinical practice A focus on the Triangle of Wound Assessment — addressing the gap challenge and identifying suspected biofilm in clinical practice Authors: Wound assessment should be comprehensive, systematic and evidence- Caroline Dowsett, Terry Swanson and Tonny Karlsmark based (World Union of Wound Healing Societies [WUWHS], 2016a). The Triangle of Wound Assessment offers clinicians a framework to assess the patient and their wound, taking into consideration the wound bed, wound edge and periwound skin (Dowsett et al, 2015). The framework can be adapted to incorporate new developments and new challenges in wound care such as the ‘gap challenge’ and biofilm prevention and management. Using the framework can assist in determining the status of the wound bed and support clinical decision making to prevent problems associated with exudate pooling at the wound bed and the potential for biofilm formation. he Triangle of Wound Assessment This article will discuss how the Triangle of was established in 2014 and provides Wound Assessment identifies infection and T a systematic approach to wound biofilm, tackles the gap challenge, and how assessment and in setting management goals, this framework can be developed for new to guide optimal treatment choice (Dowsett et challenges in wound care. al, 2015), ensuring that the periwound skin is incorporated into the assessment. Periwound The importance of holistic assessment skin can be a significant problem in patients Wounds are a significant source of cost to with chronic wounds, with between 60–70% patients, as well as to the health economy. of wounds found to be surrounded by either Chronic wounds are often hard to heal problematic or unhealthy periwound skin resulting in a cycle of pain, anxiety and (Cartier et al, 2014). -

Association Between Hemorrhoids and Lower Extremity Chronic Venous Insufficiency
Open Access Original Article DOI: 10.7759/cureus.4502 Association Between Hemorrhoids and Lower Extremity Chronic Venous Insufficiency Ugur Ekici 1 , Abdulcabbar Kartal 2 , Murat F. Ferhatoglu 2 1. General Surgery, Istanbul Gelişim University, Istanbul, TUR 2. General Surgery, Okan University Medical Faculty, Istanbul, TUR Corresponding author: Abdulcabbar Kartal, [email protected] Disclosures can be found in Additional Information at the end of the article Abstract Aim The aim of the present study was to evaluate the incidence of varicose veins among patients with hemorrhoidal disease and to compare its incidence reported in various community-based studies. Method The study group comprised of 100 patients who underwent surgery for symptomatic internal or external hemorrhoids; the control group consisted of 100 volunteers who received no prior therapy for hemorrhoidal disease and lacked any symptoms or findings suggestive of this condition. Subjects in both the groups were inquired with respect to their demographic data and risk factors. Both groups were asked to stand for two minutes before performing leg examinations while still in the standing position. The findings were recorded for both the groups. Varicose veins were classified according to the clinical appearance section of the Clinical, Etiologic, Anatomic, and Pathophysiologic (CEAP) classification that was developed by the 1994 American Venous Forum. Results There was no significant difference between the two groups with respect to age and body mass index (BMI). Significant relationships were identified between the groups with respect to the incidence of varicose veins and chronic constipation. The incidence of C1 and C2 varicose veins observed in the study group was higher than that observed in the control group. -

Treatment Strategies for Patients with Lower Extremity Chronic Venous Disease (LECVD)
Evidence-based Practice Center Systematic Review Protocol Project Title: Treatment Strategies for Patients with Lower Extremity Chronic Venous Disease (LECVD) Project ID: DVTT0515 Initial publication date if applicable: March 7, 2016 Amendment Date(s) if applicable: May 6th, 2016 (Amendments Details–see Section VII) I. Background for the Systematic Review Lower extremity chronic venous disease (LECVD) is a heterogeneous term that encompasses a variety of conditions that are typically classified based on the CEAP classification, which defines LECVD based on Clinical, Etiologic, Anatomic, and Pathophysiologic parameters. This review will focus on treatment strategies for patients with LECVD, which will be defined as patients who have had signs or symptoms of LE venous disease for at least 3 months. Patients with LECVD can be asymptomatic or symptomatic, and they can exhibit a myriad of signs including varicose veins, telangiectasias, LE edema, skin changes, and/or ulceration. The etiology of chronic venous disease includes venous dilation, venous reflux, (venous) valvular incompetence, mechanical compression (e.g., May-Thurner syndrome), and post-thrombotic syndrome. Because severity of disease and treatment are influenced by anatomic segment, LECVD is also categorized by anatomy (iliofemoral vs. infrainguinal veins) and type of veins (superficial veins, perforating veins, and deep veins). Finally, the pathophysiology of LECVD is designated typically as due to the presence of venous reflux, thrombosis, and/or obstruction. LECVD is common -

Original Article
Original Article Is chronic venous ulcer curable? A sample survey of a plastic surgeon V. Alamelu Department of Plastic, Reconstructive and Faciomaxillary Surgery, Madras Medical College and Govt General Hospital, Chennai - 600 003; Sri Jayam Hospital, West Tambaram, Chennai - 600 045; K.J. Hospital and Research Foundation, Poonamallee High Road, Chennai - 600 084, India Address for correspondence: Dr. V. Alamelu, 23, Ramakrishnan Street, West Tambaram, Chennai-600 045, India. E-mail: [email protected] ABSTRACT Introduction: Venous ulcers of lower limbs are often chronic and non-healing, many a time neglected by patients and their treating physicians as these ulcers mostly do not lead to amputation as in gangrenous arterial ulcer and also cost much to complete the course of treatment and prevention of recurrence. Materials and Methods: One hundred and twenty two lower limb venous ulcers came up for treatment between May 2006 and April 2009. Only twenty nine cases completed the treatment. The main tool of investigation was the non invasive Duplex scan venography. Biopsy of the ulcer was done for staging the disease. Patients’ choice of treatment was always conservative and as out-patient instead of hospitalisation and surgery, which required a lot of motivation by the treating unit. Results: Out of twenty nine cases, ten cases were treated conservatively and seven (24.13%) healed well. Remaining nineteen cases were given surgical modality in which fifteen cases (51.74%) were successful. Only seven cases (24.13%) failed to heal. Compression stockings were advised to control oedema, varices and pain. Foot care, regular exercises and follow-up were stressed effectively. -
Venous Ulcer Assessment and Management: Using the Updated CEAP Classification System
Practice Points Venous Ulcer Assessment and Management: Using the Updated CEAP Classification System Cathy Thomas Hess, BSN, RN, CWCN ylastcolumn,Classification of Pressure Injuries, Although most leg ulcers are venous ulcers, the clini- discussed the importance of documenting the cian should suspect other causes when the wound looks details of pressure injuries using the updated atypical (presence of necrotic tissue, exposed tendon, M pressure injury classification system. This livedo reticularis on surrounding skin, or a deep, column discusses the updated classification system for “punched-out” ulcer), has been present for longer than venous ulcers, namely, the Clinical Etiology Anatomy 6 months, or has not responded to good care. Do not Pathophysiology (CEAP) classification system. To under- hesitate to take a biopsy when in doubt. stand the use of this classification, let’sbrieflydiscussthe Visual and palpable assessment may not be enough etiology, assessment, and management of venous ulcers. to determine the next steps. Objective testing may be needed to confirm the diagnosis, determine the etiology ETIOLOGY of the problem, and identify the anatomic site and sever- Venous ulcers are believed to account for approximately ity of disease pathway (Table). 70% to 90% of chronic leg ulcers.1 The incidence of ve- nous ulceration increases with age, and women are three times more likely than men to develop venous leg ulcers.2 Table. CLINICAL FINDINGS ASSOCIATED WITH VENOUS In some studies, 50% of patients had venous ulcers that LEG ULCERS persisted for more than 9 months, and 20% had ulcers Wound location 30%–40% occur superior to the medial malleolus (near the that did not heal for more than 2 years.